Ask an EHR vendor how much their system costs, and you will get one of two responses: a vague "it depends" or a suspiciously low starting price that bears no resemblance to your final bill. This is not an accident. The electronic health record industry has perfected the art of opaque pricing, and it costs healthcare organizations billions of dollars in unexpected expenses every year.
This guide cuts through the sales fog. We have compiled real pricing data from implementation consultants, public contract filings, KLAS Research reports, and interviews with practice administrators who have lived through EHR implementations. Every dollar figure in this article reflects actual market conditions in 2025-2026, not vendor marketing materials.
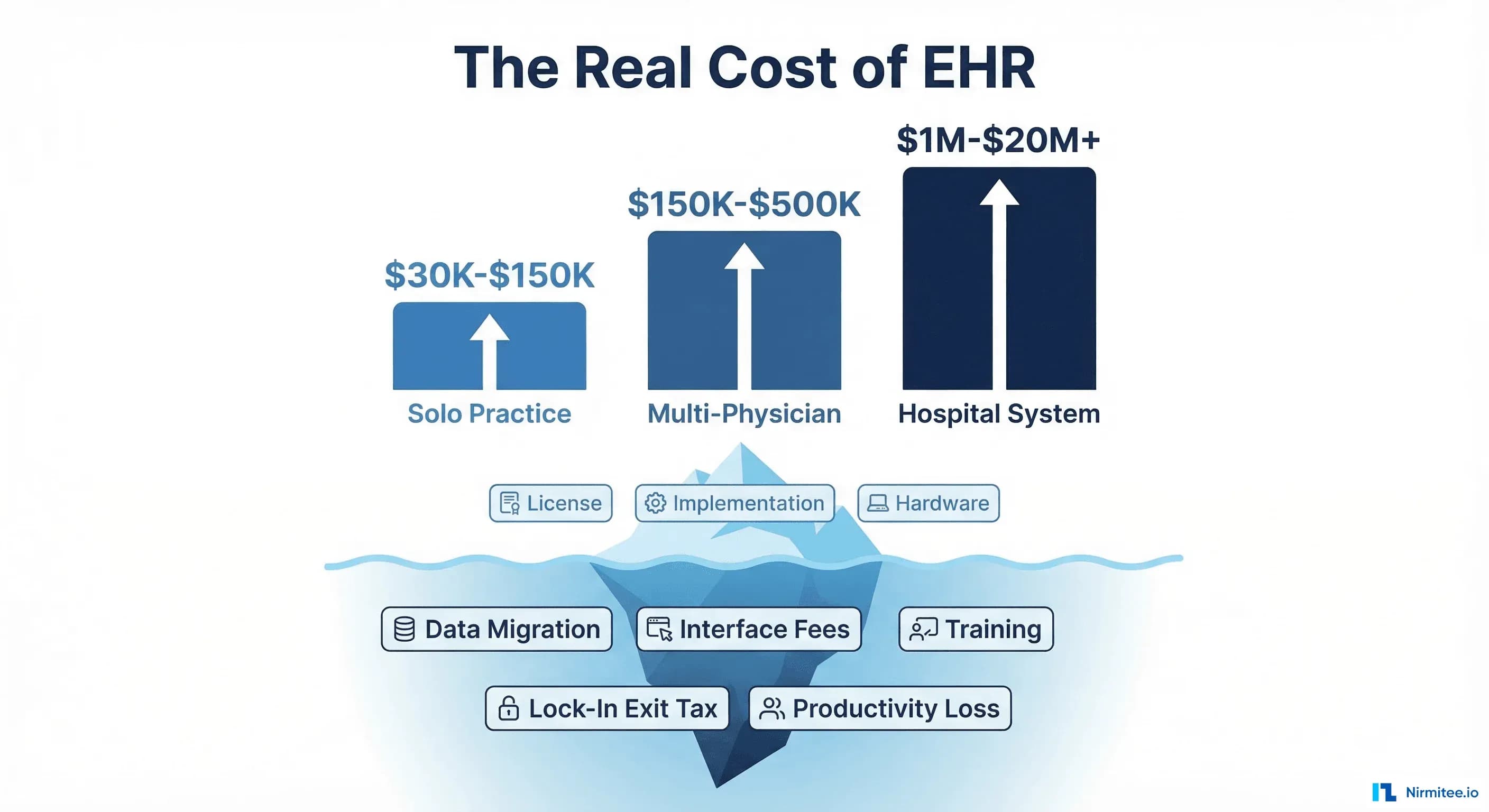
Whether you are a solo practitioner evaluating your first EHR, a multi-site practice considering a platform switch, or a hospital system negotiating a $20 million Epic contract, this guide will show you what you will actually pay — and the hidden costs that can double your total investment.
