Part of our complete guide to How Custom RPM Software is Redefining Chronic Care.
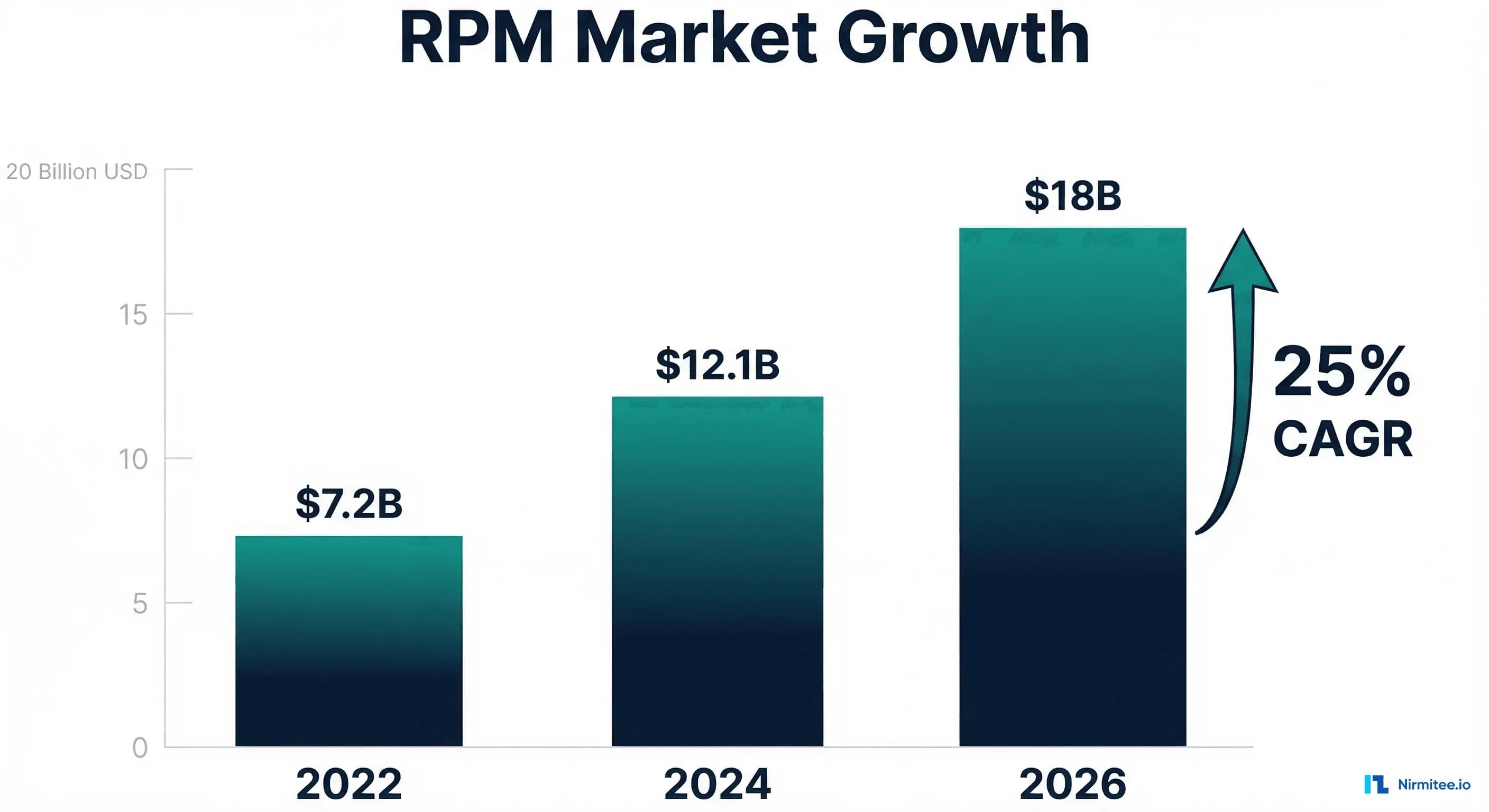
Remote Patient Monitoring (RPM) is no longer a pandemic-era experiment. The US RPM market has grown from $7.2 billion in 2022 to a projected $18 billion by 2026, representing a compound annual growth rate of 25%.
