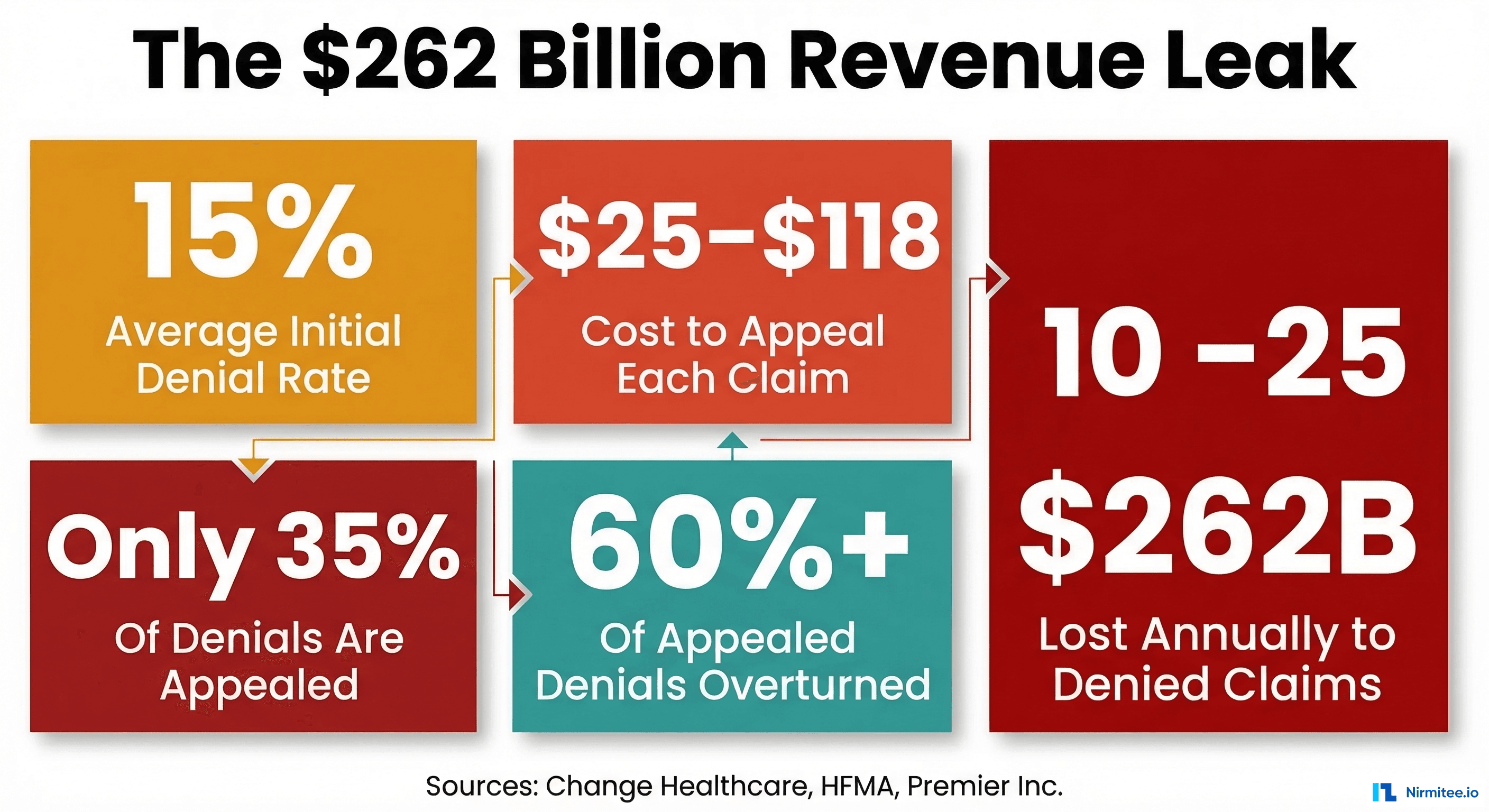
Every revenue cycle director knows the feeling: opening the monthly denials report and watching the numbers climb. Again. Initial denial rates have crossed 15% industry-wide. The average cost to appeal a single claim runs between $25 and $118. And here is the statistic that should keep every CFO awake: up to 65% of denied claims are never even resubmitted. They are simply written off.
According to a Change Healthcare analysis, $262 billion in medical claims are initially denied each year in the United States alone. That is not a billing inconvenience. That is a systemic failure that threatens the financial viability of health systems across the country.
But here is what makes this problem solvable in 2026: AI agents. Not chatbots. Not dashboards that show you prettier versions of the same bad news. Autonomous software agents that parse remittance files, classify denial root causes, extract clinical evidence, and draft payer-ready appeal letters, all before your staff finishes their morning coffee.
McKinsey's research on agentic AI in revenue cycle shows these systems can process claims 4-5x faster than manual workflows while cutting per-claim costs by up to 80%. This is not theoretical. Health systems are deploying these agents today.
This article breaks down exactly how to build a denial management agent system, from X12 835 parsing to automated appeal generation, with the architecture, denial code interpretation, and ROI math you need to make the business case.
