A 350-bed hospital system in the Midwest deployed an AI scheduling agent in Q3 2024. Within 90 days, no-show rates dropped from 18% to 11.5%, recapturing $420,000 in annual revenue that had been evaporating one missed appointment at a time. The CFO, who had been skeptical of the six-figure investment, signed off on two more agents before the first quarter ended.
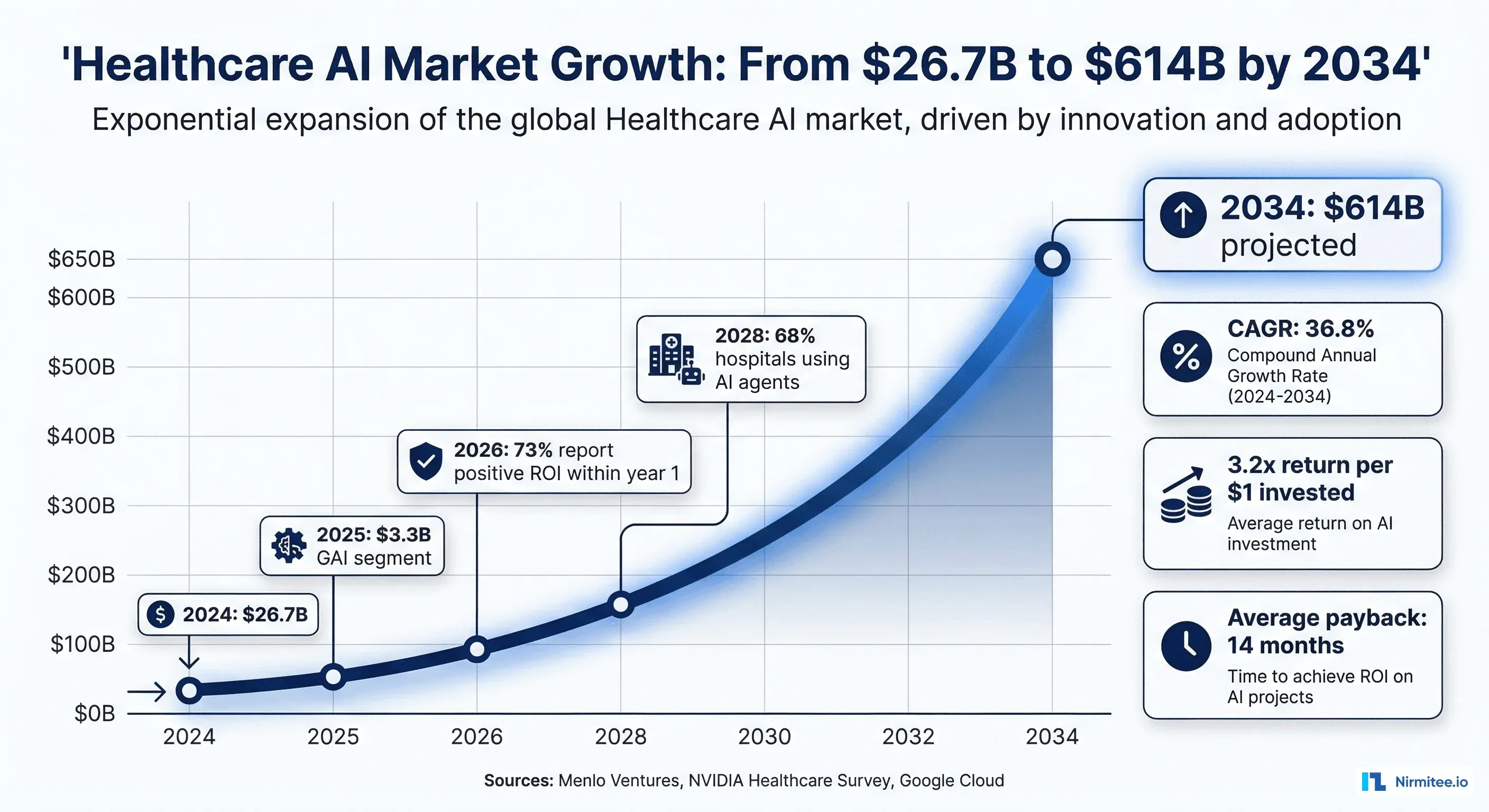
That story is becoming common. According to Google Cloud's 2025 ROI of AI in Healthcare report, 73% of healthcare leaders reported positive returns from AI investments within the first year. NVIDIA's 2026 healthcare AI survey found that 68% of healthcare organizations are already using AI agents, leading all other industries.