Why EHR Vendors Will Not Give You a Straight Answer on Pricing
The EHR pricing problem is structural, not accidental. Understanding why vendors obscure their costs is the first step to protecting your budget.
The "It Depends" Problem
EHR pricing genuinely varies based on dozens of factors: practice size, specialty, number of providers, desired modules, integration requirements, deployment model (cloud vs. on-premise), and implementation timeline. Vendors exploit this legitimate complexity to avoid publishing prices, which prevents comparison shopping and keeps buyers in the dark until deep into the sales cycle.
A 2024 KLAS Research survey found that 67% of healthcare organizations reported that their final EHR cost exceeded the initial quote by 20% or more. Among hospital systems, that figure rises to 78%. The gap between quoted and actual cost is not a bug — it is a feature of the sales process.
The Lock-In Economics
Once you sign an EHR contract, switching costs become astronomical. According to a 2024 MGMA report, only 23% of practices that are dissatisfied with their EHR have actually switched vendors. The other 77% stay — not because they are satisfied, but because the cost of leaving exceeds the pain of staying. Vendors know this, and it shapes their entire pricing strategy: get the customer in the door at a low price, then increase costs once switching becomes prohibitive.
What Happened When Texas Investigated
In 2024, the Texas Attorney General filed an antitrust lawsuit against Epic Systems, alleging that the company used anti-competitive practices to maintain its dominant market position. The lawsuit alleged that Epic's contractual terms, data-sharing restrictions, and pricing structures were designed to prevent customers from switching to competitors. While Epic has denied these allegations, the case highlighted practices that many in the industry have quietly complained about for years: data blocking, restrictive API access, and exit fees that can reach into the millions.
This was not an isolated incident. The ONC's Information Blocking Rule under the 21st Century Cures Act was specifically designed to address the practice of EHR vendors making it difficult or expensive for providers to access and share their own patient data. The rule, which went into full enforcement in 2024, prohibits practices that are "likely to interfere with, prevent, or materially discourage access, exchange, or use of electronic health information."
The Real Numbers: EHR Cost by Practice Size
Below are actual cost ranges based on publicly available contract data, consultant estimates, and practice administrator surveys. These figures include first-year implementation costs and are presented in 2025-2026 dollars.
Solo and Small Practices (1-5 Providers)
| Cost Category | Low Estimate | Mid Estimate | High Estimate |
|---|---|---|---|
| Software License / Subscription | $4,800/yr | $18,000/yr | $36,000/yr |
| Implementation & Configuration | $5,000 | $15,000 | $40,000 |
| Data Migration | $2,000 | $8,000 | $20,000 |
| Training | $1,500 | $5,000 | $12,000 |
| Hardware & Infrastructure | $2,000 | $8,000 | $25,000 |
| Interface/Integration (1-3) | $3,000 | $10,000 | $25,000 |
| First-Year Total | $18,300 | $64,000 | $158,000 |
For a solo physician choosing a cloud-based system like eClinicalWorks ($449-$599/month per provider), the low end is achievable. But most practices land in the mid range once they account for the implementation work, training time, and the inevitable scope creep that comes with configuring an EHR for your specific workflows.
