Here is a question that separates healthcare startups that scale from those that stall: what happens to your cost per transaction when you go from 1,000 customers to 10,000?
For most healthcare SaaS companies, the honest answer is uncomfortable. Costs scale almost linearly. Revenue grows, but so does headcount. Margins stay flat or compress. And when investors dig into the unit economics during Series A due diligence, this is exactly what kills deals.
The culprit is not your technology stack. It is the manual workflows hiding inside your product — the ones your team has normalized because "that is just how healthcare works."
The Hidden Manual Workflow Problem
Every healthcare SaaS product has them. They are the workflows that look automated from the customer's perspective but require human intervention behind the scenes. We have built over 20 healthcare applications, and we see the same pattern in nearly every product:
- Prior authorization follow-ups — Your system submits the auth request automatically, but someone on your team manually checks payer portals for status updates because the X12 278 response is unreliable or delayed.
- Insurance eligibility exceptions — The 270/271 transaction handles 60-70% of verifications cleanly. The rest require someone to call the payer, navigate an IVR, or log into a portal to resolve discrepancies.
- Clinical document classification — Documents arrive as PDFs, faxes, and scanned images. Your system routes the obvious ones, but 30-40% need a human to read the document, determine what it is, and file it correctly.
- Claim denial management — Denials arrive with remark codes, but the actual resolution requires reading EOBs, understanding the specific denial reason, and determining the right corrective action.
- Patient data reconciliation — When data arrives from multiple sources with conflicting information, someone has to manually review and decide which version is correct.
Each of these workflows requires skilled healthcare operations people. They are expensive. They are hard to hire. And critically, you need more of them as your customer base grows.
How This Shows Up in Investor Due Diligence
Sophisticated healthcare investors have seen this pattern hundreds of times. During due diligence, they look for specific signals:
Headcount-to-revenue ratio. If your operations team grows at 70-80% the rate of your revenue, you have a services business disguised as a software company. Software companies scale at 20-30% headcount growth relative to revenue growth. The gap is the manual workflow problem.
Gross margin trajectory. True SaaS businesses have gross margins of 70-85% that improve as they scale. Healthcare SaaS companies with hidden manual workflows often have gross margins of 45-60% that stay flat or decline. Every new customer adds revenue and costs in roughly equal proportion.
Customer onboarding time. If onboarding a new customer takes 6-12 weeks because your team has to configure rules, train on the customer's specific payer mix, and set up manual review queues, that is a unit economics red flag. It means your marginal cost of a new customer is high, and your time-to-revenue is slow.
Support ticket composition. When 40-50% of support tickets are actually your team doing work that the product should handle — resolving exceptions, fixing data, completing workflows — that is manual cost masquerading as customer support.