But here is where most health systems get stuck: they know AI works, but they do not know where to start. Which part of the patient journey gives the fastest payback? Which agents are low-risk enough to deploy first? Where is the $200 per-hour impact versus the $12 per-interaction impact?
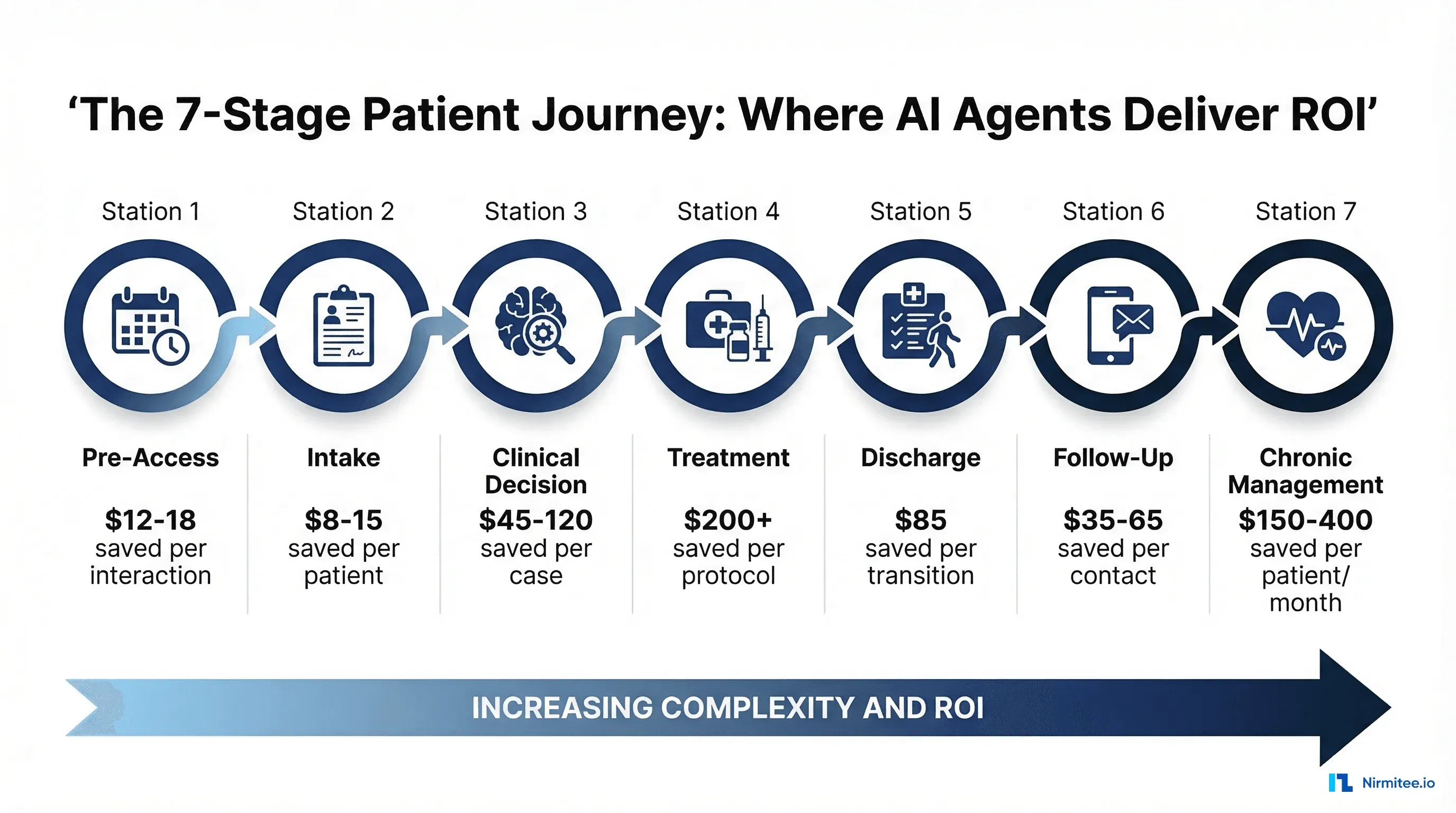
This guide maps the seven stages of the patient journey and quantifies where AI agents deliver measurable, dollar-denominated ROI at each stage.