Key insight: The license fee is typically only 25-35% of first-year costs. For every dollar you spend on software, plan to spend $2-3 on everything else.
Multi-Physician Practices (6-20 Providers)
| Cost Category | Low Estimate | Mid Estimate | High Estimate |
|---|---|---|---|
| Software License / Subscription | $36,000/yr | $120,000/yr | $300,000/yr |
| Implementation & Configuration | $25,000 | $75,000 | $200,000 |
| Data Migration | $10,000 | $30,000 | $50,000 |
| Training ($1,500/physician avg.) | $9,000 | $22,500 | $45,000 |
| Hardware & Infrastructure | $10,000 | $30,000 | $75,000 |
| Interfaces/Integrations (3-8) | $15,000 | $60,000 | $150,000 |
| Workflow Customization | $5,000 | $25,000 | $75,000 |
| First-Year Total | $110,000 | $362,500 | $895,000 |
At this size, the choice between athenahealth (revenue-based pricing at 4-8% of collections) and traditional per-provider models starts to matter significantly. A 15-provider practice collecting $5 million annually could pay $200,000-$400,000/year to athenahealth — competitive with per-provider models but with very different cash flow implications.
Multi-site practices face additional costs that single-location practices avoid: VPN infrastructure between offices ($5,000-$15,000), additional interface engines for site-specific lab and imaging connections, and the coordination overhead of rolling out to multiple locations sequentially.
Hospital Systems (50+ Beds)
| Cost Category | Community Hospital (50-200 beds) | Regional System (200-500 beds) | Large System (500+ beds) |
|---|---|---|---|
| Software License | $1M-$5M | $5M-$15M | $15M-$50M+ |
| Implementation Services | $2M-$8M | $8M-$25M | $25M-$100M+ |
| Data Migration | $200K-$1M | $1M-$5M | $5M-$20M |
| Training | $500K-$2M | $2M-$8M | $8M-$25M |
| Hardware/Infrastructure | $500K-$3M | $3M-$10M | $10M-$30M |
| Interfaces (20-100+) | $200K-$2M | $2M-$10M | $10M-$30M |
| Productivity Loss (go-live) | $1M-$5M | $5M-$15M | $15M-$50M |
| First-Year Total | $5.4M-$26M | $26M-$88M | $88M-$305M+ |
Epic dominates the large hospital market with approximately 38% market share among hospitals with 500+ beds. A typical Epic implementation for a mid-size health system runs $150M-$300M over 10 years when you include all direct and indirect costs. The University of Michigan's Epic implementation cost a reported $240 million. Cambridge University Hospitals in the UK spent $274 million on their Epic deployment.
These numbers are not outliers — they are the norm for enterprise EHR implementations. The implementation services alone (consultants, project management, workflow redesign) routinely exceed the software license cost by a factor of 2-3x.
Related reading: CMS Interoperability Rules in 2026: What You Actually Need to Do
The Hidden Costs Nobody Warns You About
The figures above represent the costs that appear in vendor proposals. The costs below are the ones that do not — and they routinely add 30-60% to the total bill.
Data Migration: $20,000 - $50,000 (Practice) / $1M - $20M (Hospital)
Moving your existing patient data into a new EHR is one of the most underestimated costs in healthcare IT. The challenge is not just transferring data — it is mapping data from one system's schema to another, cleaning up years of inconsistencies, validating that nothing was lost or corrupted, and running the old and new systems in parallel during the transition.
For a typical multi-physician practice, data migration costs break down as follows:
- Data extraction from legacy system: $5,000-$15,000 (often charged by the outgoing vendor as an "exit fee")
- Data mapping and transformation: $8,000-$20,000
- Data validation and QA: $3,000-$10,000
- Historical document scanning/import: $4,000-$15,000
- Parallel system operation (30-90 days): $5,000-$15,000 in duplicate license costs
The dirty secret: many practices discover that their legacy vendor charges $0.50-$2.00 per patient record just to extract data in a usable format. For a practice with 30,000 active patients, that is $15,000-$60,000 just to get your own data out. This is the "data extraction exit tax" that vendors rarely mention during the sales process.