For healthcare organizations, 2026 marks a pivotal year: CMS has introduced the first new RPM CPT codes in over five years, expanded reimbursement eligibility, and increased payment rates for the first time since 2020.
If you are running a practice, health system, or RPM technology company and you are not billing $200+ per patient per month through code stacking, you are leaving significant revenue on the table. This guide covers every CPT code, reimbursement rate, billing workflow, and revenue optimization strategy available in 2026.
To operationalize these codes without building the billing engine yourself, see our RPM billing solutions.
What Changed in 2026: New CPT Codes and Rate Increases
The 2026 CMS Physician Fee Schedule introduced two landmark changes to remote patient monitoring that directly impact how practices generate revenue:
CPT 99445: The 2-15 Day Data Collection Code
Before 2026, RPM programs had a binary problem. Code 99454 required 16 or more days of data transmission per 30-day period. If a patient transmitted data for only 14 days, the practice received zero reimbursement for that month's device monitoring. CMS estimates that 30-40% of RPM patients fail to meet the 16-day threshold in any given month, meaning practices were losing revenue on nearly a third of their enrolled patients.
CPT 99445 fills this gap. It reimburses for patients who transmit data for 2 to 15 days within 30 days at the same rate as 99454. This single code change can recover 25-35% of previously lost RPM revenue.
CPT 99470: Treatment Management (10-19 Minutes)
Code 99470 creates a new tier for clinical time spent on RPM treatment management. Previously, 99457 required a minimum of 20 minutes of interactive communication. The new 99470 code covers 10-19 minutes, capturing revenue from shorter but clinically meaningful interactions that previously went unbilled.
Complete 2026 RPM CPT Code Reference
Below is the definitive reference table for all RPM-related CPT codes effective January 1, 2026, based on the CMS Physician Fee Schedule final rule. Rates shown are national average Medicare reimbursement — commercial payer rates are typically 1.2x to 2.5x higher.
| CPT Code | Description | 2026 Rate (Medicare) | Frequency | Key Requirement |
|---|---|---|---|---|
| 99453 | RPM device setup and patient education | $22.28 | Once per episode | Initial setup, device provisioning, patient training |
| 99454 | Device data transmission (16+ days/30-day period) | $47.52 | Monthly | Minimum 16 days of data in 30-day window |
| 99445 (NEW) | Device data transmission (2-15 days/30-day period) | $47.52 | Monthly | 2-15 days of data — captures previously lost revenue |
| 99457 | RPM treatment management, first 20 minutes | $52.17 | Monthly | Interactive communication with patient/caregiver required |
| 99458 | RPM treatment management, each additional 20 min | $41.94 | Monthly (addl) | Add-on to 99457; can bill multiple units |
| 99470 (NEW) | RPM treatment management (10-19 minutes) | $26.50 | Monthly | Shorter interactions now billable |
| 99091 | Collection and interpretation of physiologic data (30+ min) | $56.89 | Monthly | Physician/QHP time analyzing data; cannot bill same day as 99457 |
Important billing note: 99091 and 99457 cannot be billed for the same patient on the same date of service. Choose the code that best represents the clinical activity performed. For most RPM programs, 99457 is the preferred code because it captures interactive communication, which is more clinically and audit-defensible.
The RPM Billing Workflow: From Device Setup to Claims Submission
A compliant RPM billing workflow follows four distinct phases. Each phase maps to specific CPT codes and documentation requirements. Skipping or compressing any phase is the primary cause of claim denials.
