Why Healthcare Still Can't Share Data in 2026
A patient walks into an emergency room after a car accident. The ER physician needs their medication list, allergy history, recent lab results, and surgical history — all sitting in three different healthcare systems across two states. In 2026, getting that data still takes phone calls, faxes, and precious minutes that could determine outcomes.
This is the interoperability problem. And despite billions of dollars in investment, decades of standards development, and federal mandates with million-dollar penalties — healthcare remains one of the least interoperable industries on earth.
This guide maps the entire interoperability landscape: the standards, the regulations, the networks, and the practical steps your organization needs to take. Whether you're a CIO building a multi-year strategy or a product manager scoping your first integration, this is the reference you'll come back to.
The Healthcare Interoperability Ecosystem
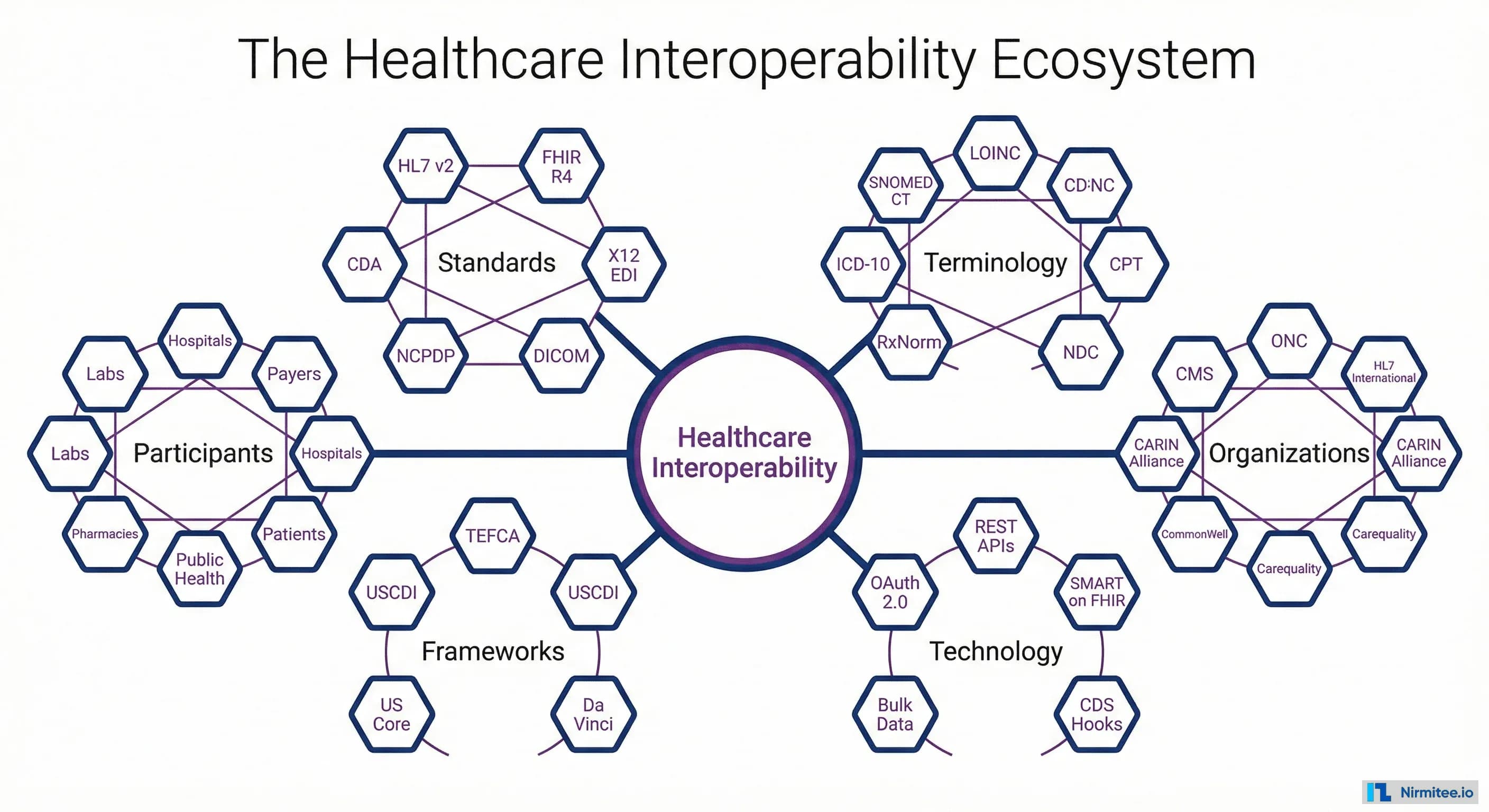
Healthcare interoperability isn't a single technology or standard — it's an ecosystem of interconnected standards, organizations, terminologies, and frameworks that must work together. Understanding this ecosystem is the first step to navigating it.