The Denial Crisis: A $262 Billion Revenue Leak
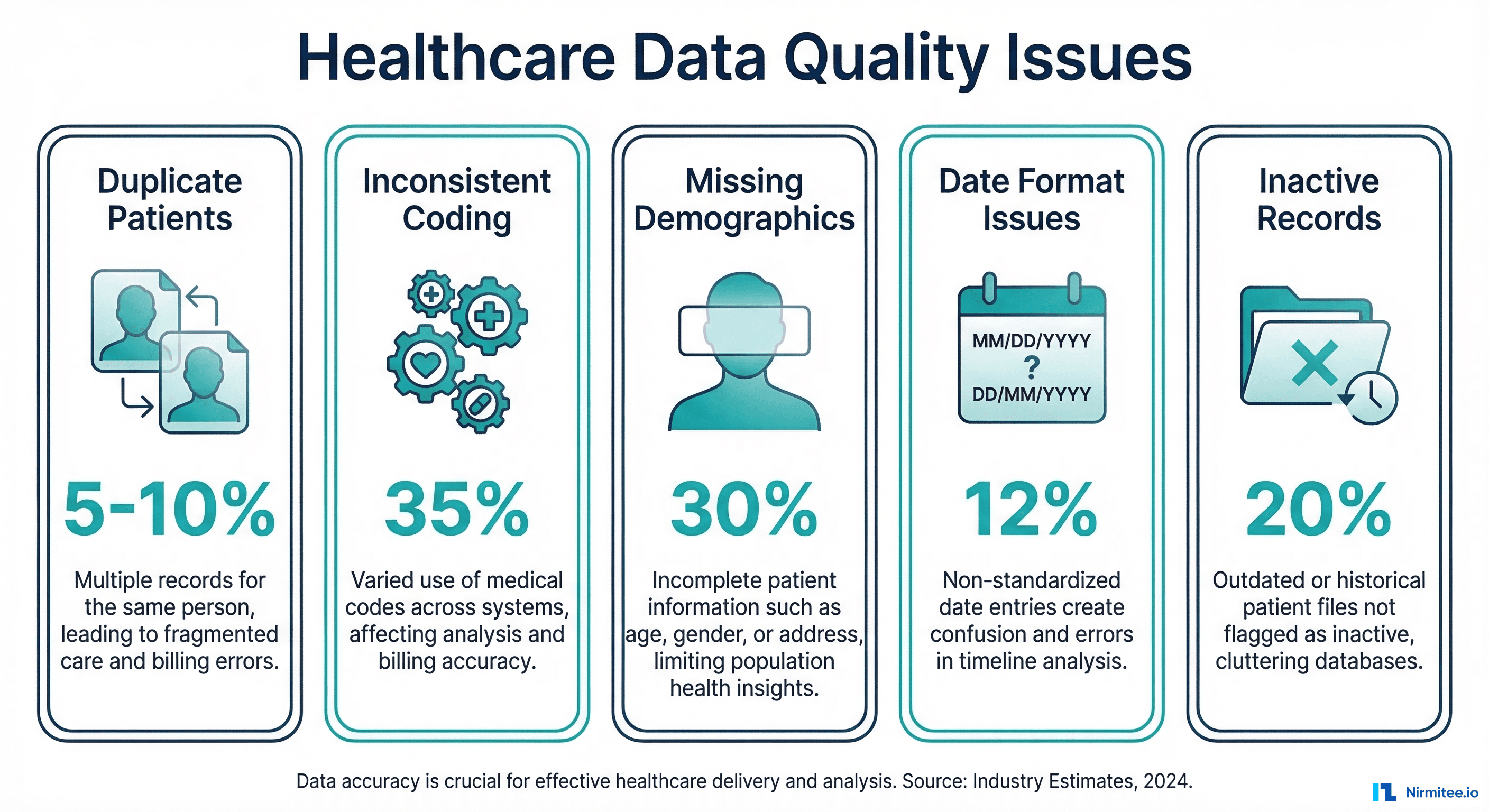
Before building the solution, let us quantify the problem precisely. The denial landscape in 2025-2026 looks like this:
- 15% average initial denial rate across private payers, with Medicare Advantage averaging 15.7% and commercial payers at 13.9%, according to Experian Health's 2025 State of Claims report
- $25-$118 cost per appeal, with the average administrative cost per denied claim reaching $57.23 in 2023, up from $43.84 the year prior (Premier Inc.)
- Only 35-40% of denied claims are appealed, meaning the majority of recoverable revenue is abandoned
- 60%+ overturn rate on appeals when they are actually filed, with 62% of prior authorization denials and 50% of initial claim denials reversed on appeal (AHA)
- $4.9 million average annual denials per hospital, representing roughly 3.3% of net patient revenue
The math is devastating: if 60% of appeals succeed, but you only appeal 35% of denials, you are voluntarily leaving millions on the table every year. The bottleneck is not medical merit. It is operational capacity. Your staff cannot physically review, research, draft, and submit appeals fast enough.
This is exactly the kind of problem AI agents are built to solve. Not the judgment calls. The throughput problem. If you are exploring where AI agents fit into your revenue cycle workflows, our guide on finding the 3-5 workflows that should be AI agents is a useful starting point.
Agent 1: Denial Root Cause Classification
The first agent in the pipeline is the denial classifier. When an X12 835 Electronic Remittance Advice arrives from a payer, this agent parses the file, extracts every Claim Adjustment Segment (CAS), and cross-references the denial reason codes against the original 837 claim submission.
How X12 835 Parsing Works
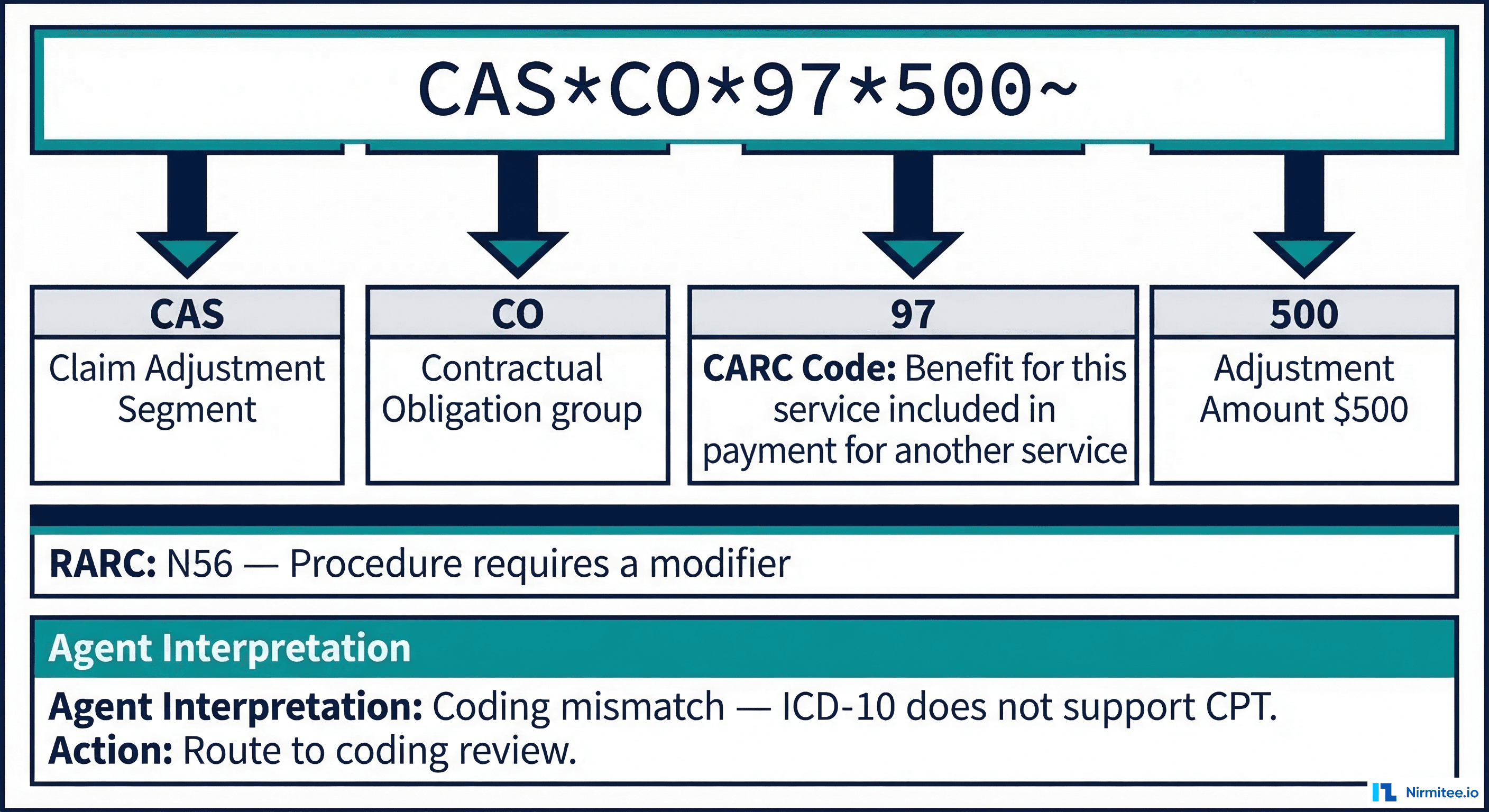