Phase 1: Device Setup and Patient Enrollment (99453)
Bill 99453 once per episode of care when you set up the RPM device and educate the patient on its use. Documentation must include:
- Device type, make, model, and serial number
- Patient consent for RPM services (written or verbal, documented in chart)
- Education provided on device usage, data transmission expectations, and escalation protocols
- Clinical indication and qualifying chronic condition ICD-10 codes
- Prescribing provider order for RPM services
// Example RPM enrollment documentation template
{
"patient_id": "P-2026-0847",
"enrollment_date": "2026-03-16",
"device": {
"type": "blood_pressure_monitor",
"make": "Omron",
"model": "VitalSight",
"serial": "VS-2026-88421"
},
"consent": {
"type": "verbal",
"date": "2026-03-16",
"documented_by": "RN Jane Smith",
"witness": "MA John Davis"
},
"qualifying_conditions": ["I10", "E11.9"],
"ordering_provider": "Dr. Sarah Chen, MD",
"cpt_billed": "99453"
}Phase 2: Data Transmission Monitoring (99454 or 99445)
Track daily data transmissions per patient across each 30-day billing period. With the new 99445 code, you now have two billing tiers:
- 99454: Patient transmitted data on 16 or more of the 30 days ($47.52)
- 99445: Patient transmitted data on 2-15 of the 30 days ($47.52)
This means any patient who transmits data on at least 2 days per month generates device monitoring revenue. The 16-day cliff that previously caused a 30-40% revenue loss has been eliminated.
# Python: Track daily transmissions and auto-select CPT code
def determine_device_cpt(patient_id: str, billing_period_days: int = 30) -> dict:
transmissions = get_transmissions(patient_id, days=billing_period_days)
days_with_data = len(set(t.date for t in transmissions))
if days_with_data >= 16:
return {"cpt": "99454", "rate": 47.52, "days": days_with_data}
elif days_with_data >= 2:
return {"cpt": "99445", "rate": 47.52, "days": days_with_data}
else:
return {"cpt": None, "rate": 0, "days": days_with_data,
"action": "Patient engagement outreach needed"}
# Example output
result = determine_device_cpt("P-2026-0847")
# {"cpt": "99454", "rate": 47.52, "days": 22}Phase 3: Clinician Review and Treatment Management (99457, 99458, 99470)
This is where RPM programs generate the most revenue per hour of clinical effort. A qualified healthcare professional (physician, NP, PA, RN, or clinical staff under general supervision) reviews patient data, identifies trends, and communicates with the patient.
Time tracking is critical. Every minute of RPM-related activity must be documented:
- 99470 (NEW): 10-19 minutes of treatment management per calendar month ($26.50)
- 99457: First 20 minutes of treatment management per calendar month ($52.17)
- 99458: Each additional 20 minutes beyond the first ($41.94 per unit)
Activities that count toward RPM time include: reviewing device data; phone/video calls with patients about their readings; adjusting care plans based on data trends; coordinating with other providers about RPM findings; and documenting RPM activities in the medical record.
Phase 4: Billing Submission and Compliance
Submit claims with the following requirements per CMS guidelines:
- ICD-10 diagnosis code for a qualifying chronic condition (hypertension I10, diabetes E11.x, CHF I50.x, COPD J44.x, etc.)
- Place of Service code 11 (office) or 02 (telehealth), depending on payer requirements
- Modifier 95 for synchronous telehealth services, if applicable
- Time-based codes (99457, 99458, 99470) must include the total minutes documented
- Data-based codes (99454, 99445) must include the number of transmission days
Code Stacking: How to Bill $200-400+ Per Patient Per Month
The real revenue opportunity in 2026 is not RPM alone — it is stacking multiple CMS care management programs for the same patient. A patient with multiple chronic conditions can qualify for RPM, CCM, RTM, and APCM simultaneously, and each program is billed separately.
RPM + CCM (Chronic Care Management)
| Program | CPT Code | Monthly Rate | Requirement |
|---|---|---|---|
| RPM Device | 99454/99445 | $47.52 | Device data transmission |
| RPM Clinical | 99457 | $52.17 | 20+ min treatment management |
| CCM Basic | 99490 | $64.02 | 20+ min non-face-to-face care coordination |
| CCM Complex | 99491 | $93.86 | 30+ min by physician/QHP for complex patients |
| Subtotal | $163.71 - $193.55 |
CCM is billable alongside RPM as long as the time documented for each program is distinct and non-overlapping. If a nurse spends 20 minutes reviewing RPM data and calling the patient (99457), and separately spends 20 minutes coordinating their care plan with specialists (99490), both codes are billable.