Interface and Integration Fees: $5,000 - $25,000 Per Interface
Every connection between your EHR and an external system — lab systems, imaging centers, pharmacies, billing clearinghouses, patient portals, medical devices — requires an interface. Each interface costs money to build, test, certify, and maintain.
Typical per-interface costs:
| Interface Type | Build Cost | Annual Maintenance |
|---|---|---|
| Lab Results (HL7v2) | $5,000-$15,000 | $1,200-$3,600/yr |
| Pharmacy (NCPDP/SCRIPT) | $3,000-$8,000 | $600-$2,400/yr |
| Imaging/PACS (DICOM) | $8,000-$25,000 | $2,400-$6,000/yr |
| Billing/Clearinghouse | $5,000-$12,000 | $1,200-$3,600/yr |
| HIE Connection | $10,000-$25,000 | $3,000-$8,000/yr |
| Patient Portal | $5,000-$15,000 | $1,200-$4,800/yr |
| Medical Device Integration | $8,000-$20,000 | $2,400-$6,000/yr |
A typical multi-physician practice needs 5-10 interfaces. A hospital might need 50-200. At $5,000-$25,000 each, plus annual maintenance, integration costs can exceed the EHR license itself.
The emerging FHIR standard is designed to reduce these costs by providing a standardized API layer. But most legacy systems still rely on HL7v2 point-to-point interfaces, and the transition to FHIR-based interoperability is measured in years, not months.
Related: TEFCA, Information Blocking, and Your Integration Engine: 2026 Compliance Guide
Customization: $10,000 - $100,000+
No EHR works perfectly out of the box for every specialty. Dermatology practices need image annotation workflows. Orthopedic groups need specific surgical documentation templates. Behavioral health requires different note structures than primary care. Every customization costs money.
Common customization costs:
- Custom templates and forms: $2,000-$15,000 per template
- Workflow modifications: $5,000-$25,000 per workflow
- Custom reports and dashboards: $3,000-$20,000 each
- Specialty-specific modules: $10,000-$50,000
- API development for custom integrations: $15,000-$75,000
Worse, many customizations need to be rebuilt or re-tested with every major EHR version upgrade. A vendor who charges $50,000 to customize your system today may charge $15,000-$25,000 to update those customizations when they release their next major version. This creates a recurring cost that few organizations budget for.
Training: $1,500 Per Physician (And That Is Just the Start)
The $1,500 per physician figure is the direct training cost — classroom time, e-learning modules, and go-live support. But the real cost of training is measured in lost productivity.
Research published in the Journal of Health Affairs found that physician productivity drops by 20-30% for the first 3-6 months after an EHR implementation. For a physician generating $500,000 in annual collections, a 25% productivity loss over 4 months represents $41,667 in lost revenue — per physician. For a 10-provider practice, that is $416,670 in lost collections that never appears on any vendor's quote.
Additional training-related costs:
- Super-user training (power users who support others): $3,000-$8,000 per super-user
- Staff turnover re-training: $500-$2,000 per new hire, ongoing
- Annual refresher and upgrade training: $300-$800 per user per year
- Temporary staffing during training: $5,000-$20,000 for practice coverage
The Data Extraction "Exit Tax"
Perhaps the most egregious hidden cost is what happens when you try to leave. Despite the CMS interoperability mandates and the Information Blocking Rule, extracting your data from a legacy EHR remains expensive and time-consuming.
Common exit costs reported by practices that have switched vendors:
- Data extraction fee: $10,000-$50,000 (charged by the outgoing vendor)
- Data in non-standard format: Additional $5,000-$20,000 for conversion
- Contract early termination penalty: 50-100% of remaining contract value
- Continued access fee: $500-$2,000/month for read-only access during transition
- Legal review of exit terms: $5,000-$15,000
Total exit costs for a mid-size practice typically range from $50,000 to $150,000 — and that is before paying for the new system. For hospital systems, exit costs can exceed $10 million. This is the vendor lock-in tax, and it is the single biggest reason why organizations stay with underperforming EHR systems.