The 835 transaction set contains structured segments that encode exactly why a claim was adjusted. The agent must interpret three key code sets:
- Claim Adjustment Group Codes: CO (Contractual Obligation), OA (Other Adjustment), PI (Payer Initiated), PR (Patient Responsibility). These determine who bears the financial impact.
- CARC (Claim Adjustment Reason Codes): 300+ standardized codes that specify the exact reason. For example, CARC 197 means "precertification/authorization/notification absent," while CARC 50 means "non-covered service."
- RARC (Remittance Advice Remark Codes): Supplemental codes that provide additional context, like N56 ("Procedure requires a modifier") or N386 ("This decision was based on a Local Coverage Determination").
A Real 835 Denial Example
Consider this CAS segment from an 835 remittance:
CLP*CLAIM12345*4*1500*0*0*MC*REF123~
CAS*CO*197*1500~
CAS*CO*16*0~
SVC*HC:99214*1500*0*1~
LQ*HE*N657~The agent interprets this as follows:
CLP*...*4: Claim status 4 = DeniedCAS*CO*197*1500: Contractual Obligation, CARC 197 = Precertification/authorization absent, $1,500 adjustmentCAS*CO*16*0: CARC 16 = Claim/service lacks information needed for adjudicationLQ*HE*N657: RARC N657 = "Authorization was not obtained prior to service"
The classifier agent maps this combination to: Prior Authorization denial — authorization not obtained before date of service. It tags the claim as "auth_missing," sets priority to high (based on claim value), and routes it to the authorization-specific appeal workflow.
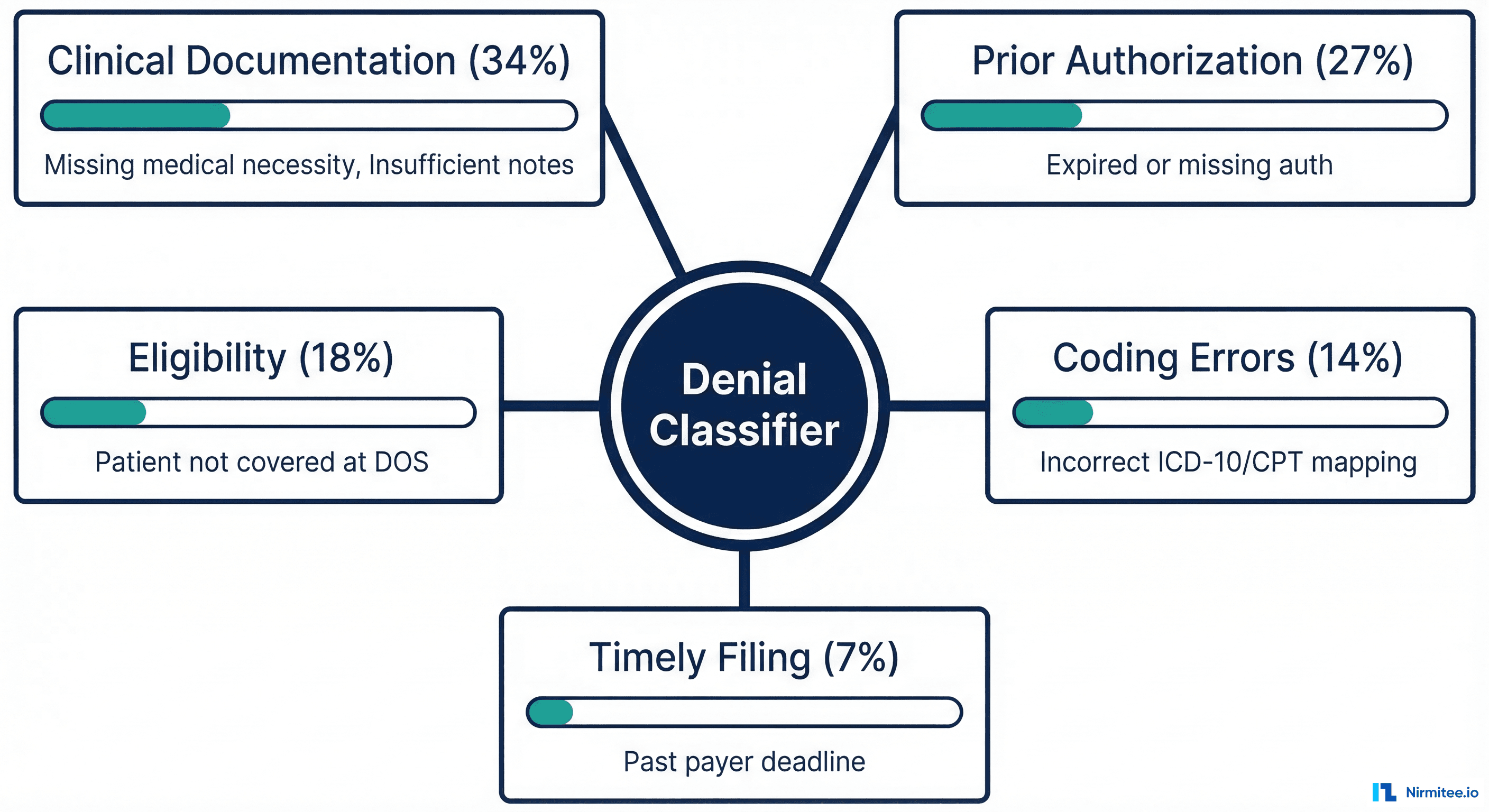
Classification Categories and Distribution
Based on industry data from HFMA and Change Healthcare, denials typically break down into five root cause categories:
- Clinical Documentation (34%): Missing medical necessity documentation, insufficient clinical notes to support the diagnosis or procedure. These require extracting evidence from the patient record.