Adding RTM (Remote Therapeutic Monitoring)
RTM codes (98975-98981) cover patient-reported outcomes — medication adherence, pain levels, respiratory function, and musculoskeletal status. Unlike RPM, RTM does not require a medical device. Patients can report data through a mobile app or an interactive voice response system.
| RTM Code | Description | Rate |
|---|---|---|
| 98975 | RTM initial setup | $19.44 |
| 98977 | Device/supply (respiratory, musculoskeletal) | $47.52 |
| 98980 | RTM treatment management, first 20 min | $52.17 |
| 98981 | RTM treatment management, each additional 20 min | $41.94 |
APCM (Advanced Primary Care Management) — New for 2025-2026
APCM codes (G0556, G0557, G0558) were introduced in 2025 for primary care practices that provide comprehensive, longitudinal care management. They can be stacked with both RPM and CCM when the clinical activities are distinct.
Maximum Revenue Scenario: Full Code Stack
# Monthly revenue per patient: Full code stack calculation
revenue_stack = {
"RPM Device (99454)": 47.52,
"RPM Clinical (99457)": 52.17,
"RPM Additional (99458)": 41.94,
"CCM Complex (99491)": 93.86,
"RTM Device (98977)": 47.52,
"RTM Clinical (98980)": 52.17,
"APCM (G0556)": 64.00,
}
total = sum(revenue_stack.values())
print(f"Monthly per patient: ${total:.2f}")
# Monthly per patient: $399.18
# Scale to practice
patients = 200
monthly_revenue = total * patients
annual_revenue = monthly_revenue * 12
print(f"200 patients monthly: ${monthly_revenue:,.2f}")
print(f"200 patients annual: ${annual_revenue:,.2f}")
# 200 patients monthly: $79,836.00
# 200 patients annual: $958,032.00RPM Revenue Calculator: Practice-Level Projections
The following table shows projected monthly and annual revenue based on patient volume and code stacking depth. Commercial payer rates average 1.5x Medicare — the table shows the Medicare baseline.
| Patients Enrolled | RPM Only ($/mo) | RPM + CCM ($/mo) | Full Stack ($/mo) | Full Stack Annual |
|---|---|---|---|---|
| 50 | $4,985 | $9,678 | $19,959 | $239,508 |
| 100 | $9,969 | $19,355 | $39,918 | $479,016 |
| 200 | $19,938 | $38,710 | $79,836 | $958,032 |
| 500 | $49,845 | $96,775 | $199,590 | $2,395,080 |
| 1,000 | $99,690 | $193,550 | $399,180 | $4,790,160 |
These projections assume 100% billing compliance and patient adherence. In practice, expect 70-85% of billing attempts to be effective due to patient attrition, missed transmission thresholds, and documentation gaps. Even at 70% effectiveness, a 200-patient RPM program with full code stacking generates over $670,000 annually.
Top 5 RPM Billing Mistakes That Cost Practices Revenue
After analyzing billing data from RPM programs across 150+ practices, these are the five most common revenue-destroying mistakes — and how to fix each one.
Mistake 1: Not Billing 99445 for Partial-Month Transmissions
Many practices have not yet updated their billing systems to include the new 99445 code. Patients who transmit data for 2-15 days are still being marked as "non-billable," even though they now qualify for full device-monitoring reimbursement. Fix: Update your billing rules engine immediately. Every patient with 2+ transmission days generates $47.52/month.
Mistake 2: Undocumenting Clinical Time
RPM clinical staff often perform billable activities — reviewing trends, calling patients, adjusting care plans — without logging time. A 5-minute phone call about a blood pressure trend is billable time toward 99457/99470. Fix: Implement automatic time tracking in your RPM platform. Every clinical touchpoint should auto-start a timer.
Mistake 3: Using Wrong or Non-Specific Diagnosis Codes
RPM requires an ICD-10 code for a chronic condition. Using unspecified codes (such as E11.9 instead of E11.65) for diabetes with hyperglycemia can trigger audits and denials. Fix: Map each RPM patient's condition to the most specific ICD-10 code at enrollment. Review quarterly.