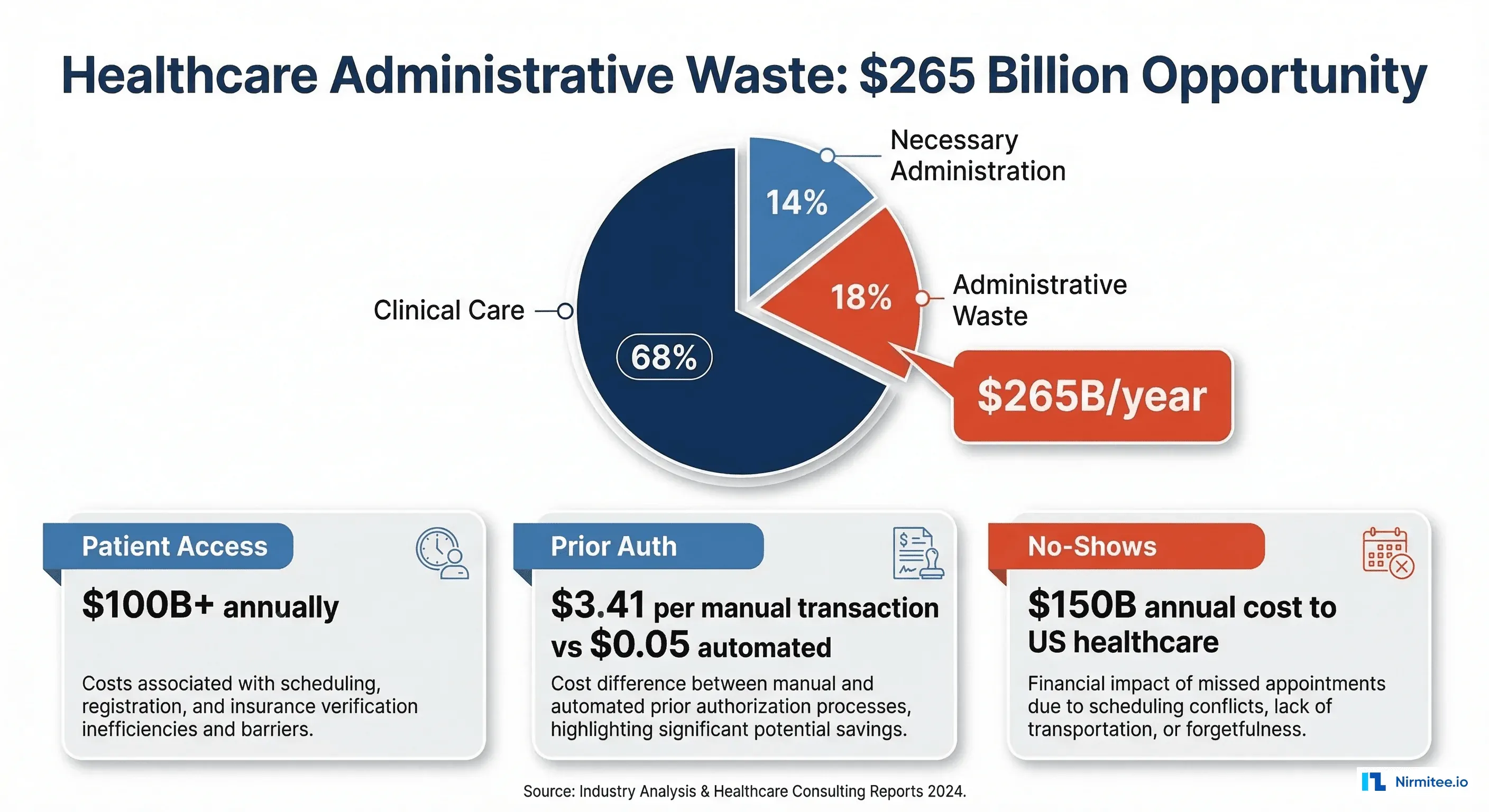
The $265 Billion Administrative Waste Opportunity
Before diving into specific stages, consider the scale of the opportunity. The U.S. healthcare system spends an estimated $265 billion annually on administrative waste: tasks that add cost without adding clinical value. Patient access alone accounts for more than $100 billion in annual administrative spending, according to Menlo Ventures' State of AI in Healthcare report.
AI agents do not replace clinicians. They replace the manual, repetitive administrative tasks that consume 15-30% of healthcare workers' time. The ROI comes from doing these tasks faster, more accurately, and 24 hours a day without overtime pay.