- Prior Authorization (27%): Expired, missing, or mismatched authorization numbers. Our deep dive on how AI agents are eliminating the prior authorization bottleneck covers this category in detail.
- Eligibility (18%): Patient was not covered by the payer on the date of service, or coordination of benefits issues. Related: how an eligibility verification agent cuts verification to 30 seconds.
- Coding Errors (14%): Incorrect ICD-10 to CPT mapping, missing modifiers, unbundling errors, or diagnosis codes that do not support the billed procedure.
- Timely Filing (7%): Claim submitted past the payer's filing deadline. These are typically non-recoverable unless extenuating circumstances can be documented.
The classifier's accuracy is critical because it determines which downstream agent handles the appeal. A clinical documentation denial routes to the evidence extraction agent. A coding error routes to the coding validation agent. Getting this wrong wastes time and reduces overturn rates.
Agent 2: Automated Evidence Extraction and Appeal Generation
Once a denial is classified, the evidence extraction agent takes over. This is where the real intelligence lives. The agent needs to build a compelling, evidence-backed appeal, and it needs to do it in minutes, not the 15-20 minutes a human coder or analyst would spend.
Clinical Evidence Extraction via NLP
For clinical documentation denials (the largest category), the agent performs several NLP operations on the patient's encounter record:
- Medical necessity extraction: Scanning physician notes, H&P documentation, and progress notes for language that establishes medical necessity. The agent identifies key phrases like "acute exacerbation," "failed conservative treatment," "risk of complications if untreated."
- Diagnosis-procedure linkage: Verifying that documented diagnoses (ICD-10 codes) clinically justify the performed procedures (CPT codes). If a payer denies a chest CT (CPT 71260) for "lack of medical necessity," the agent searches for documented symptoms (persistent cough, hemoptysis, abnormal chest X-ray) that establish the clinical rationale.
- Supporting lab and imaging results: Pulling relevant lab values, imaging findings, and test results that corroborate the clinical decision. An elevated troponin supports cardiac catheterization. An abnormal MRI supports surgical intervention.
- Payer policy cross-reference: Matching extracted clinical evidence against the specific payer's coverage criteria, including Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs) from CMS.
Appeal Letter Generation
With evidence extracted, the appeal generator agent drafts a payer-ready letter. A well-structured AI-generated appeal includes:
APPEAL LETTER — CLAIM #[CLAIM_ID]
Patient: [NAME] | DOB: [DOB] | Member ID: [MEMBER_ID]
Date of Service: [DOS] | Provider: [PROVIDER_NPI]
Denied Service: CPT 71260 (CT Chest with Contrast)
Denial Reason: CARC 50 — Non-covered service
RARC: N386 — Based on Local Coverage Determination
CLINICAL JUSTIFICATION:
The patient presented on [DOS] with a 6-week history of persistent
productive cough, unintentional weight loss of 12 lbs, and hemoptysis.
Physical examination revealed decreased breath sounds in the right
lower lobe (documented in Dr. [NAME]'s progress note, page 3).
Chest X-ray performed on [DATE] showed a 2.3cm opacity in the right
lower lobe (Radiology Report #[ID]). Given the clinical presentation
— persistent cough with hemoptysis combined with radiographic
abnormality — CT Chest with contrast was medically necessary per
the applicable LCD (L37950) criteria, Section 4.2.
SUPPORTING EVIDENCE ATTACHED:
1. Progress notes from [DOS] (pages 1-4)
2. Chest X-ray report dated [DATE]
3. Lab results: CBC with differential showing elevated WBC
4. LCD L37950 relevant criteria excerpt
This service meets all coverage criteria under the applicable LCD.
We respectfully request reconsideration of this denial.The key differentiator is specificity. The agent does not generate generic appeal language. It cites the exact LCD number, references specific page numbers in clinical documentation, and links quantified clinical findings to the payer's published coverage criteria. This level of detail is what drives the 60%+ overturn rate.
Understanding how AI agents work in production, including the orchestration, tool use, and decision loops involved, is essential context. Our technical breakdown of how AI agents actually work in production systems covers the architecture patterns that make this possible.
Agent 3: Payer Rule Change Detection
Payer policies are a moving target. Medicare LCDs change quarterly. Commercial payers update their medical policies without fanfare. A denial management system that was calibrated last quarter may be operating on stale rules today.
The payer rule change detection agent solves this by continuously monitoring:
- CMS LCD/NCD updates: Tracking the Medicare Coverage Database for new, revised, or retired coverage determinations that affect denial patterns
- Commercial payer bulletins: Monitoring payer portals and provider newsletters for policy updates, prior authorization requirement changes, and billing guideline revisions
- Code set updates: CARC and RARC codes are updated three times per year by X12 and CMS. New codes mean new denial patterns the classifier must recognize.