Investors do not always articulate it this way, but what they are really asking is: does this company have software economics or services economics? Manual workflows are what tip the answer toward services.
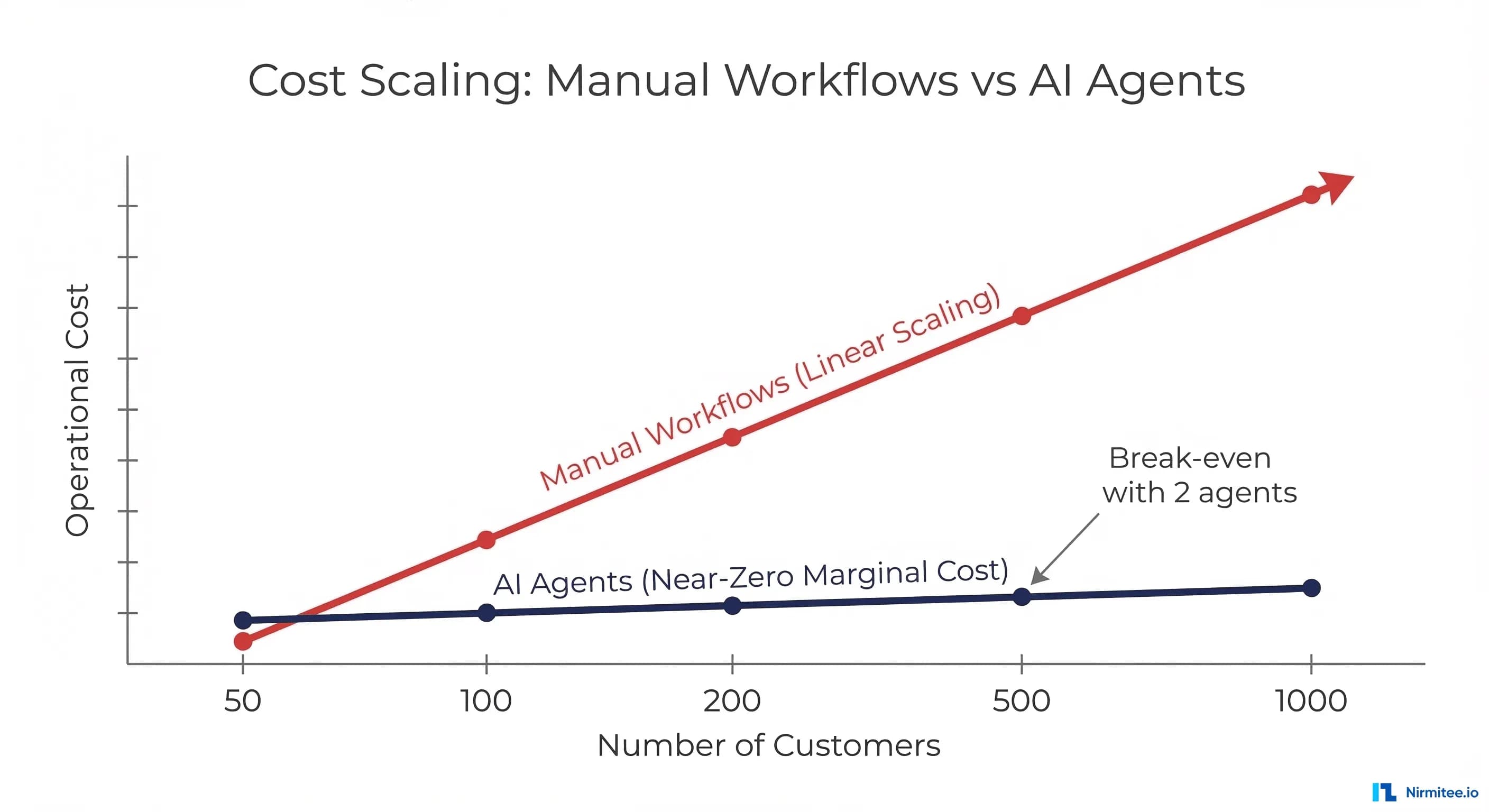
The Math: Linear vs. Near-Zero Marginal Cost
Let us make this concrete with numbers from a real pattern we see across healthcare SaaS products.
Linear cost model (manual workflows):
- 1,000 customers: 15 operations staff handling exceptions, cost $1.2M/year
- 5,000 customers: 68 operations staff, cost $5.4M/year
- 10,000 customers: 130 operations staff, cost $10.4M/year
- Cost per customer: stays at roughly $1,000-1,100/year regardless of scale
Near-zero marginal cost model (agent-powered workflows):
- 1,000 customers: 4 operations staff overseeing agents, cost $320K/year + $180K compute = $500K
- 5,000 customers: 6 operations staff, cost $480K + $400K compute = $880K
- 10,000 customers: 8 operations staff, cost $640K + $700K compute = $1.34M
- Cost per customer: drops from $500 to $176 to $134 as you scale
The difference at 10,000 customers is $9M per year in operational costs. That is not a rounding error — it is the difference between a 45% gross margin and an 80% gross margin. It is the difference between a company valued at 8x revenue and one valued at 15-20x revenue.
The key insight is not just that agents are cheaper. It is that agent costs scale sub-linearly. Compute costs increase with volume, but at a fraction of the rate of human labor costs. And the agents get better over time — they handle more edge cases, require fewer escalations, and process faster — while human teams have a learning curve with every new hire.
Specific Workflows and Their Scaling Behavior
Not all manual workflows respond equally to agent automation. Here is how we evaluate which ones to target first:
Prior authorization status checking — High impact, immediate ROI. An agent can poll payer APIs, parse X12 278 responses, handle the common exceptions (wrong member ID format, missing clinical data), and escalate only truly unusual cases. We see 85-90% automation rates within the first month. The remaining 10-15% are edge cases that the agent flags with full context for human review, making even the manual work faster.
Clinical document classification — High impact, builds over time. An LLM-based agent reads the document, classifies it against standard categories (lab result, discharge summary, referral letter, operative note, etc.), extracts key data points, and routes it to the right place. Initial accuracy is typically 88-92%, improving to 96-98% within three months as the feedback loop captures corrections. The volume of documents that need human review drops from 35% to under 5%.
Insurance eligibility resolution — Medium-high impact, variable by payer. For payers with good API support, the agent handles exceptions by trying alternative identifiers, checking secondary coverage, and resolving common mismatches. For payers that still require portal access, the agent uses LLM-powered browser automation that understands page content semantically rather than relying on fixed element positions. Automation rates vary from 75% to 95% depending on payer mix.
