The Hidden Layer That Makes or Breaks Healthcare Data Exchange
You can build the fastest FHIR API, deploy the most reliable integration engine, and connect every system in your hospital — but if your lab sends "glucose" while your EHR expects "GLUC" and your analytics platform looks for LOINC code 2345-7, your data is meaningless.
Healthcare terminology standards are the invisible layer that gives data meaning. They ensure that when Lab A in Boston sends a hemoglobin result and Hospital B in Chicago receives it, both systems understand exactly what that result represents — same test, same units, same clinical significance.
This guide explains the six major healthcare terminology standards, how they relate to each other, when to use each one, and how to implement them in your organization.
The Healthcare Terminology Ecosystem
Healthcare uses multiple overlapping terminology standards because different aspects of care require different classification systems. No single standard covers everything.
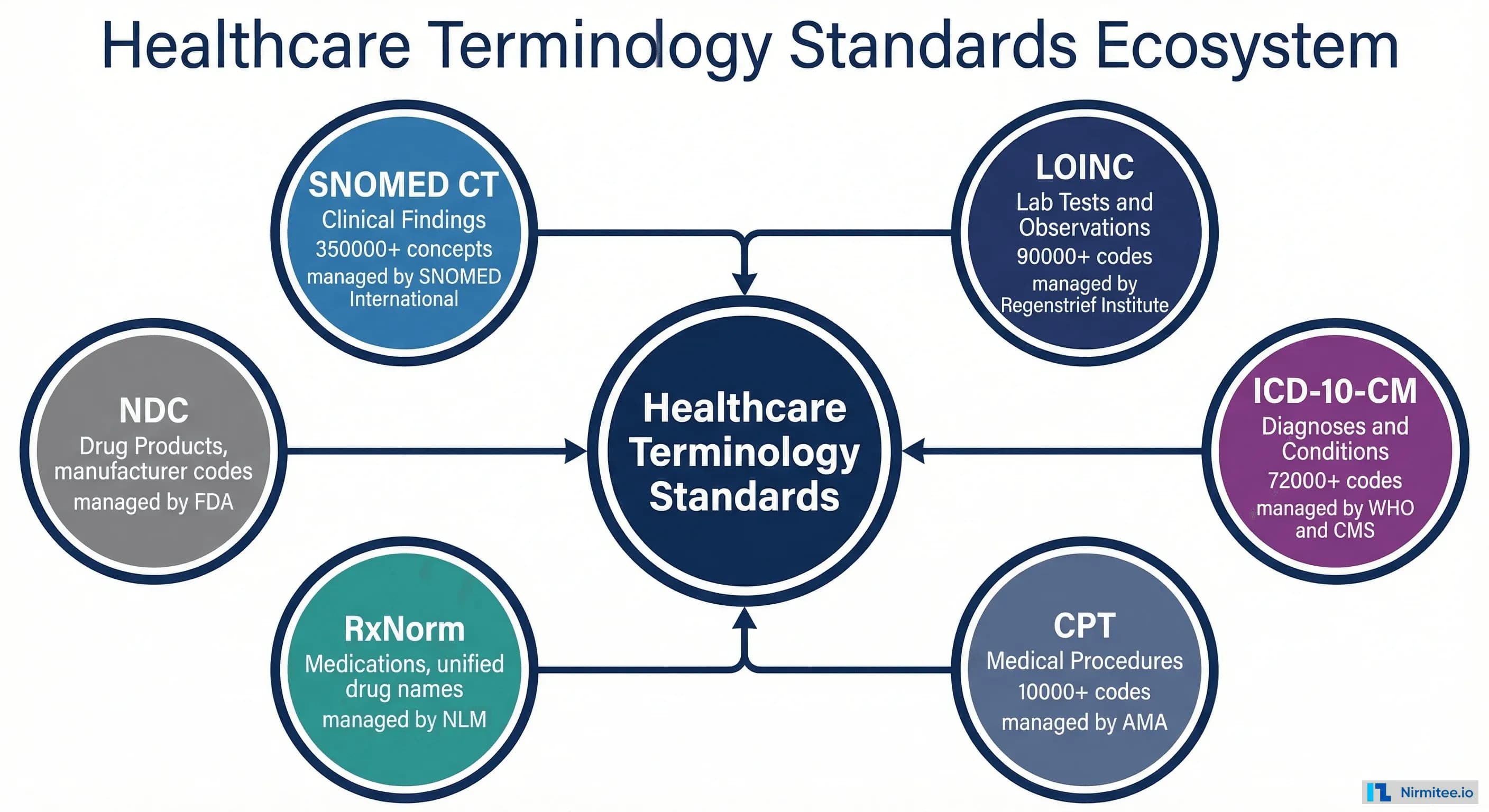
The six standards you need to know:
- SNOMED CT — Clinical findings, diseases, procedures, body structures. The most comprehensive clinical terminology with 350,000+ concepts.
- LOINC — Laboratory tests and clinical observations. 90,000+ codes covering every lab test, vital sign, and clinical measurement.
- ICD-10-CM — Diagnoses and conditions for billing and reporting. 72,000+ codes used for insurance claims and epidemiological tracking.
- CPT — Medical procedures for billing. 10,000+ codes owned by the AMA, required for reimbursement claims.
- RxNorm — Medications. Provides normalized names for drugs across different naming systems used by pharmacies, EHRs, and payers.
