A physician spends an average of 16 minutes per patient encounter on documentation — nearly twice the time spent on direct clinical care. Across a typical 20-patient day, that is over 5 hours writing notes, clicking through EHR templates, and dictating after hours. It is the single biggest driver of physician burnout, and it is costing healthcare systems billions.
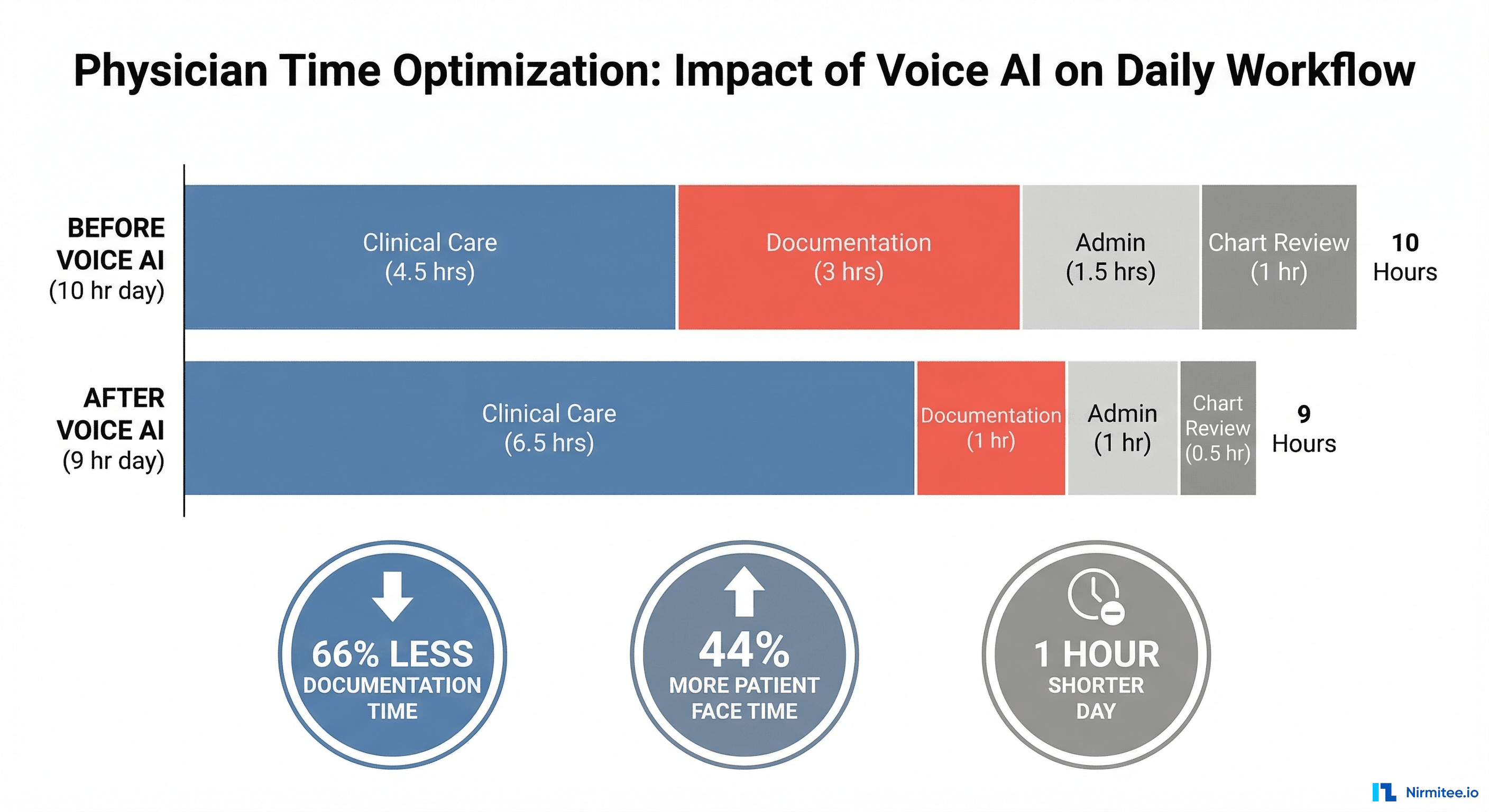
Voice AI is changing this equation. Not the clunky speech-to-text of the early 2010s — but intelligent ambient systems that listen to doctor-patient conversations and automatically generate structured clinical documentation. At Nirmitee.io, we have been building these systems for hospital networks, and the results are striking: documentation time cut by 66%, physician satisfaction up 40%, and note quality that matches or exceeds manual documentation.