- State-specific regulations: Tracking state insurance department rulings, prompt payment laws, and appeal deadline changes
When the agent detects a rule change, it updates the classifier's mapping rules and the appeal generator's policy references without requiring model retraining. This is a rule-engine update, not a machine learning update, which means it can take effect immediately.
For example, if UnitedHealthcare publishes a new medical policy requiring a specific modifier for telehealth visits effective April 1, the agent updates the coding validation rules to flag claims missing that modifier before submission, and updates appeal templates to reference the new policy for denials received after that date.
Agent 4: Predictive Denial Prevention
The most valuable denial is the one that never happens. Predictive denial prevention shifts the strategy from reactive appeal to proactive interception.
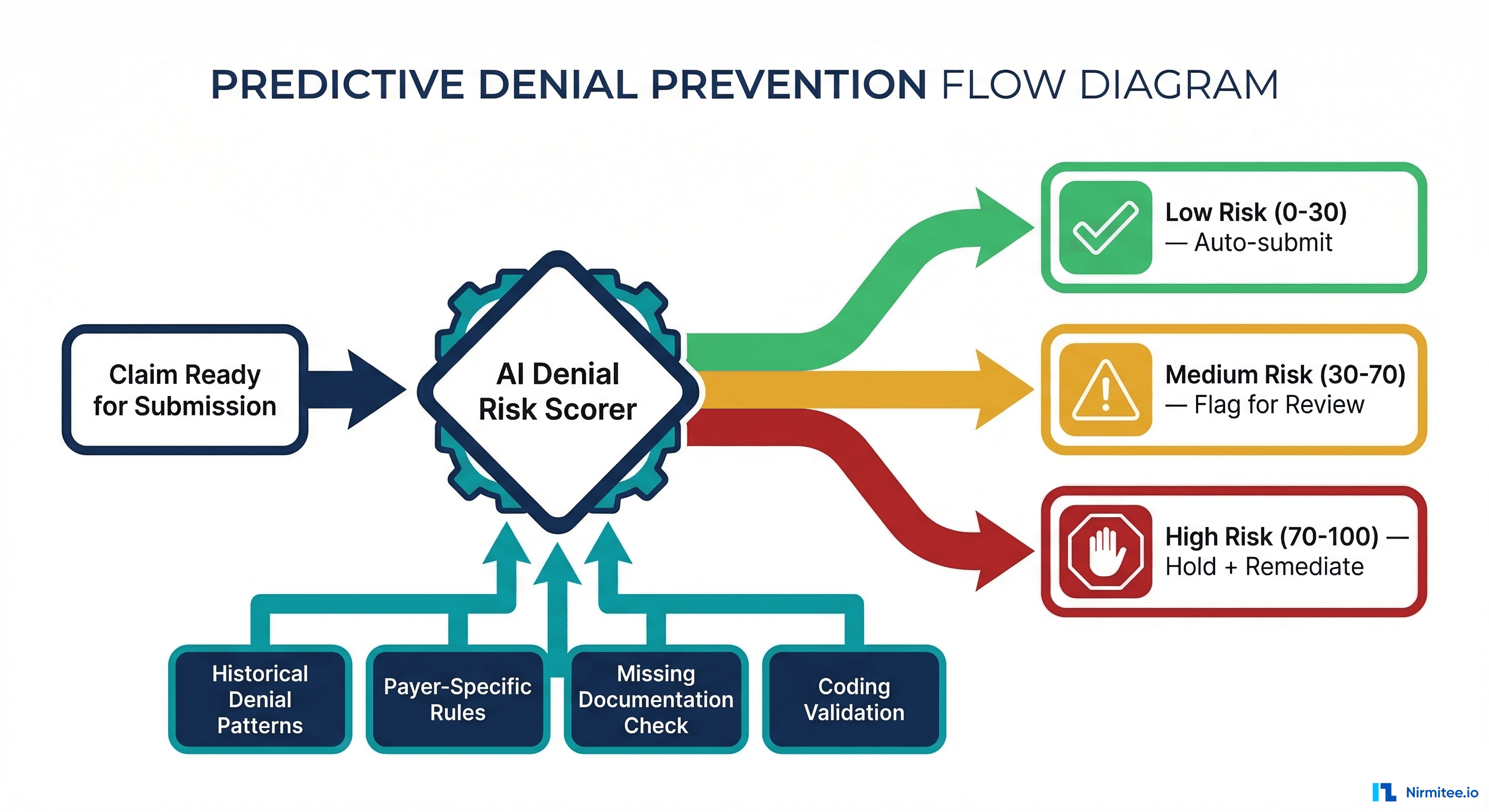
Pre-Submission Risk Scoring
Before a claim leaves your billing system, the denial risk scorer evaluates it against multiple data sources:
- Historical denial patterns: Has this payer denied this CPT code before? What was the denial rate for this specific CPT-ICD combination in the last 90 days? What is the denial rate for this referring provider?
- Payer-specific rules: Does this payer require prior authorization for this procedure? Is the patient's plan type subject to specific exclusions? Are there known payer processing quirks (e.g., specific modifier requirements)?
- Documentation completeness check: Are the required supporting documents attached? Is the medical necessity language present in the clinical notes? Does the documentation support the billed level of service?
- Coding validation: Does the ICD-10 code clinically support the CPT code? Are required modifiers present? Is the code combination subject to CCI edits?
Each claim receives a risk score from 0 to 100:
- Low Risk (0-30): Auto-submit. The claim matches historical approval patterns and all documentation is complete.
- Medium Risk (30-70): Flag for review. A human reviews the flagged elements, adds missing documentation or modifiers, and submits.
- High Risk (70-100): Hold and remediate. The claim has a high probability of denial and should not be submitted until the identified issues are resolved.
Health systems using predictive scoring report 25-40% reductions in initial denial rates within the first six months. Preventing a denial costs a fraction of appealing one.