The ecosystem has six pillars:
- Messaging Standards — HL7 v2, FHIR R4, CDA, X12 EDI, DICOM — the languages systems use to communicate.
- Terminology Standards — SNOMED CT, LOINC, ICD-10, CPT, RxNorm — the shared vocabularies that ensure data means the same thing everywhere.
- Regulatory Bodies — ONC, CMS, HL7 International — the organizations setting rules and standards.
- Technology — REST APIs, OAuth 2.0, SMART on FHIR, CDS Hooks — the technical building blocks.
- Frameworks — TEFCA, USCDI, US Core profiles — the agreements that make nationwide exchange possible.
- Participants — Hospitals, payers, labs, pharmacies, patients, public health — everyone who needs to share data.
The Cost of Poor Interoperability
Before diving into solutions, it's important to quantify why this matters. Poor interoperability isn't just an IT inconvenience — it's a clinical safety risk and a massive financial drain.
The numbers are staggering:
- $30 billion wasted annually on administrative complexity caused by data silos and manual processes
- 18% of medical errors are linked to data gaps between healthcare systems — missing allergies, unknown medications, absent surgical history
- 86% of providers report that faxing remains their primary method for sharing data with external organizations
- The average patient has records scattered across 19 different healthcare systems
- Physicians spend an average of 40 minutes per day searching for patient information that should be readily available
Every one of these problems is solvable with modern interoperability infrastructure. The question isn't whether to invest — it's how to invest wisely.
The Interoperability Standards Stack
Healthcare interoperability works in layers, just like networking. Each layer builds on the one below it. Understanding the stack helps you identify where your organization's gaps are and what to prioritize.
Layer 1 — Transport: How data moves between systems. TCP/IP, HTTPS, SFTP, MLLP. This is mostly solved — nearly all healthcare organizations have network connectivity.
Layer 2 — Messaging: The format of messages exchanged. HL7 v2 (legacy), FHIR REST (modern), X12 EDI (claims), Direct Messaging (secure email). This layer determines what your integration engine needs to support.
Layer 3 — Content: The clinical documents and resources being exchanged. CDA/CCDA documents, FHIR Resources, Blue Button data. This defines what data is shared.
Layer 4 — Terminology: The coded vocabularies that ensure shared meaning. SNOMED CT for clinical findings, LOINC for lab tests, ICD-10 for diagnoses, CPT for procedures, RxNorm for medications. This is where most organizations struggle. You can send a message in the right format but with the wrong codes, and the receiving system can't use it.
Layer 5 — Applications: What uses the data. Patient portals, clinical decision support, population health analytics, quality reporting. This is where interoperability delivers value.
TEFCA: The National Network Taking Shape
The Trusted Exchange Framework and Common Agreement (TEFCA) is the federal government's answer to nationwide health information exchange. After years of development, TEFCA launched in 2023 and is rapidly becoming the backbone of cross-organizational data exchange in the US.
TEFCA works through Qualified Health Information Networks (QHINs) — organizations certified to facilitate data exchange under the TEFCA framework. The current QHINs include CommonWell Health Alliance, Carequality, eHealth Exchange, KONZA, MedAllies, and Health Gorilla.
Key TEFCA capabilities:
- Query-based exchange — Find and retrieve patient records from any participating organization nationwide
- Message delivery — Push clinical documents to specific recipients
- Individual access services — Patients can request their records from any TEFCA participant
What this means for your organization: Connecting to a QHIN gives you access to the national network without building individual connections to every other healthcare organization. If you're planning cross-organizational data exchange, TEFCA should be your primary strategy.