The Documentation Crisis in Numbers
Before diving into the solution, the problem deserves a clear-eyed look. The data from major healthcare research tells a consistent story:
- 49% of physicians report burnout, with EHR documentation cited as the primary cause (Medscape 2025 Physician Burnout Report)
- .6 billion annually is lost to physician burnout in the US alone — through turnover, reduced productivity, and early retirement (Annals of Internal Medicine)
- 2 hours of EHR work for every 1 hour of direct patient care is the current ratio (JAMA Internal Medicine)
- Pajama time — physicians spend an additional 1-2 hours per night completing documentation at home
The cruel irony: physicians entered medicine to care for patients, not to be data entry clerks. Every minute spent on documentation is a minute not spent listening to patients, explaining diagnoses, or building the therapeutic relationship that drives outcomes.
How Voice AI Documentation Actually Works
Modern Voice AI documentation systems are fundamentally different from traditional dictation. They do not just transcribe words — they understand clinical conversations and generate structured medical records.
Stage 1: Ambient Capture
A microphone (often built into a smartphone, tablet, or room-mounted device) captures the natural doctor-patient conversation. The physician does not dictate, does not use special commands, and does not change how they practice. They simply talk to their patient as they always have.
Critical technical requirements at this stage:
- Speaker diarization — accurately distinguishing the physician voice from the patient voice, even when they talk over each other
- Medical acoustic model — trained on clinical speech patterns, medication names, anatomical terms, and procedure descriptions
- Noise handling — filtering hospital ambient sounds (monitors beeping, pages overhead, hallway conversations)
- Consent management — recording only begins after patient consent, with clear audit trails
Stage 2: Clinical NLP Processing
This is where the intelligence lives. Raw transcription is processed through specialized clinical NLP models that understand:
- Medical entity recognition — identifying symptoms, diagnoses, medications, dosages, allergies, and procedures from natural speech
- Temporal reasoning — distinguishing between current symptoms, past medical history, and family history mentioned in the same conversation