Stage 1: Pre-Access (Scheduling and Eligibility)
The problem: The average medical practice loses $150 billion annually across the U.S. healthcare system to patient no-shows. Each missed appointment costs an average of $200 in lost revenue. Meanwhile, scheduling staff spend 70% of their phone time on tasks an AI agent can handle: appointment booking, rescheduling, insurance verification, and waitlist management.
What the agent does: Handles inbound and outbound scheduling calls, verifies insurance eligibility in real time, manages cancellation waitlists, and sends intelligent reminders calibrated to each patient's no-show risk profile.
Measurable ROI:
- No-show reduction: 25-35% (industry average drops from 18% to 11-13%)
- Revenue recaptured per 200-bed facility: $380,000-$520,000 annually
- Staff time redirected: 2,000+ hours per year from phone scheduling to patient care
- After-hours coverage: 34% of appointments now booked outside business hours
- Payback period: 2-4 months
This is consistently the highest-ROI, lowest-risk AI agent deployment in healthcare. We break down the full scheduling agent business case separately.
Stage 2: Intake and Registration
The problem: Patient intake is a data entry bottleneck. Staff manually enter demographics, insurance information, medical history, and consent forms. The average intake process takes 12-18 minutes per patient, and automated data validation reduces follow-up calls by 60%.
What the agent does: Pre-populates registration forms from prior visits and insurance databases. Validates information in real time. Collects medical history via conversational interface (text or voice) before the patient arrives. Flags discrepancies for human review instead of requiring full manual entry.
Measurable ROI:
- Intake time reduction: 65-75% (from 15 minutes to 4-5 minutes average)
- Data accuracy improvement: 40% fewer registration errors
- Staff savings per 200-bed facility: $180,000-$260,000 annually (3-4 FTEs redirected)
- Patient satisfaction: 22% improvement in check-in experience scores
- Payback period: 4-6 months
Stage 3: Clinical Decision Support
The problem: Clinicians spend 49% of their time on EHR documentation and administrative tasks, according to AMA studies. Clinical decision support tools embedded in EHR workflows are either ignored (alert fatigue) or too generic to be useful. Meanwhile, diagnostic errors contribute to an estimated 371,000 deaths and 424,000 permanent disabilities annually in the U.S.
What the agent does: Surfaces relevant clinical context from the patient's complete record at the point of care. Identifies potential drug interactions, allergy conflicts, and care gaps. Generates differential diagnoses based on presenting symptoms and patient history. Produces clinical documentation from the encounter in real time.
Measurable ROI:
- Documentation time savings: 41% reduction, saving 66 minutes per provider per day
- Extrapolated across 100 providers: 40,000+ hours annually
- Diagnostic accuracy improvement: 12-18% for complex cases
- Revenue per provider increase: $45,000-$120,000 annually from increased patient throughput
- Annual savings for 200-bed facility: $450,000-$800,000
- Payback period: 8-12 months
Stage 4: Treatment (Prior Authorization)
The problem: Prior authorization is the single most expensive administrative process in healthcare. The CAQH Index reports that each manual prior authorization costs $3.41 per transaction. Multiply that across the millions of prior auth requests a large health system processes annually, and the labor cost is staggering. More critically, prior auth delays treatment: the average turnaround is 3-5 business days, during which patients wait for needed medications and procedures.
What the agent does: Reads clinical documentation, extracts relevant clinical criteria, cross-references payer-specific policies, assembles the prior auth submission, and submits electronically. Handles denials by identifying the specific deficiency and resubmitting with additional supporting documentation.
Measurable ROI:
- Cost per transaction: from $3.41 (manual) to $0.05 (automated), a 98.5% reduction
- Processing time: from 3-5 days to under 24 hours
- Denial rate reduction: 15-25% through better initial submission quality
- Staff time savings: 14 minutes per transaction
- Annual savings for 200-bed facility: $600,000-$1.2 million
- Payback period: 5-8 months

Stage 5: Discharge Planning
The problem: Poor discharge planning is the leading cause of preventable hospital readmissions, which cost the U.S. healthcare system $26 billion annually. CMS penalizes hospitals with above-average readmission rates through the Hospital Readmissions Reduction Program (HRRP), directly impacting revenue. A single 30-day readmission costs $15,000-$25,000.
What the agent does: Generates personalized discharge instructions based on the patient's conditions, medications, and social determinants. Coordinates follow-up appointments before discharge. Identifies high-risk patients for intensive post-discharge follow-up. Ensures medication reconciliation is complete and accurate.