USCDI: The Minimum Data Set
The United States Core Data for Interoperability (USCDI) defines the minimum set of data classes that must be exchangeable between healthcare systems. It's the answer to "what data do we need to share?"
USCDI v3 includes data classes for patient demographics, problems/conditions, medications, allergies, vital signs, lab results, procedures, clinical notes, immunizations, health insurance, goals, assessments, care team, provenance, diagnostic imaging, and social determinants of health (SDOH).
USCDI is updated annually by ONC, with each version expanding the required data set. Healthcare IT vendors certified under the ONC Health IT Certification Program must support the current USCDI version.
The Regulatory Landscape: What's Required and When
Healthcare interoperability is no longer voluntary. A cascade of federal regulations now mandates specific interoperability capabilities, with penalties for non-compliance.
The key regulations and their impacts:
21st Century Cures Act (2016) — The foundation. Established information blocking provisions and directed ONC to develop interoperability standards.
ONC Final Rule (2020) — Defined information blocking, established USCDI, and updated Health IT certification requirements.
CMS Interoperability Rules (2020-2026) — Mandated Patient Access APIs (FHIR), Provider Directory APIs, Payer-to-Payer data exchange, and Prior Authorization APIs for Medicare/Medicaid participants.
Information Blocking Penalties — Healthcare organizations that unreasonably restrict electronic health information exchange face penalties of up to $1 million per violation. This applies to providers, health IT developers, and health information exchanges.
Assessing Your Interoperability Maturity
Before building a strategy, you need to know where you stand. This maturity assessment helps you evaluate your current capabilities across five critical dimensions.
Rate your organization across each dimension:
- Data Exchange: Are you still faxing (Level 1), using HL7 v2 point-to-point (Level 2), using an integration engine with FHIR (Level 3), or connected to national networks like TEFCA (Level 4)?
- Terminology Standards: Are you using local codes (Level 1), partially mapped to standard terminologies (Level 2), fully coded with SNOMED/LOINC/ICD-10 (Level 3), or actively maintaining terminology governance (Level 4)?
- Security and Consent: Basic authentication (Level 1), role-based access (Level 2), OAuth 2.0/SMART (Level 3), or granular consent management with FHIR Consent resources (Level 4)?
- Governance: No formal governance (Level 1), documented policies (Level 2), active data governance committee (Level 3), or participating in cross-organizational governance frameworks (Level 4)?
- Patient Access: No patient access (Level 1), patient portal (Level 2), FHIR Patient Access API (Level 3), or TEFCA Individual Access Services (Level 4)?
Most healthcare organizations score between Level 2 and Level 3. The regulatory environment is pushing everyone toward Level 3-4 by 2027.
Your Interoperability Action Plan
Regardless of where you are on the maturity spectrum, the path forward follows the same six steps.
- Assess your current state. Inventory every system, every interface, every data flow. Map where data moves — and where it doesn't. Score yourself on the maturity matrix above.
- Define your use cases. Prioritize by three criteria: clinical impact (does this affect patient safety?), compliance requirements (is there a regulatory deadline?), and ROI (what's the financial benefit?).
- Choose your standards. FHIR R4 for all new development. Maintain HL7 v2 for existing interfaces. Map to standard terminologies (SNOMED, LOINC, ICD-10). Plan for USCDI compliance.
- Select your technology. Integration engine (Mirth Connect for open-source, Rhapsody for enterprise), FHIR server (HAPI FHIR or vendor-provided), and terminology service for code mapping.
- Build and test. Phased implementation starting with highest-priority use cases. Thorough testing including conformance validation (Inferno, Touchstone), load testing, and security audit.
- Monitor and optimize. Track message volumes, error rates, latency, and compliance metrics. Continuously improve mappings and add new integrations.
For detailed guidance on specific standards and technologies, see our companion guides: What is HL7?, What is FHIR?, HL7 Integration Playbook, and Mirth Connect Guide.
Need help building your interoperability strategy? Our healthcare integration team works with hospitals and health systems across the US — from assessment through production deployment.