The Prior Authorization Crisis in Healthcare
Prior authorization (PA) — the process where healthcare providers must get approval from insurance companies before delivering certain treatments — has become one of the biggest bottlenecks in American healthcare. According to the American Medical Association (AMA), physicians complete an average of 45 prior authorization requests per week, with each request taking 12-14 business days for a decision. The result? Delayed patient care, physician burnout, and billions in administrative waste.
At Nirmitee.io, we partnered with a mid-sized health system (200+ bed hospital, 50+ outpatient clinics) to deploy an AI-powered multi-agent system that automates 85% of prior authorization workflows — reducing turnaround from 14 days to under 3 hours.
This is the story of how we did it.
Understanding the Problem
Our client's prior authorization department was processing 2,800+ requests per month with a team of 12 PA coordinators. The pain points were severe:
- 14-day average turnaround: Patients waited nearly two weeks for treatment approvals, with some urgent cases taking 5+ days even with expedited review.
- 35% initial denial rate: Over a third of requests were denied on first submission, primarily due to missing clinical documentation or incorrect coding — not because the treatment was medically unnecessary.
- 80% manual touch rate: Nearly every request required a coordinator to manually extract clinical data from the EHR, look up payer-specific requirements, compile documentation, and submit via payer portals.
- $2.4M annual administrative cost: The fully loaded cost of the PA team, including salaries, benefits, training, and technology overhead.
- Physician dissatisfaction: Clinicians spent 20+ minutes per patient on PA-related documentation, pulling them away from direct patient care.
Root Cause Analysis
Before building any technology, we spent three weeks embedded with the PA team to map every step of their workflow. The root causes of delay fell into four categories:
- Data Fragmentation: Clinical data needed for PA requests was spread across the EHR (Epic), lab systems, imaging archives (PACS), and external referral documents. Coordinators spent 40% of their time simply locating and compiling information.
- Payer Rule Complexity: Each of the 15 major payers the hospital worked with had different PA requirements — different forms, different clinical criteria, different submission portals. Rules changed quarterly, and the team struggled to stay current.
- Coding Errors: 60% of initial denials were due to incorrect CPT/ICD-10 code combinations or missing modifier codes, not clinical insufficiency.
- No Feedback Loop: When a request was denied, the denial reason was rarely fed back into the process to prevent the same error on future submissions.
Our Multi-Agent Architecture
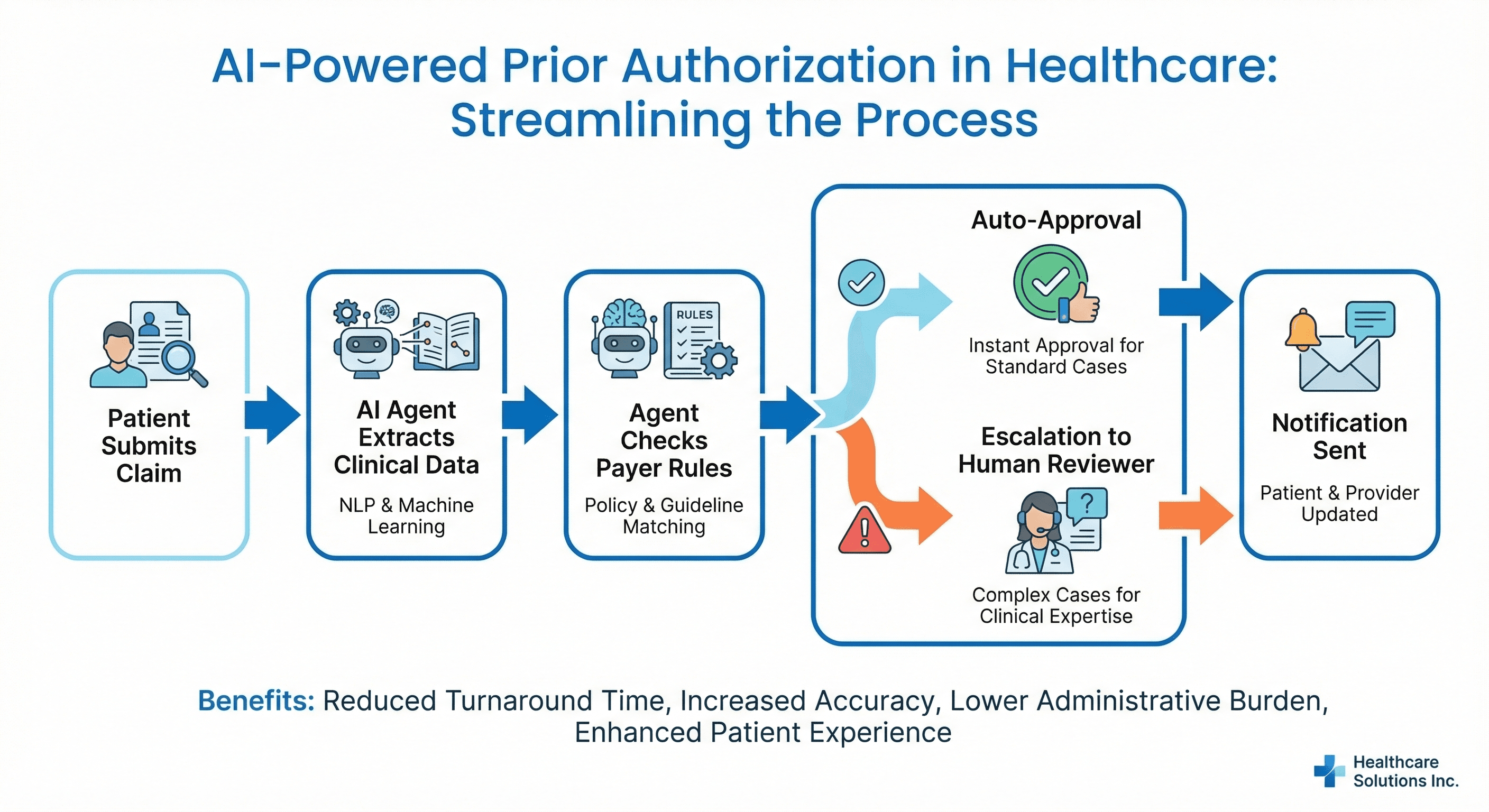
Rather than building a monolithic automation system, we designed a multi-agent architecture where four specialized AI agents collaborate to process each PA request. This approach mirrors how a well-functioning human team operates — each agent has deep expertise in one domain and communicates results to the others.
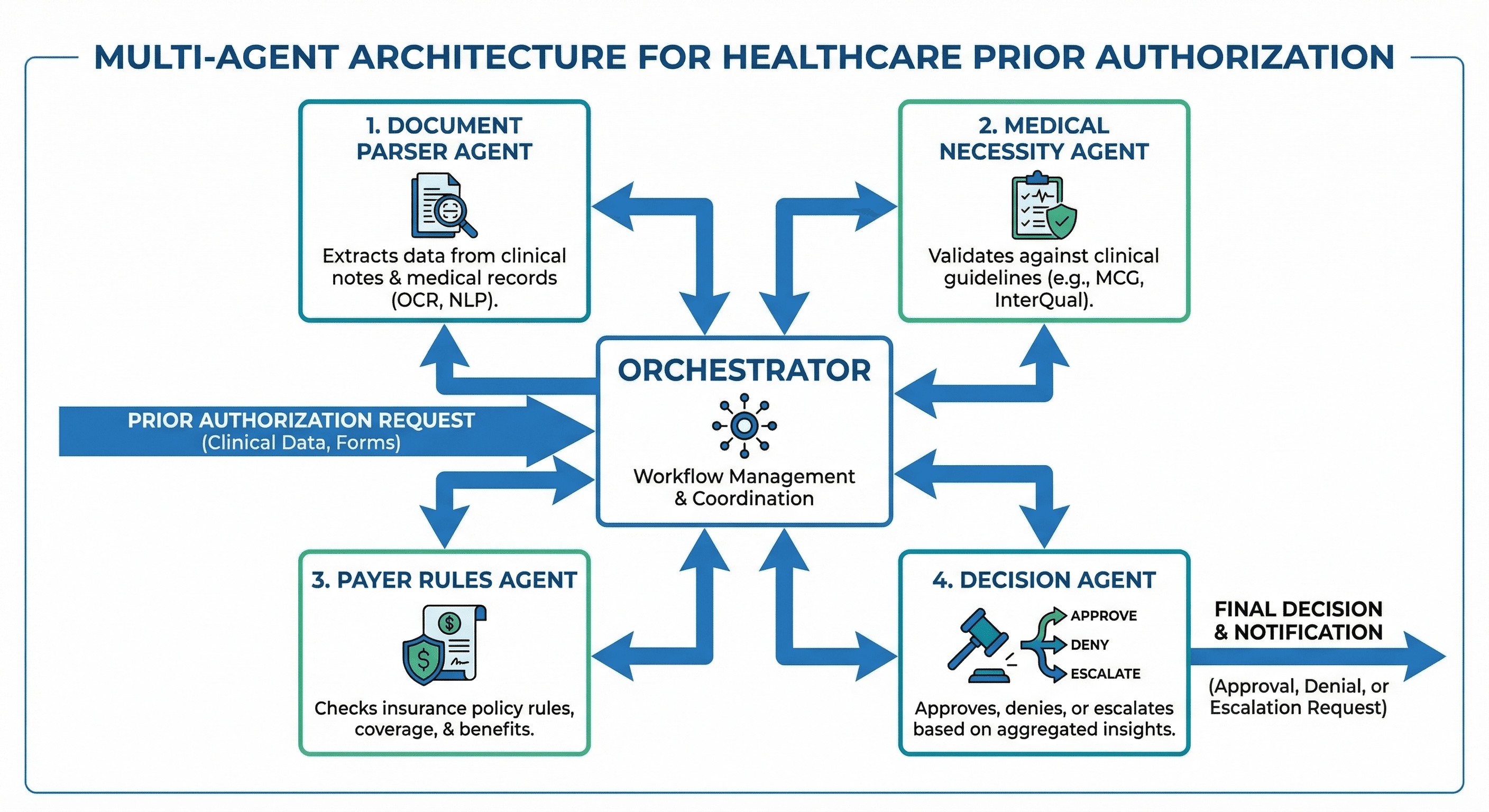
Agent 1: The Document Parser
The Document Parser agent is the first to engage when a PA request is initiated. Its responsibilities include:
- Clinical Note Extraction: Using fine-tuned NLP models to extract structured clinical data from unstructured physician notes, including diagnoses, symptoms, treatment history, and clinical rationale.
- Lab Result Interpretation: Pulling relevant lab values (HbA1c for diabetes medications, eGFR for renal drugs, liver function panels for hepatotoxic drugs) and flagging abnormalities that support medical necessity.
- Imaging Report Analysis: Parsing radiology and pathology reports to extract findings that justify requested procedures.