Measurable ROI:
- Readmission rate reduction: 12-20% for targeted conditions
- Per-readmission cost avoided: $15,000-$25,000
- HRRP penalty avoidance: $200,000-$500,000 annually for penalized hospitals
- Discharge processing time reduction: 35-45%
- Annual savings for 200-bed facility: $320,000-$480,000
- Payback period: 6-9 months
Stage 6: Post-Discharge Follow-Up
The problem: Within 30 days of discharge, 20% of patients are readmitted and 50% have not seen their follow-up provider. The gap between discharge and the first follow-up visit is where patients fall through the cracks: they forget medications, miss warning signs, and end up back in the emergency department. Hospitals lack the staff to call every discharged patient, so only high-risk patients get proactive follow-up.
What the agent does: Conducts automated post-discharge check-ins via phone or text within 24-72 hours. Asks structured questions about symptoms, medication adherence, and warning signs. Escalates concerning responses to a care coordinator. Schedules follow-up appointments for patients who have not yet booked one.
Measurable ROI:
- Post-discharge contact rate: from 35% (manual) to 92% (automated)
- Early intervention: identifies 28% more patients needing immediate care
- Care coordinator efficiency: nurses focus on high-priority cases instead of routine calls
- Annual savings for 200-bed facility: $250,000-$400,000
- Payback period: 4-6 months
Stage 7: Chronic Disease Management
The problem: Six in ten American adults have at least one chronic disease. Chronic diseases account for 90% of the $4.5 trillion in annual U.S. healthcare spending. Between clinic visits (typically every 3-6 months), patients are largely on their own. Medication non-adherence alone costs the system $528 billion annually, according to the IQVIA Institute.
What the agent does: Monitors remote patient monitoring data from wearable devices and connected health tools. Detects trends before they become emergencies (rising blood pressure over 2 weeks, declining glucose control). Delivers personalized coaching messages. Coordinates care plan adjustments with the clinical team. Supports RPM/CCM/RTM billing by tracking qualifying patient interactions.
Measurable ROI:
- Emergency department visit reduction: 18-30% for monitored chronic conditions
- Hospitalization reduction: 15-25% for heart failure, COPD, diabetes patients
- RPM revenue generation: $150-$400 per patient per month in reimbursable codes
- Annual savings and revenue for 200-bed facility: $500,000-$900,000
- Payback period: 8-14 months

Total ROI: The Full Picture