Claim denial analysis — High impact, requires domain depth. The agent reads denial codes and EOB details, maps them to resolution strategies, determines whether to appeal or correct and resubmit, and drafts the appropriate response. This is where healthcare domain knowledge in the agent's prompt engineering makes the biggest difference. Generic LLM approaches achieve 60-70% accuracy. Domain-tuned agents with proper FHIR integration and payer-specific rule sets achieve 90-95%.
Patient data reconciliation — Medium impact, high complexity. Matching and merging patient records from multiple sources requires the agent to weigh multiple signals: demographic similarity, temporal context, clinical plausibility. This is typically the last workflow to automate because the consequences of errors are highest. We recommend starting with agent-assisted reconciliation (agent suggests, human confirms) before moving to agent-autonomous for high-confidence matches.
The Agent Economics Flywheel
The real power of agent-based unit economics is not a one-time cost reduction. It is a flywheel that compounds over time:
More customers generate more transaction volume. In the manual model, this is a problem — more volume means more staff. In the agent model, more volume means more data for the agent to learn from.
Agents handle the volume at near-zero marginal cost. Each additional transaction costs fractions of a cent in compute versus dollars in human labor. The cost curve flattens as volume grows.
Higher margins fund growth. The operational savings go directly to your bottom line or get reinvested in product development. You can afford to acquire customers at higher CAC because your LTV is structurally higher. You can invest in building more agents for more workflows.
Better agents attract more customers. As your agents handle more edge cases and achieve higher automation rates, your product becomes demonstrably better. Faster turnaround, fewer errors, more consistent results. This is a competitive advantage that compounds — your agents have seen more data patterns than a new competitor's agents ever have.
Agent improvements transfer across customers. When an agent learns to handle a new payer's denial pattern from Customer A's data, Customer B automatically benefits. In the manual model, each operations team member's knowledge is siloed. In the agent model, learning is shared infrastructure.
This flywheel is why the gap between agent-powered and manually-operated healthcare SaaS companies will widen exponentially over the next 3-5 years. The companies that start building agents now will have compounding advantages that late movers cannot quickly replicate.
How to Present This to Investors and Your Board
If you are raising a Series A or presenting to your board, here is how to frame the agent economics story credibly:
Do not claim you will eliminate all manual work. Investors are skeptical of anyone who says AI will replace humans entirely. Instead, show the specific workflows you are automating, the current automation rates, and the trajectory. "We have automated 87% of prior auth follow-ups and are improving at 2-3% per month" is more credible than "Our AI handles everything."
Show the cost-per-transaction trend. Build a chart that shows cost per transaction declining over time as agent automation rates increase. This is the single most powerful unit economics slide you can present. It shows investors that your cost structure is improving with scale, not staying flat.
Quantify the margin expansion. Show your current gross margin, your projected gross margin at 3x and 10x current scale with agents, and contrast it with what the margin would be if you scaled with manual operations. The delta is your agent ROI story.
Demonstrate the feedback loop. Show how human corrections improve the agent. This addresses the "what if the AI is wrong" concern by showing that errors are self-correcting. Every human override trains the agent to handle that case next time. Show the escalation rate declining month-over-month as evidence.
Frame it as a moat. Your agent is not a generic AI tool. It is trained on your specific healthcare workflows, your payer relationships, your clinical data patterns. Every transaction it processes makes it harder for competitors to replicate. This is a data network effect — the more you process, the better you get, the more customers you win, the more you process.
Address the build vs. buy question. Investors will ask why you are building agents in-house versus using an off-the-shelf solution. The answer is domain specificity. Generic AI tools cannot handle the nuance of healthcare workflows — the payer-specific rules, the clinical context, the compliance requirements. Your agents encode your domain knowledge, which is your competitive advantage.
The Bottom Line
The hidden manual workflow problem is the single biggest threat to healthcare SaaS unit economics. It turns what should be a software business into a services business, compresses margins, limits scale, and ultimately caps your valuation.
AI agents do not just reduce costs — they fundamentally change the cost structure from linear to sub-linear. Every additional customer generates revenue with minimal additional cost. Margins expand as you grow instead of staying flat. And the flywheel effect means the gap between your unit economics and your manually-operated competitors widens every quarter.
The math is straightforward. The technology is available. The question is whether you restructure your unit economics now — while the competitive advantage is still available — or wait until your investors and your market force the issue.
Looking to build a robust healthcare platform? Our Healthcare Software Product Development team turns complex requirements into production-ready systems. We also offer specialized Agentic AI for Healthcare services. Talk to our team to get started.