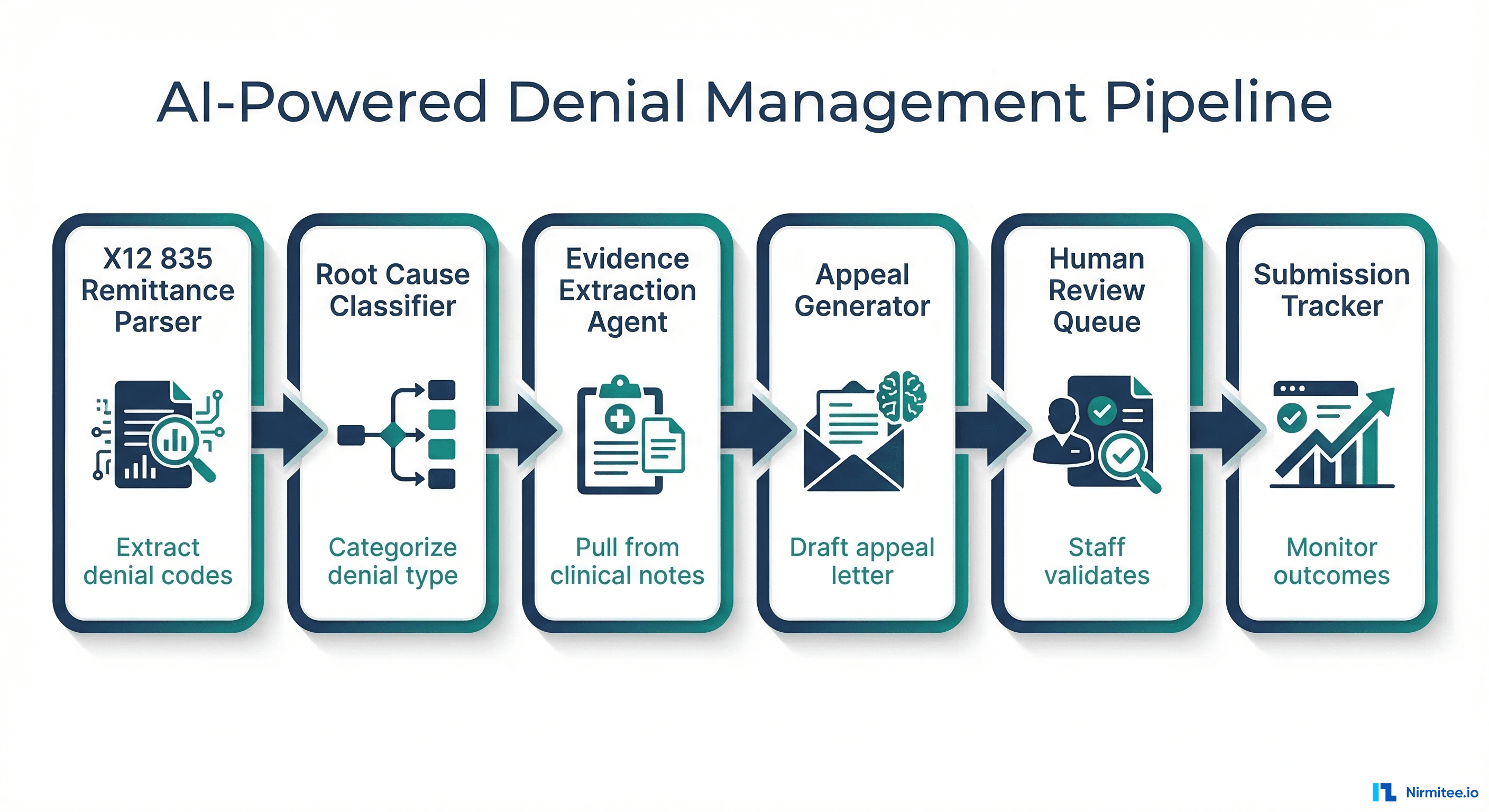
System Architecture: End-to-End Pipeline
The complete denial management agent system follows a pipeline architecture with human-in-the-loop checkpoints:
Data Flow Architecture
┌─────────────────┐ ┌──────────────────┐ ┌─────────────────────┐
│ X12 835 Parser │────▶│ Denial Root Cause│────▶│ Evidence Extraction │
│ (Remittance │ │ Classifier │ │ Agent (NLP on │
│ Ingestion) │ │ (CARC/RARC/Group)│ │ Clinical Notes) │
└─────────────────┘ └──────────────────┘ └──────────┬──────────┘
│
┌─────────────────┐ ┌──────────────────┐ ┌──────────▼──────────┐
│ Submission │◀────│ Human Review │◀────│ Appeal Letter │
│ Tracker │ │ Queue │ │ Generator │
│ (Payer Portal) │ │ (Staff Validates)│ │ (Payer-Specific) │
└─────────────────┘ └──────────────────┘ └─────────────────────┘
▲ ▲
│ ┌──────────────────┐ │
└───────────│ Payer Rule │────────────────┘
│ Change Monitor │
└──────────────────┘Integration Points
The system connects to your existing infrastructure at five key points:
- Clearinghouse / EDI gateway: Receives 835 remittance files and sends 837 claim resubmissions
- EHR / Clinical data repository: Read-only access to patient encounter notes, lab results, imaging reports, and clinical documentation via FHIR APIs or direct database queries
- Practice management system: Reads original claim data (837), patient demographics, insurance information, and authorization records
- Payer portals: Submits appeals electronically where available, tracks appeal status and outcomes
- Workflow / task management: Routes flagged claims to the human review queue and tracks staff actions
The agent system does not replace your clearinghouse or PMS. It sits between them, adding an intelligence layer that catches denials faster, classifies them accurately, and generates appeals that your staff reviews and submits. If you have explored why RPA failed healthcare and how agentic AI differs, this architecture demonstrates the difference: agents reason about denial context rather than just clicking through screens.