The True Cost of Vendor Lock-In: A 5-Year TCO Analysis
To understand the real financial impact of EHR vendor lock-in, let us model a 5-year Total Cost of Ownership for a 15-provider multi-specialty practice under two scenarios: a proprietary EHR with typical lock-in dynamics versus an open-standards-based system.
Scenario A: Proprietary EHR (Typical Major Vendor)
| Year | License/Subscription | Implementation & Support | Interfaces & Integrations | Hidden Costs | Cumulative Total |
|---|---|---|---|---|---|
| Year 1 | $150,000 | $200,000 | $75,000 | $125,000 | $550,000 |
| Year 2 | $157,500 | $45,000 | $25,000 | $40,000 | $817,500 |
| Year 3 | $165,375 | $45,000 | $35,000 | $45,000 | $1,107,875 |
| Year 4 | $173,644 | $45,000 | $30,000 | $35,000 | $1,391,519 |
| Year 5 | $182,326 | $45,000 | $25,000 | $30,000 | $1,673,845 |
5-Year TCO: $1,673,845
Key assumptions: 5% annual license escalation (typical in EHR contracts), Year 1 implementation includes data migration and training, ongoing interface costs include new connections and maintenance, and hidden costs include customization rework, upgrade labor, and productivity impacts.
Scenario B: Open-Standards EHR (FHIR-Native)
| Year | License/Subscription | Implementation & Support | Interfaces & Integrations | Hidden Costs | Cumulative Total |
|---|---|---|---|---|---|
| Year 1 | $120,000 | $180,000 | $40,000 | $100,000 | $440,000 |
| Year 2 | $123,600 | $36,000 | $12,000 | $25,000 | $636,600 |
| Year 3 | $127,308 | $36,000 | $10,000 | $20,000 | $829,908 |
| Year 4 | $131,127 | $36,000 | $10,000 | $15,000 | $1,022,035 |
| Year 5 | $135,061 | $36,000 | $10,000 | $12,000 | $1,215,096 |
5-Year TCO: $1,215,096
5-Year Savings: $458,749 (27.4% reduction)
The savings come from three primary sources:
- Lower interface costs: FHIR APIs reduce per-interface build costs by 40-60% compared to HL7v2 point-to-point connections, and ongoing maintenance is significantly lower
- Reduced lock-in premium: When switching costs are lower, vendors compete more aggressively on price and must deliver ongoing value rather than relying on contractual captivity
- Lower customization rework: Standards-based systems using open APIs require less re-engineering during upgrades
At Nirmitee, we build healthcare integration platforms on open FHIR standards precisely because we have seen these TCO dynamics play out across dozens of implementations. When your data flows through standardized FHIR APIs rather than proprietary interfaces, the long-term cost advantages compound year over year.
EHR Pricing Models Compared
Understanding the three dominant EHR pricing models is critical to predicting your long-term costs. Each model transfers financial risk differently between the vendor and the buyer.
Model 1: Per-Provider Subscription (SaaS)
How it works: You pay a monthly fee per provider (physician, NP, PA) who uses the system. Pricing typically ranges from $500 to $2,000 per provider per month, depending on the vendor and included modules.
Representative vendors: eClinicalWorks ($449-$599/mo), DrChrono ($500-$1,100/mo), Practice Fusion ($149-$399/mo for basic tiers)
Advantages:
- Predictable monthly cost
- Lower upfront investment
- Vendor handles hosting, updates, and security patches
- Scales linearly with practice growth
Disadvantages:
- Higher long-term cost than perpetual license for stable practices
- You never own the software
- Vendor can increase prices at renewal (typical escalation: 3-8% annually)
- Data is stored on vendor infrastructure, adding exit complexity
5-Year TCO for 10 providers: $360,000 - $1,200,000 (license only, before implementation)
Model 2: Revenue-Based Pricing (Percentage of Collections)
How it works: Instead of a fixed fee, you pay a percentage of your practice's collections. Typical range: 3-8% of net collections. This model aligns the vendor's revenue with your practice's financial success.