- Patient History Assembly: Compiling a longitudinal view of the patient's treatment history, including prior failed therapies (critical for step therapy requirements).
The Parser agent processes documents in under 30 seconds — compared to the 15-20 minutes a coordinator would spend manually reviewing charts.
Agent 2: The Medical Necessity Validator
Once clinical data is extracted, the Medical Necessity agent evaluates whether the requested treatment meets evidence-based clinical guidelines:
- Guideline Matching: Cross-references the clinical data against MCG (Milliman Care Guidelines), InterQual criteria, and specialty-specific guidelines (NCCN for oncology, ADA for diabetes, ACC/AHA for cardiology).
- Step Therapy Verification: Confirms that required prior treatments have been attempted and documented before approving next-line therapies.
- Contraindication Check: Identifies if the patient has documented allergies, adverse reactions, or contraindications that justify bypassing standard step therapy protocols.
- Confidence Scoring: Assigns a medical necessity confidence score (0-100). Requests scoring above 85 proceed to auto-approval; those below 60 are flagged for human review.
Agent 3: The Payer Rules Engine
The most complex agent manages the labyrinth of payer-specific requirements:
- Payer Policy Database: Maintains an up-to-date knowledge base of PA requirements for each payer, plan type, and service category — updated weekly via automated payer portal scraping and manual policy review.
- Code Validation: Verifies CPT, ICD-10, HCPCS, and modifier code combinations against payer-specific code edit rules. This alone eliminated 60% of coding-related denials.
- Form Auto-Population: Generates payer-specific PA request forms pre-populated with the correct clinical data, codes, and supporting documentation.
- Submission Routing: Determines the optimal submission channel (electronic via Availity/Surescripts, fax, or payer portal) based on payer preferences and request urgency.