When you add up the savings across all seven stages, a 200-bed hospital deploying AI agents across the complete patient journey can expect $2.7 million to $4.6 million in combined annual savings and new revenue. At the industry benchmark of 3.2x return per dollar invested, this represents a total AI investment of $840,000 to $1.4 million, an amount many health systems can fund from operational budgets without capital expenditure approval.
| Stage | Annual Savings (200-bed) | Payback Period | Risk Level |
|---|---|---|---|
| Pre-Access (Scheduling) | $380K-$520K | 2-4 months | Low |
| Intake (Registration) | $180K-$260K | 4-6 months | Low |
| Clinical Decision Support | $450K-$800K | 8-12 months | Medium-High |
| Treatment (Prior Auth) | $600K-$1.2M | 5-8 months | Medium |
| Discharge Planning | $320K-$480K | 6-9 months | Medium |
| Follow-Up | $250K-$400K | 4-6 months | Low |
| Chronic Management | $500K-$900K | 8-14 months | Medium |
| TOTAL | $2.7M-$4.6M |
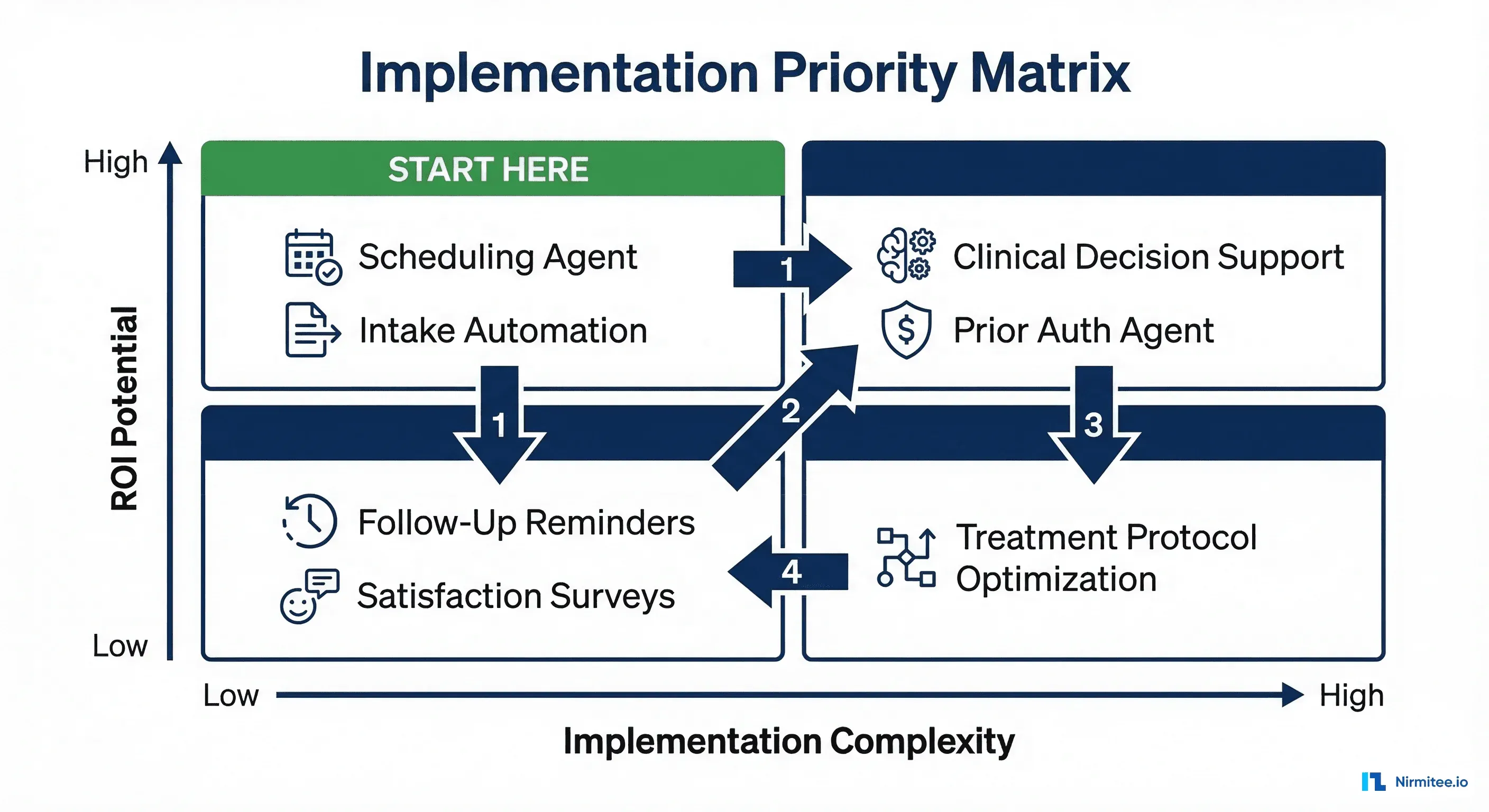
Where to Start: The Implementation Sequence
You do not deploy all seven agents at once. Based on the ROI timelines documented across healthcare organizations, the optimal deployment sequence follows the high-ROI, low-complexity path:
Quarter 1: Scheduling Agent (lowest risk, fastest payback, builds organizational confidence)
Quarter 2: Intake Automation + Follow-Up Agent (extends the access workflow, addresses readmission risk)
Quarter 3: Prior Authorization Agent (highest dollar savings, medium complexity)
Quarter 4+: Clinical Decision Support + Discharge + Chronic Management (higher complexity, higher clinical integration)
This sequence lets you demonstrate measurable ROI within 90 days (building executive confidence and budget support for subsequent agents), tackle the highest-dollar opportunities while organizational AI maturity is still growing, and defer clinical-grade agents until your team has experience operating AI in production.
The Window Is Closing
Health systems that deploy AI agents in 2026 will compound their operational advantages year over year. Those that wait will find themselves competing against organizations with 18-24 months of optimization data, trained models, and refined workflows. The procurement cycle for healthcare AI has already shortened from 8 months to 6.6 months, signaling that health system leadership is moving faster than at any point in digital health history.
The question is not whether AI agents will transform the patient journey. It is whether your organization will be deploying them or competing against those that already have.
Nirmitee helps health systems identify the highest-ROI agent opportunities and deploy them in production in 90 days or less. From scheduling agents to clinical decision support, our team builds the AI infrastructure that turns administrative waste into measurable savings.