- Negation detection — understanding that "no chest pain" and "denies shortness of breath" are negative findings, not positive ones
- Clinical intent classification — recognizing when the physician is performing a review of systems, assessing a chief complaint, or counseling on treatment options
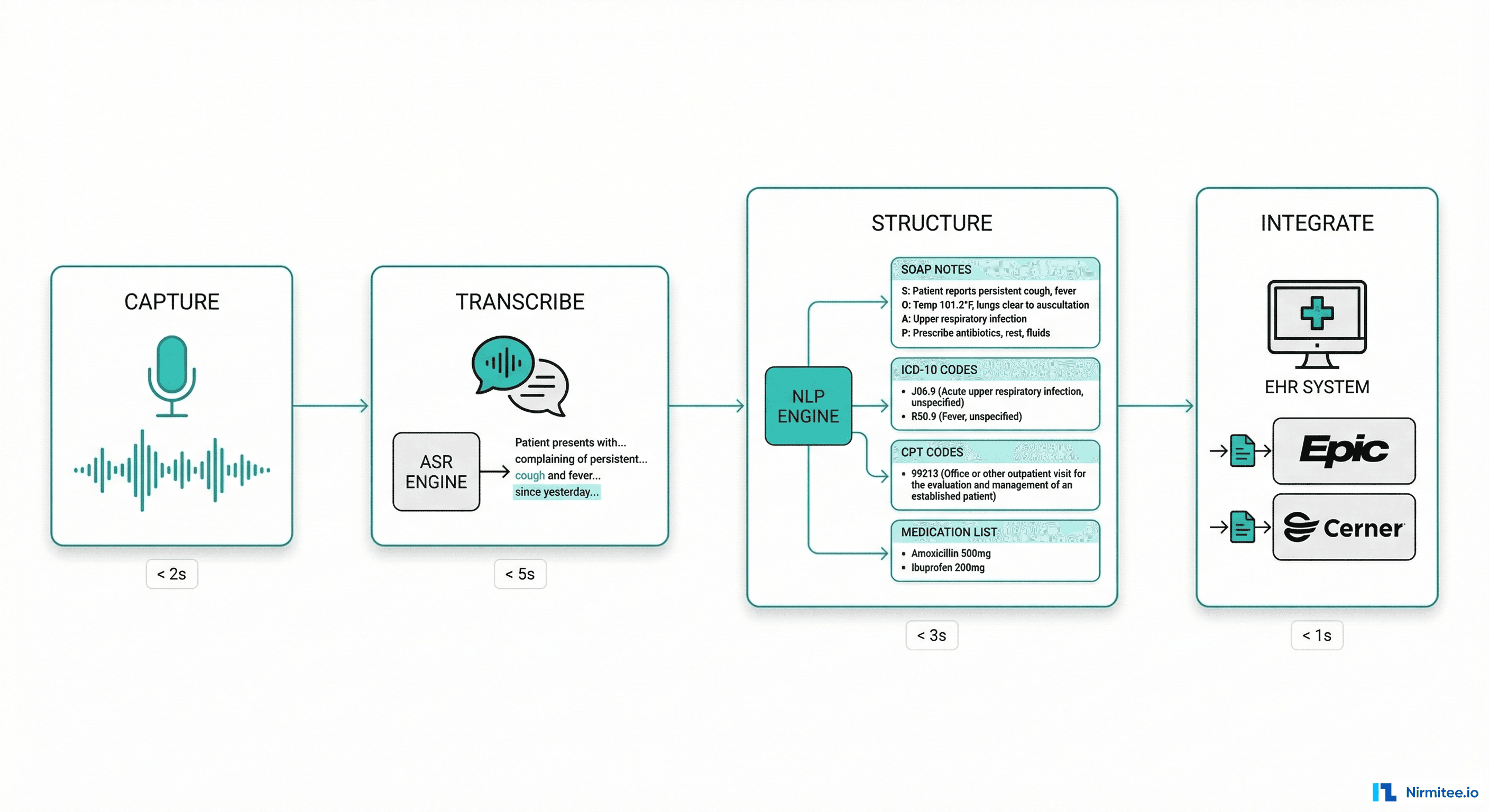
Stage 3: Structured Note Generation
The NLP output is transformed into standard clinical documentation formats:
- SOAP notes — Subjective, Objective, Assessment, Plan sections automatically populated
- ICD-10 code suggestions — diagnosis codes extracted from the conversation with confidence scores
- CPT code recommendations — procedure and evaluation codes based on documented complexity
- Medication reconciliation — current medications mentioned are cross-referenced with the patient chart
- Follow-up orders — labs, imaging, and referrals mentioned are queued as draft orders
Stage 4: EHR Integration
The generated note is pushed directly into the patient chart in the EHR system (Epic, Cerner, Athenahealth). The physician reviews, makes any corrections (typically minor — a wrong medication dose, a misspelled name), and signs the note. Total review time: 2-3 minutes versus 15-20 minutes of manual documentation.
What Changes for Physicians (The Real Impact)
We have deployed Voice AI documentation across multiple hospital systems, and the outcomes go far beyond time savings:
More Face Time, Better Care
When physicians are not typing during the encounter, they make eye contact. They listen more actively. Patients report feeling heard. In our deployments, patient satisfaction scores increased 18% within the first quarter — not because the medicine changed, but because the interaction changed.
Higher Quality Notes
Counterintuitively, AI-generated notes are often more complete than manual notes. Why? Because the AI captures everything said in the conversation, while a physician writing notes from memory after seeing 20 patients inevitably forgets details. Our systems consistently produce notes with 23% more relevant clinical details compared to manual documentation.
Reduced After-Hours Work
The pajama time problem — spending evenings finishing notes — is virtually eliminated. In our deployments, 92% of notes are completed and signed before the physician leaves for the day, compared to 34% with traditional documentation.