Agent 4: The Decision Orchestrator
The Orchestrator is the supervisory agent that manages the end-to-end workflow:
- Workflow Coordination: Sequences the other three agents, handles retries on failures, and manages parallel processing when multiple PA requests arrive simultaneously.
- Auto-Approval Logic: When all three upstream agents return high-confidence results (medical necessity score greater than 85, code validation passed, payer rules satisfied), the Orchestrator auto-approves and submits the request.
- Intelligent Escalation: Routes low-confidence or edge cases to the appropriate human reviewer — a PA coordinator for administrative issues, or a peer-to-peer physician reviewer for clinical disputes.
- Learning Loop: Captures denial reasons, successful appeal strategies, and human reviewer decisions to continuously improve the system's accuracy.
HIPAA Compliance & Security Architecture
Handling Protected Health Information (PHI) with AI requires rigorous security controls. Our architecture was designed for HIPAA compliance from the ground up:
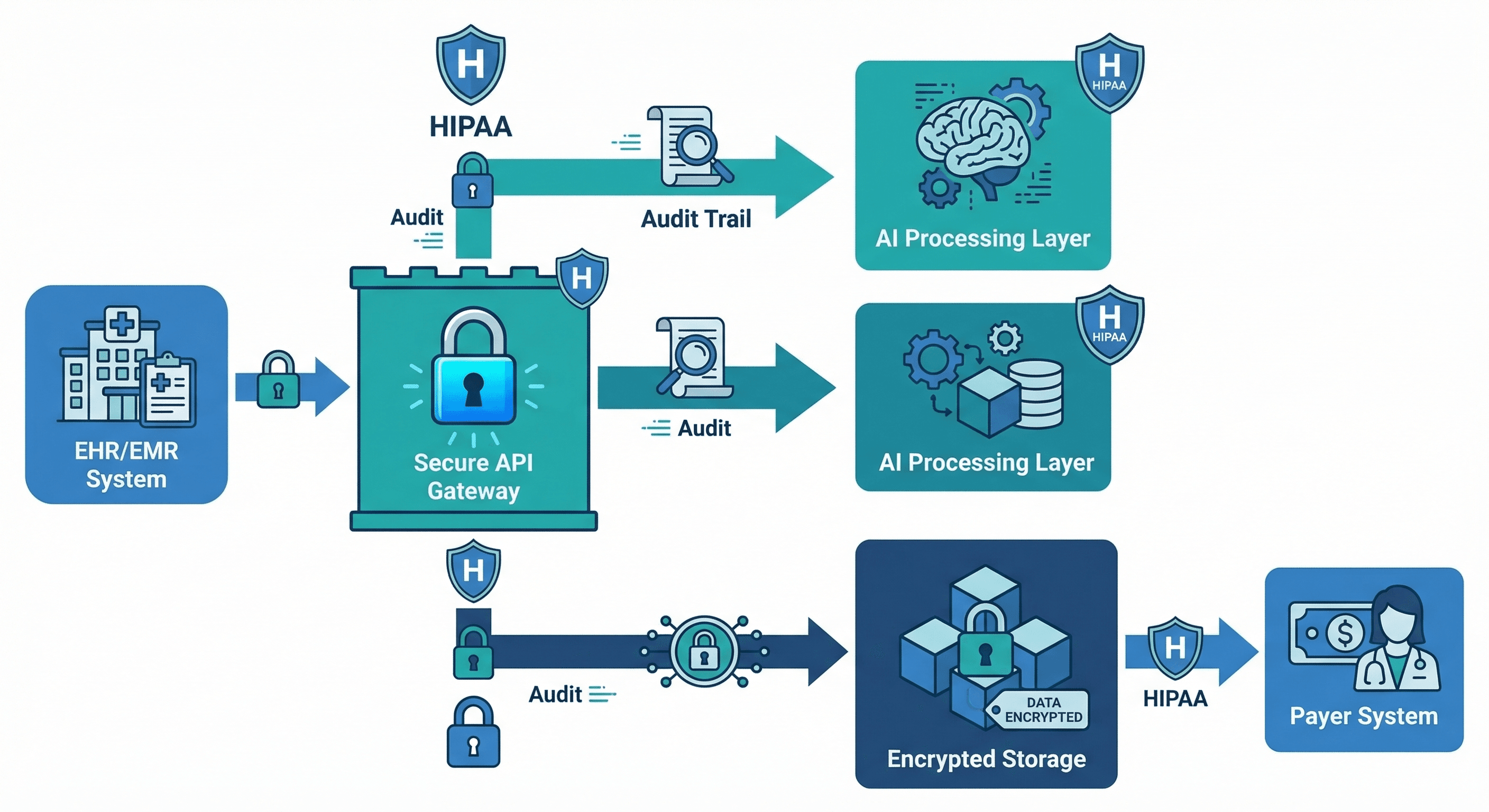
- Data Encryption: All PHI is encrypted at rest (AES-256) and in transit (TLS 1.3). AI processing occurs within the hospital's private cloud — no PHI is sent to external LLM APIs.