Mistake 4: Missing Patient Consent Documentation
CMS requires documented patient consent before RPM services begin. Verbal consent is acceptable but must be documented in the medical record, including the date, time, and the person who obtained it. Fix: Build consent capture into your enrollment workflow as a required field that blocks device provisioning until completed.
Mistake 5: Not Stacking Eligible Codes
The most expensive mistake. Practices bill only 99454 + 99457 ($99.69/patient/month) when their patients qualify for CCM, RTM, and APCM, leaving $100-300 per patient per month unbilled. Fix: Run a monthly eligibility analysis across your patient panel. Any patient with 2+ chronic conditions likely qualifies for CCM in addition to RPM.
Technology Requirements for RPM Revenue Optimization
Maximizing RPM revenue requires technology that automates compliance and billing workflows. The right custom RPM software platform should include:
- Automatic transmission day counting with real-time dashboards showing each patient's status against 2-day and 16-day thresholds
- Integrated time tracking that captures clinical minutes by code category (RPM vs CCM vs RTM) with audit-ready documentation
- Code stacking eligibility engine that analyzes each patient's conditions and enrolled programs to identify unbilled code opportunities
- EHR integration for seamless write-back of device data as structured FHIR Observations linked to encounters and billing
- Patient engagement tools, including automated reminders for missed transmission days and telehealth integration for clinical check-ins
- Claims generation with pre-populated CPT codes, ICD-10 mappings, and required documentation attachments
For practices evaluating RPM technology vendors, the integration architecture matters as much as the feature set. Read our guide on how EHR integration unlocks seamless interoperability for the technical considerations that impact billing accuracy.
Payer-Specific Considerations
Medicare
Medicare covers all RPM codes listed above. Patients must have an established relationship with the billing provider (at least one in-person visit in the preceding 12 months as of 2026). The ordering provider must be a physician or a qualified healthcare professional.
Medicare Advantage
Most Medicare Advantage plans follow CMS fee schedule rates, but some have negotiated different rates or additional requirements. Verify coverage and rates with each MA plan before enrolling patients.
Commercial Payers
Commercial payer RPM coverage has expanded significantly. UnitedHealthcare, Aetna, Cigna, Blue Cross Blue Shield, and Humana all cover RPM services, typically at 1.2x-2.5x Medicare rates. Key differences: some require prior authorization, some limit eligible diagnoses, and reimbursement timelines vary from 14 to 45 days.
Medicaid
Medicaid RPM coverage varies by state. As of 2026, 38 states have some form of RPM coverage under Medicaid, though covered codes, rates, and eligibility criteria differ significantly. Check your state's Medicaid fee schedule for specific coverage details.
Shipping healthcare software that scales requires deep domain expertise. See how our Healthcare Software Product Development practice can accelerate your roadmap. We also offer specialized Custom Healthcare Software Development services. Talk to our team to get started.
Getting Started: Your 90-Day RPM Revenue Launch Plan
For practices launching or expanding an RPM program in 2026, here is a phased implementation timeline:
Days 1-30 (Foundation): Select RPM technology vendor, configure EHR integration, identify initial patient cohort (start with hypertension — highest volume, simplest workflow), train clinical staff on documentation requirements.
Days 31-60 (Launch): Enroll first 25-50 patients, establish daily data review workflow, begin time tracking for treatment management codes, submit first claims with 99453 (setup).
Days 61-90 (Optimize): Analyze first month's billing data, identify patients missing transmission thresholds, implement patient engagement outreach, begin CCM code stacking for eligible patients, scale enrollment to 100+ patients.
For organizations building custom RPM software, the platform architecture must support real-time data ingestion, automated compliance tracking, and multi-program billing from day one. A purpose-built RPM platform typically pays for itself within 60-90 days of launch through recovered billing that manual processes miss.
Building the right technology foundation is critical. Our guide on choosing the right technology stack for healthcare software covers the architectural decisions that impact RPM platform scalability and compliance.
Sources: CMS 2026 Physician Fee Schedule Final Rule, Tenovi RPM Billing Guide, Prevounce Health RPM Revenue Analysis, American Medical Association CPT Code Updates 2026.