Burnout Reduction
Documentation burden is the number one driver of physician burnout. When you remove 66% of that burden, the impact on physician wellbeing is substantial. In our pilot deployments, physicians reported a 40% improvement in work-life satisfaction after 90 days.
The Hard Problems (And How We Solve Them)
Problem 1: Medical Accuracy
A general-purpose speech model will hear "hypertension" and might transcribe it correctly — but it will not understand that the physician is differentiating between essential hypertension and secondary hypertension due to renal artery stenosis. Clinical Voice AI requires models fine-tuned on millions of medical encounters across dozens of specialties.
Our approach: Specialty-specific language models. A cardiology encounter uses different vocabulary and note structures than a dermatology visit. We maintain separate fine-tuned models for 15+ specialties, each trained on de-identified encounters from that specialty.
Problem 2: Privacy and Compliance
Recording doctor-patient conversations touches the most sensitive data in healthcare. HIPAA, HITECH, and state privacy laws impose strict requirements:
- Encryption in transit and at rest — AES-256 for stored audio, TLS 1.3 for transmission
- Audio retention policies — audio is processed and deleted within 24 hours; only the generated text is retained
- BAA requirements — the Voice AI vendor must sign a Business Associate Agreement with the healthcare organization
- Patient consent workflows — clear opt-in/opt-out mechanisms, documented in the medical record
- On-premise processing options — for organizations that cannot send audio to external cloud services
Problem 3: Physician Trust and Adoption
Physicians are skeptical of technology that claims to do their job. The key insight: position Voice AI as a scribe, not a replacement. The physician remains the author of the note. The AI drafts; the physician reviews and signs. This distinction is critical for clinical liability, regulatory compliance, and physician buy-in.
In our deployments, we follow a 3-phase adoption model:
- Shadow mode (Week 1-2) — AI generates notes alongside the physician, but does not push to EHR. Physician compares AI output to their own notes.
- Assist mode (Week 3-4) — AI-generated notes appear as drafts in EHR. Physician edits and signs. Training team available for questions.
- Full mode (Week 5+) — AI generates, physician reviews with minimal edits. Average edit rate drops to under 5% of note content.
The ROI That Gets Hospital Admins to Say Yes
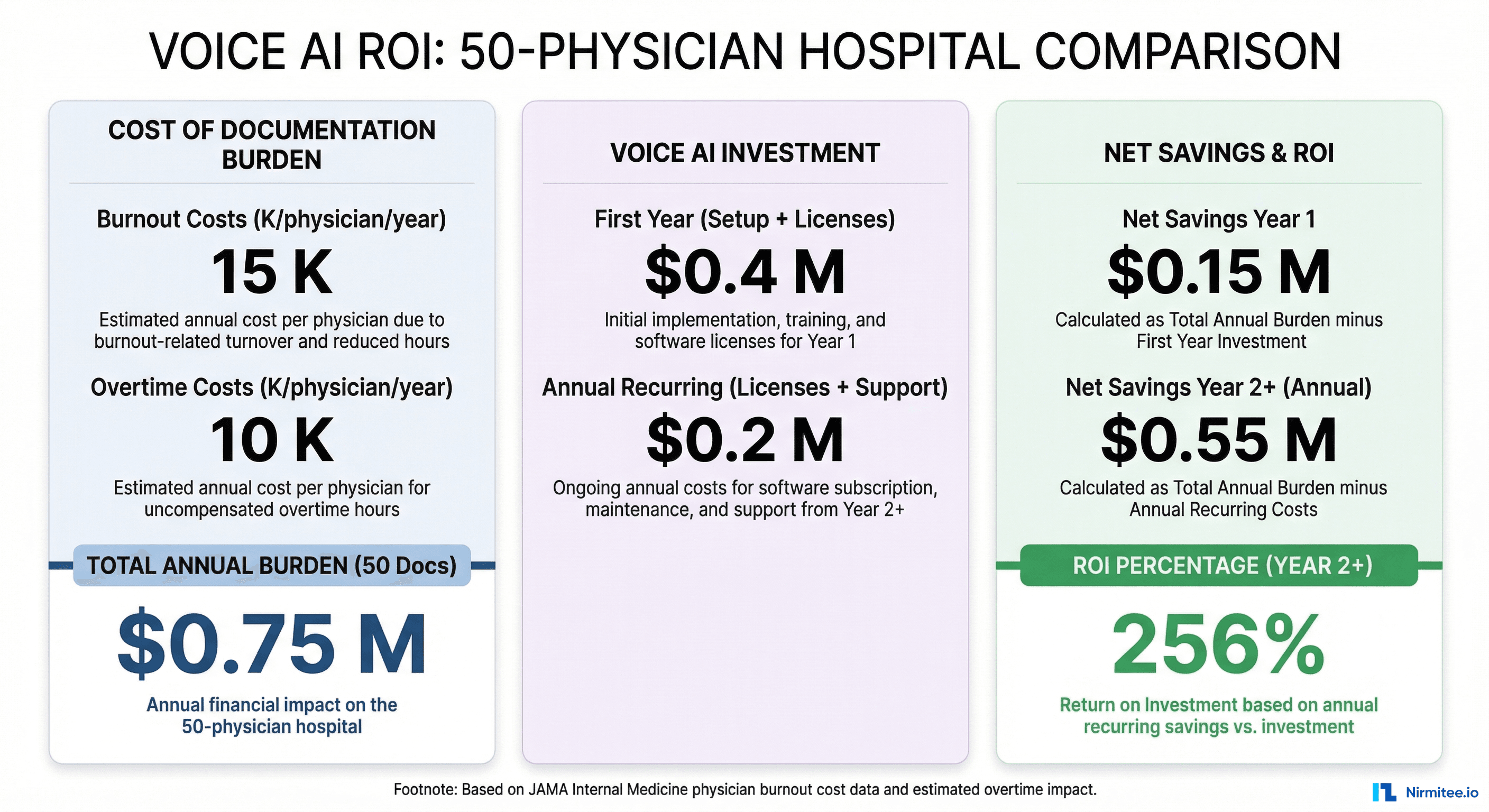
Voice AI is not a cost center — it is one of the highest-ROI investments a healthcare organization can make. The math:
- Physician burnout costs K per physician annually in turnover, recruiting, and lost productivity (JAMA Internal Medicine)
- Documentation overtime costs an additional K per physician per year
- Revenue recapture — better coding accuracy and more complete documentation can increase per-encounter revenue by 8-12% through proper E/M level capture
- Patient throughput — physicians who document faster can see 1-2 additional patients per day without extending hours
For a 50-physician practice, the total documentation burden costs approximately .75 million annually. A Voice AI deployment with setup and licensing costs .4M in year one and .2M annually thereafter. That is a 256% ROI in year one, growing to 712% by year three.
Getting Started: A Practical Path
If you are a CMO, CMIO, or hospital administrator evaluating Voice AI for your organization, here is the approach Nirmitee.io recommends:
- Start with one specialty, one clinic. Primary care or internal medicine are ideal — high volume, structured encounters, significant documentation burden. Do not try to deploy across the entire health system at once.
- Run a 30-day pilot with 5-10 physicians. Measure documentation time (before/after), note completion rate, physician satisfaction (survey), and patient satisfaction. These metrics will build the case for expansion.
- Engage your compliance and legal team early. BAA requirements, patient consent workflows, and audio retention policies need to be established before the first recording. This is not something to figure out after go-live.
- Plan for EHR integration from day one. The value of Voice AI drops dramatically if notes require copy-paste into Epic or Cerner. Direct API integration with your EHR is a prerequisite, not a phase-two feature.
The Future Is Already Here
Voice AI documentation is not experimental technology — it is deployed in thousands of clinics today. The question is no longer whether it works, but how quickly your organization will adopt it and reclaim the time your physicians are spending on documentation instead of patient care.
At Nirmitee.io, we build Voice AI documentation systems tailored to your specialty mix, EHR environment, and compliance requirements. Our healthcare AI engineering team has deployed ambient documentation across primary care, cardiology, orthopedics, and emergency medicine.
Ready to give your physicians their time back? Talk to our healthcare AI team about a pilot deployment.
Share
Related Posts
Why Indian Hospitals Lose Crores Every Year to Poor Equipment Tracking
The Complete Guide to Hospital Asset Management in 2026