Representative vendors: athenahealth (approximately 4-8% of collections, including RCM services), some regional EHR vendors
Advantages:
- No upfront software cost in many cases
- Cost scales with revenue — you pay less during slow periods
- Vendor is financially incentivized to help you collect more
- Often includes revenue cycle management (RCM) services in the fee
Disadvantages:
- Extremely expensive for high-revenue practices — a $10M practice pays $400,000-$800,000/year
- Cost never decreases even after implementation is "done"
- Difficult to compare against fixed-fee models
- Revenue-based contracts are among the hardest to exit
5-Year TCO for 10 providers ($5M annual collections): $750,000 - $2,000,000
Model 3: Perpetual License (On-Premise)
How it works: You pay a one-time license fee to "own" the software, then pay annual maintenance (typically 15-22% of the license cost) for updates and support. You host the system on your own infrastructure.
Representative vendors: Epic (for hospital systems), MEDITECH, legacy installations of many vendors who have since moved to SaaS
Advantages:
- Data stays on your infrastructure
- Lower long-term cost if you maintain the system for 7+ years
- More control over upgrade timing
- No per-provider monthly fees after purchase
Disadvantages:
- Very high upfront cost ($100,000-$500,000+ for practices, $5M-$50M+ for hospitals)
- You are responsible for hosting, backups, security, and disaster recovery
- Maintenance fees increase over time (and vendors can refuse support if you skip upgrades)
- Hardware refresh costs every 4-5 years
- IT staffing requirements are 2-5x higher than SaaS models
5-Year TCO for 10 providers: $500,000 - $2,000,000+ (including infrastructure and IT staff)
Which Model Costs Less? The Answer Depends on Your Revenue
For practices with annual collections under $3 million, per-provider subscription is almost always the most cost-effective model. Between $3-8 million, it depends on negotiation and included services. Above $8 million, fixed-fee models become significantly cheaper than revenue-based pricing.
The key principle: never choose a pricing model in isolation. Calculate the 5-year TCO under each model using your actual numbers, and factor in the switching costs if you need to change models later.
How to Negotiate Your EHR Contract: 7 Clauses That Save You Hundreds of Thousands
Most healthcare organizations treat EHR contract negotiation as a software purchase. It is actually a decade-long partnership agreement that will define your operational flexibility, data strategy, and technology roadmap. Here are the seven contract provisions that have the highest financial impact — and that most buyers fail to negotiate.
1. Data Portability Guarantee
What to demand: A written guarantee that all patient data will be provided in standard, machine-readable formats (C-CDA, FHIR Bulk Data Export, or CSV) within 90 days of termination notice, at no additional cost.
Why it matters: Without this clause, you may face $50,000-$500,000 in data extraction fees when you leave, delivered in proprietary formats that cost additional money to convert. The ONC Information Blocking Rule supports your position, but having it in the contract gives you contractual enforcement beyond regulatory complaints.
Negotiation leverage: Reference the 21st Century Cures Act and the ONC Final Rule. Any vendor who resists standardized data export is positioning for future information blocking complaints.
2. FHIR API Access at No Additional Cost
What to demand: Full access to the vendor's FHIR R4 API endpoints for all standard resource types, with no per-call fees, rate limiting below reasonable thresholds, or additional licensing requirements.
Why it matters: Some vendors technically offer FHIR APIs but charge $10,000-$50,000 annually for "API access licenses" or impose rate limits that make the API useless for production workflows. The CMS Interoperability and Patient Access Rule requires payers to offer FHIR APIs, and similar requirements are expanding to providers.