The ROI Case: $3.36M Annual Recovery
Revenue cycle directors need hard numbers to justify an AI investment. Here is the conservative math:
Recovery Calculation
| Metric | Manual Process | With AI Agents |
|---|---|---|
| Denials reviewed per month | 2,000 | 5,000 |
| Denials appealed (% of reviewed) | 35% (700) | 85% (4,250) |
| Average claim value | $500 | $500 |
| Overturn rate | 55% | 60% |
| Revenue recovered per month | $192,500 | $1,275,000 |
| Cost per appeal | $118 | $28 |
| Monthly appeal costs | $82,600 | $119,000 |
| Net monthly recovery | $109,900 | $1,156,000 |
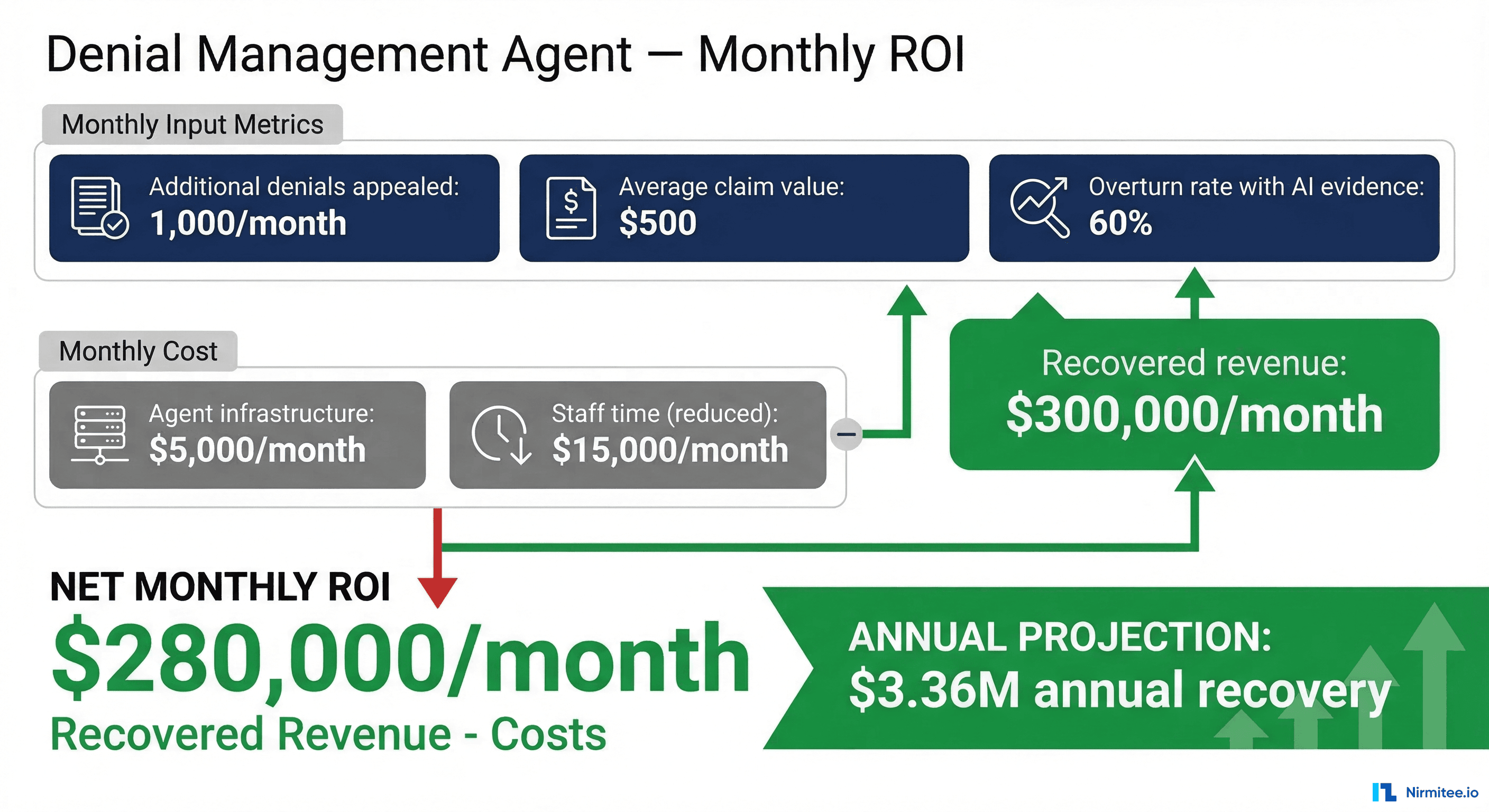
Even in the simplest scenario, appealing just 1,000 additional denials per month at $500 average value and a 60% overturn rate recovers $300,000 per month. Subtract $20,000 in agent infrastructure and reduced staff costs, and you net $280,000 per month, or $3.36 million annually.
The real multiplier is not just the recovery amount. It is the capacity unlock. When your denial analysts can review 800+ agent-prepared appeals per month instead of manually researching 200, you are processing 4x the volume without hiring additional FTEs. For a deeper look at how AI drives operational cost reduction across health systems, see our analysis on how healthcare companies are cutting 30% operational costs with AI.
Implementation Roadmap: From Pilot to Production
Deploying denial management agents is not an all-or-nothing endeavor. The most successful implementations follow a phased approach:
Phase 1: Denial Classification (Weeks 1-4)
- Connect 835 ingestion pipeline to your clearinghouse
- Build CARC/RARC mapping rules for your top 20 denial reason codes (which typically represent 80% of volume)
- Validate classifier accuracy against 90 days of historical denial data
- Target: 90%+ classification accuracy before proceeding
Phase 2: Evidence Extraction + Appeal Generation (Weeks 5-10)
- Integrate read-only access to your EHR's clinical documentation
- Build NLP pipelines for medical necessity language extraction
- Create appeal letter templates per denial category and per payer
- Human review rate: 100% of generated appeals reviewed by staff
Phase 3: Predictive Prevention (Weeks 11-16)
- Train risk scoring model on 12+ months of historical claims and denial outcomes
- Integrate pre-submission scoring into your billing workflow
- Set conservative thresholds initially (flag more, auto-submit less)
- Tune thresholds based on false positive/negative rates
Phase 4: Continuous Optimization (Ongoing)
- Deploy payer rule change monitoring
- Reduce human review rate to 20-30% for high-confidence appeals
- Expand to secondary and tertiary payers
- Build feedback loops: appeal outcomes improve classifier accuracy and risk scores
Data security and HIPAA compliance are non-negotiable throughout this process. Clinical data access must be governed by minimum necessary standards, all PHI must be encrypted in transit and at rest, and audit logs must track every agent access to patient records. Our HIPAA compliance checklist for developers covers the technical controls required.