- NDC — Drug products. National Drug Codes identify specific manufactured drug products for supply chain and dispensing.
SNOMED CT: The Clinical Language
SNOMED CT (Systematized Nomenclature of Medicine — Clinical Terms) is the most comprehensive healthcare terminology in existence. It's the standard for documenting clinical findings in electronic health records.
SNOMED CT organizes clinical knowledge in a hierarchy using "is-a" relationships. Type 2 Diabetes Mellitus is-a Diabetes Mellitus, which is-a Disorder of glucose metabolism, which is-a Clinical Finding. This hierarchy enables powerful queries: search for "all endocrine disorders" and automatically find every diabetes variant, thyroid condition, and adrenal disorder.
When to use SNOMED CT: Clinical documentation, problem lists, allergy recording, clinical decision support, population health analytics. SNOMED CT is required by USCDI for clinical findings and is the primary terminology for FHIR Condition and AllergyIntolerance resources.
LOINC: The Lab Test Dictionary
LOINC (Logical Observation Identifiers Names and Codes) provides universal codes for laboratory tests and clinical observations. Without LOINC, a "glucose test" at one lab might be coded as "GLU," at another as "GLUC," and at a third as "BG" — making data aggregation impossible.
Every LOINC code has six axes that fully describe the observation:
- Component — What is being measured (Glucose, Hemoglobin, Sodium)
- Property — The characteristic measured (mass concentration, enzyme activity, number)
- Timing — Point in time vs. over a period
- System — The specimen type (Serum/Plasma, Urine, Blood)
- Scale — Quantitative, ordinal, nominal, or narrative
- Method — The measurement technique (optional)
When to use LOINC: Lab results, vital signs, clinical measurements, survey instruments, document types. LOINC is required by USCDI for all laboratory observations and is the primary terminology for FHIR Observation and DiagnosticReport resources.
ICD-10-CM: The Billing Language
ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) is the diagnosis coding system used for medical billing, insurance claims, and public health reporting in the United States.
ICD-10-CM codes are alphanumeric, starting with a letter that indicates the chapter (disease category). The code gets more specific with each additional character — E11 is Type 2 Diabetes, E11.6 adds "with complications," and E11.65 specifies "with hyperglycemia."
When to use ICD-10-CM: Insurance claims, billing, death certificates, epidemiological reporting, quality metrics. Every encounter submitted for reimbursement requires ICD-10-CM diagnosis codes. It's also used in FHIR Condition resources when a billing context is needed.
SNOMED CT vs ICD-10: These are complementary, not competing. SNOMED CT captures clinical detail (the full clinical picture), while ICD-10 captures billing categories (the reimbursable diagnosis). A patient might have a SNOMED problem list entry for their clinical record and a corresponding ICD-10 code for their insurance claim.
Which Standard Should You Use When?
The most common source of confusion is knowing which terminology to apply in which context. This decision guide simplifies the choice.
The simple rule: SNOMED CT for clinical documentation, ICD-10 for billing, LOINC for labs, CPT for procedures, RxNorm for medications. In practice, a single patient encounter will use all five standards simultaneously.
Cross-Standard Mapping: One Concept, Many Codes
A single clinical concept — like Type 2 Diabetes — exists in multiple terminology systems simultaneously, each serving a different purpose.
For a patient with Type 2 Diabetes visiting their doctor:
- SNOMED CT 44054006 — Documents "Type 2 diabetes mellitus" in the clinical problem list
- ICD-10-CM E11.9 — Codes "Type 2 diabetes mellitus without complications" for the insurance claim
- LOINC 4548-4 — Identifies the "Hemoglobin A1c" monitoring test that was ordered
- RxNorm 860975 — Identifies "Metformin 500 MG Oral Tablet" prescribed for treatment
- CPT 99213 — Codes the office visit for billing
All five codes describe aspects of the same encounter. Cross-standard mapping — maintained through FHIR ConceptMap resources and NLM mapping services — connects these codes and enables comprehensive data exchange.
RxNorm: Normalizing Medication Names
Medications are named differently across systems. Your EHR might call it "metformin HCl 500mg tablet," your pharmacy "GLUCOPHAGE 500MG TAB," and your payer "metformin hydrochloride 500 MG oral tablet." RxNorm provides the Rosetta Stone.
RxNorm organizes drug information in a hierarchy from generic ingredients to specific branded products. Each concept has a unique identifier (CUI) that serves as the universal reference point across systems.
When to use RxNorm: Medication reconciliation, e-prescribing, drug interaction checking, formulary management. RxNorm is required by USCDI for medication data and is the primary terminology for FHIR MedicationRequest and MedicationDispense resources.
Implementation Checklist
Implementing healthcare terminology standards is a multi-year journey for most organizations. This checklist helps you prioritize.
Start with what's mandated (ICD-10 for billing, LOINC for labs, RxNorm for medications), then expand to what's recommended (SNOMED CT for clinical documentation, cross-standard mapping). Terminology governance — the ongoing process of maintaining code mappings and training staff — is where most organizations underinvest.
For context on how terminology standards fit into the broader interoperability picture, see Healthcare Interoperability Guide. For FHIR implementation context, see What is FHIR?
Need help with terminology mapping or implementation? Our healthcare integration team has deep expertise in SNOMED CT, LOINC, ICD-10, and cross-standard mapping for FHIR-based systems.