- On-Premise LLM Deployment: We deployed fine-tuned open-source models (Llama-based) within the hospital's infrastructure. No patient data leaves the facility perimeter.
- Role-Based Access Control: AI agents operate under service accounts with minimum necessary permissions. The Document Parser can read clinical records but cannot modify them.
- Complete Audit Trail: Every agent action, decision, and data access is logged with timestamps, enabling compliance audits and decision traceability.
- BAA Coverage: Nirmitee.io operates under a signed Business Associate Agreement covering all AI processing activities.
Implementation Timeline
The project was delivered in four phases over 16 weeks:
- Weeks 1-3: Discovery & Design — Workflow mapping, payer rule cataloguing, data source inventory, architecture design.
- Weeks 4-8: Core Development — Agent development, EHR integration (Epic FHIR APIs), payer portal connectors, model fine-tuning on 50,000 historical PA records.
- Weeks 9-12: Testing & Validation — Shadow mode (AI processes alongside humans, results compared but not submitted), accuracy validation against 5,000 test cases, security penetration testing.
- Weeks 13-16: Phased Rollout — Started with radiology PAs (highest volume, most standardized), expanded to pharmacy, then surgical, then all categories.
Results: Before vs After
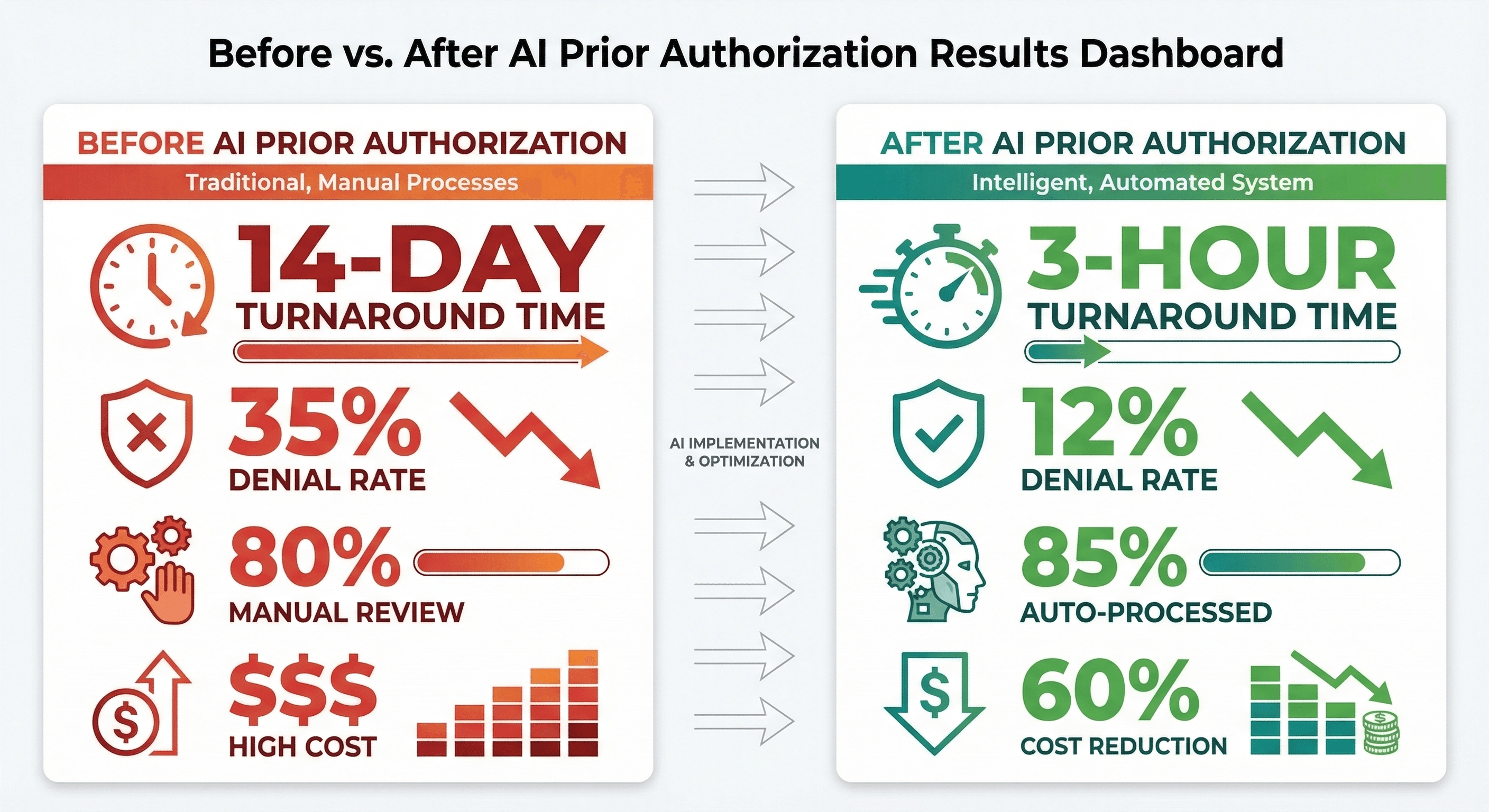
After 6 months in production, the results exceeded projections:
| Metric | Before | After | Improvement |
|---|---|---|---|
| Average turnaround time | 14 days | 2.8 hours | 99% faster |
| Initial denial rate | 35% | 12% | 66% reduction |
| Auto-processed rate | 0% | 85% | 85% automation |
| Manual review needed | 80% | 15% | 81% reduction |
| Annual PA team cost | $2.4M | $960K | 60% cost reduction |
| Physician time on PA | 20 min/patient | 3 min/patient | 85% time saved |
| Patient care delays | 38% of cases | 6% of cases | 84% reduction |
Financial Impact
- $1.44M annual savings in direct PA administrative costs