Negotiation leverage: API access is increasingly a regulatory requirement, not a premium feature. Frame it as compliance, not an add-on.
3. No Data Extraction Fees
What to demand: Zero fees for exporting your own clinical, financial, and operational data at any time, in any format you request, for any purpose including migration to a competitor.
Why it matters: Data extraction fees are the backbone of vendor lock-in economics. Eliminating them at contract signing removes the single biggest barrier to switching.
Negotiation leverage: "We consider data extraction fees to be information blocking under 45 CFR 171. We need this clause to ensure our future compliance posture."
4. Exit Terms and Transition Timeline
What to demand: Clear terms for contract termination including: maximum notice period (90 days), no early termination penalty after year 3, vendor obligation to provide 12 months of read-only access at no additional cost during transition, and a defined data transfer cooperation framework.
Why it matters: Without exit terms, you are at the vendor's mercy when it is time to leave. The cost of an unplanned EHR transition without contractual protections averages 2-3x the cost of a planned transition with clear exit terms.
5. Uptime SLA with Financial Penalties
What to demand: A 99.9% uptime SLA (approximately 8.7 hours of downtime per year) with financial remedies: service credits of 10-25% of monthly fees for each hour of unplanned downtime, and contract termination rights if uptime falls below 99.5% in any quarter.
Why it matters: EHR downtime costs healthcare organizations an estimated $7,900 per minute in lost revenue and operational disruption, according to a Ponemon Institute study. An SLA without financial penalties is a marketing document, not a contractual commitment.
6. Integration Fee Caps
What to demand: A maximum annual cost for new interfaces, including a defined number of included integrations (3-5 per year) and a cap on per-interface costs for additional connections (not to exceed $10,000 per standard interface).
Why it matters: Interface costs are one of the most common sources of budget overruns. Without caps, you may pay $25,000 for an interface that a competitor charges $5,000 for, with no recourse.
7. Price Lock Period
What to demand: A 3-year minimum price lock on all subscription fees, with any subsequent increases capped at CPI or 3%, whichever is lower. No "market rate adjustments" or other mechanisms that allow unlimited price increases.
Why it matters: Without price protection, vendors typically increase rates by 5-10% annually after the initial term. Over a 7-year relationship, an 8% annual increase turns a $150,000/year contract into $257,000/year — a 71% increase. A 3% cap keeps it at $184,000.
Cumulative 7-year difference: Uncapped escalation costs $195,000 more than a 3%-capped contract. This single clause can be the most valuable provision in your entire agreement.
Making the Right EHR Investment: A Framework for Decision-Making
After reviewing the real numbers, hidden costs, and contract pitfalls, here is a practical framework for making your EHR investment decision:
The 5-Question Cost Evaluation
- What is the 5-year TCO, not just Year 1? Demand a detailed 5-year cost projection from every vendor, including license escalation, interface maintenance, and training for staff turnover.
- What are my switching costs? Calculate the cost of leaving this vendor in Year 3, Year 5, and Year 7. If the answer is "we do not know," that is a red flag.
- What am I paying for that should be free? FHIR API access, data export, standard report generation, and basic interoperability should not be premium features in 2026.
- What is my cost per encounter? Divide total annual EHR costs by annual patient encounters. Benchmarks: $15-$30/encounter for ambulatory, $50-$150/encounter for inpatient. If you are above these ranges, you are overpaying.
- What does the exit look like? Before signing, simulate the exit process. If the vendor cannot clearly articulate how you would leave and what it would cost, you will find out the hard way.
The Open Standards Advantage
The healthcare industry is at an inflection point. The combination of the TEFCA framework, the Information Blocking Rule, and CMS interoperability mandates is creating a regulatory environment that increasingly favors open standards over proprietary lock-in.