Building production-grade healthcare AI agents requires careful architecture. Our Agentic AI for Healthcare team ships agents that meet clinical and compliance standards. We also offer specialized Healthcare AI Solutions services. Talk to our team to get started.
Frequently Asked QuestionsHow long does it take for an AI agent to process a denied claim?
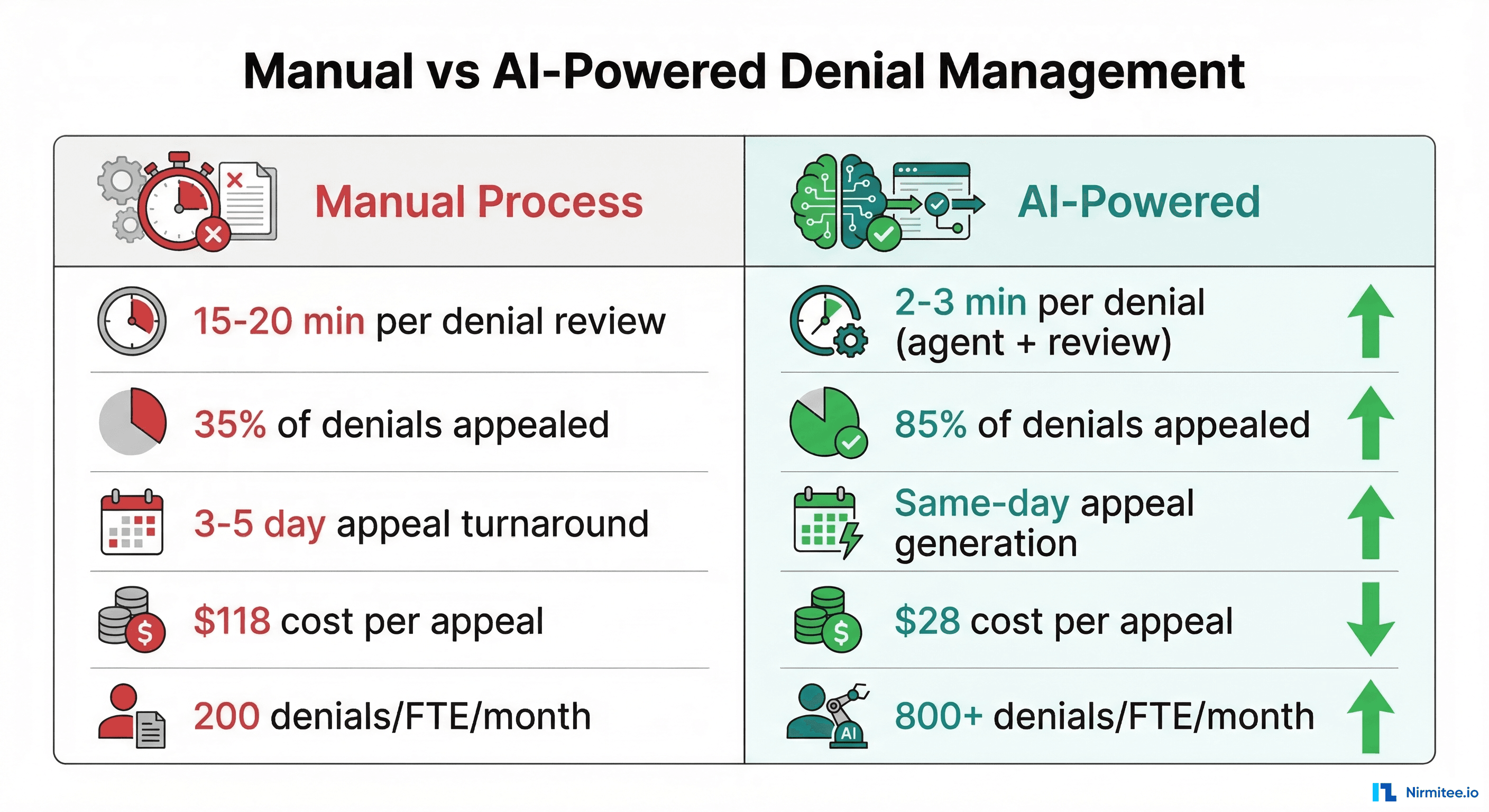
The full pipeline, from 835 ingestion through appeal letter generation, typically completes in 2-3 minutes per claim. The human review step adds an additional 3-5 minutes. Compare this to the 15-20 minutes for manual research and drafting per denial.
What denial categories are best suited for AI-generated appeals?
Clinical documentation and prior authorization denials (which together account for over 60% of all denials) show the highest ROI from agent-generated appeals. Coding error denials also respond well. Timely filing denials are typically non-recoverable regardless of appeal quality.
Does this replace denial management staff?
No. It augments their capacity. Staff shift from researching and drafting appeals to reviewing agent-generated appeals and handling complex edge cases that require human judgment. Most implementations see staff handling 3-4x more denials with the same headcount.
What EHR integrations are required?
At minimum, read-only access to clinical encounter notes and supporting documentation. FHIR R4 APIs (specifically the DocumentReference and DiagnosticReport resources) provide the cleanest integration path. Direct database access or HL7 ADT/ORU feeds work as alternatives.
How do you handle payer-specific appeal format requirements?
The appeal generator maintains payer-specific templates that conform to each payer's submission requirements, including format, required attachments, appeal address, and deadline calculations. The payer rule monitor keeps these templates current.
Building the System That Pays for Itself
Denial management is one of the clearest ROI cases for AI agents in healthcare. The inputs are structured (X12 835 files with standardized codes). The evidence is accessible (clinical documentation in your EHR). The appeal process follows established templates. And the financial impact is directly measurable.
The health systems that will thrive financially in 2026 and beyond are not the ones with the largest denial management teams. They are the ones that deploy intelligent agents to handle the volume while their staff focuses on the complex cases, payer negotiations, and process improvements that require human expertise.
At Nirmitee, we build AI agent systems for healthcare organizations, including denial management pipelines that integrate with your existing EHR, clearinghouse, and practice management infrastructure. If your revenue cycle team is drowning in denials and you are ready to explore what an agent-first approach looks like, let's talk.