- $800K recovered revenue from reduced denials and faster approvals (treatments delivered sooner = revenue recognized sooner)
- $320K saved in appeal costs (fewer initial denials = fewer appeals to process)
- ROI: 340% within the first year, with the system paying for itself in under 4 months
Key Technical Learnings
Building this system taught us lessons that apply to any healthcare AI deployment:
- Domain-specific fine-tuning is non-negotiable: Generic LLMs misinterpret clinical abbreviations, miss critical negation patterns ("no evidence of metastasis" vs "evidence of metastasis"), and hallucinate medical codes. Our fine-tuned models achieved 97% accuracy on clinical data extraction vs 72% for general-purpose models.
- Payer rules are the hardest part: Clinical AI is well-studied; payer rule encoding is not. Rules are ambiguous, change frequently, and are often documented in 200-page PDF policy manuals. Invest heavily here.
- Shadow mode builds trust: Running AI alongside humans for 4 weeks before going live let the PA team see the system's accuracy firsthand. By the time we switched to production, the team was advocates, not resistors.
- The learning loop is the moat: Every denial, every appeal, every human override makes the system smarter. After 6 months, our denial prediction accuracy improved from 89% to 96%.
- Start with the highest-volume, most-standardized category: Radiology PAs were ideal for launch — high volume, relatively standardized criteria, and the PA team was most frustrated with them.
What This Means for Your Organization
Prior authorization automation is not science fiction — it is production-ready technology delivering measurable ROI today. If your organization processes more than 500 PA requests per month, the economics are compelling.
Nirmitee.io brings the full stack: healthcare domain expertise, HIPAA-compliant AI engineering, EHR integration experience, and production deployment methodology. We have done this before, and we can do it for you.
Ready to eliminate the prior authorization bottleneck? Schedule a consultation with our healthcare AI team.