Organizations that invest in FHIR-native systems today position themselves for:
- Lower integration costs: FHIR APIs cost 40-60% less per integration than HL7v2 interfaces
- Easier vendor switching: Standardized data formats reduce migration costs by 50-70%
- Regulatory compliance: Meeting current and future interoperability requirements without additional investment
- Innovation access: Open APIs enable third-party apps and AI-powered clinical tools that proprietary systems cannot support
Nirmitee's healthcare integration platform is built on this principle. We help organizations connect their existing EHR systems through SMART on FHIR and standardized APIs, reducing integration costs and eliminating the data silos that drive vendor lock-in.
Conclusion: The Most Expensive EHR Is the One You Cannot Leave
The sticker price of an EHR system is the least important number in your evaluation. What matters is the total cost of ownership over 5-10 years, including the hidden costs that vendors deliberately omit from their proposals: data migration, interface fees, customization, training productivity loss, and the exit tax that keeps you locked in even when a better option exists.
The healthcare organizations that manage EHR costs most effectively share three characteristics:
- They negotiate before signing, not after. Every contract clause listed in this guide is negotiable — but only before you sign. After implementation, your leverage drops to near zero.
- They calculate TCO, not sticker price. A system that costs $100,000 less in Year 1 but $50,000 more per year in hidden fees is not cheaper — it is $150,000 more expensive over 5 years.
- They demand open standards. FHIR APIs, standardized data export, and interoperability are not nice-to-have features. They are the foundation of long-term cost control and the only reliable hedge against vendor lock-in.
Your EHR is the operational backbone of your healthcare organization. It deserves the same financial scrutiny you would apply to a building lease or a major equipment purchase. Armed with the real numbers in this guide, you can walk into your next vendor negotiation knowing exactly what things cost — and exactly what to demand.
Need help evaluating EHR integration costs or building a standards-based interoperability strategy? Talk to Nirmitee's integration team about reducing your healthcare IT total cost of ownership.
From concept to deployment, our Custom Healthcare Software Development team ships healthcare applications that clinicians actually use. We also offer specialized Healthcare Interoperability Solutions services. Talk to our team to get started.
Frequently Asked QuestionsHow much does an EHR system cost for a small practice?
A small practice with 1-5 providers should budget $18,000 to $158,000 for first-year costs, including software, implementation, data migration, training, and interfaces. Cloud-based subscriptions like eClinicalWorks ($449-$599/month per provider) offer the lowest entry point, but total costs including implementation typically run 3-4x the license fee alone.
What are the biggest hidden costs of EHR implementation?
The five biggest hidden costs are: (1) data migration from your legacy system ($20,000-$50,000 for practices), (2) interface fees for lab, pharmacy, and imaging connections ($5,000-$25,000 each), (3) physician productivity loss during transition (20-30% for 3-6 months), (4) ongoing customization and upgrade rework costs, and (5) the data extraction "exit tax" if you ever need to switch vendors ($10,000-$50,000+).
How much does it cost to switch EHR vendors?
Switching costs typically range from $50,000 to $150,000 for multi-physician practices and $5 million to $20 million+ for hospital systems. This includes data extraction fees, early termination penalties, parallel system operation costs, new system implementation, re-training, and productivity loss. Only 23% of dissatisfied practices actually switch vendors, primarily because switching costs exceed the cost of staying.
Is Epic worth the cost for hospitals?
Epic's total 10-year cost for a mid-size health system typically ranges from $150 million to $300 million. Whether it is "worth it" depends on your organization's size, complexity, and strategic priorities. Epic offers the deepest feature set and largest network effects, but comes with significant vendor lock-in risk and among the highest switching costs in the industry. Organizations should carefully evaluate open-standards alternatives and negotiate robust exit terms before committing.
How can I reduce EHR implementation costs?
Five proven strategies: (1) Negotiate a 5-year contract with price lock and exit terms before signing, (2) Choose FHIR-native systems to reduce interface costs by 40-60%, (3) Phase your implementation to spread costs and learn from early modules, (4) Invest heavily in training to minimize the productivity loss window, and (5) Demand data portability guarantees to preserve future negotiating leverage.