ABDM integration for hospital software isn't one project — it's four milestones, each with its own certification gate. This guide covers all four: what NHA requires at M1, M2, M3, and M4, how they connect technically, and how to sequence the work so your team doesn't get stuck at any one milestone. This is a milestone roadmap guide, not a hands-on developer implementation walkthrough.
A typical mid-size hospital runs 4 to 8 separate software systems: HIS for patient management, LIMS for labs, RIS/PACS for radiology, pharmacy management, billing, and more. Each system owns a different slice of the patient's health record. Making all of them work together under ABDM is fundamentally different from integrating a single monolithic EHR.
This guide breaks down every ABDM milestone in detail, explains what happens at each stage, and addresses the real-world challenge of multi-software, multi-facility integration — the scenario every integrator and hospital IT team actually faces.
Who this guide is for:
- HMIS, LIMS, or RIS vendors building toward ABDM certification
- Hospital IT teams planning a multi-software integration project
- Health-tech startups adding ABDM compliance to an existing product
- Integrators and consultants managing sandbox-to-production deployments
Understanding the ABDM Milestone Framework
ABDM certification is structured into progressive milestones. Each builds on the previous one, adding new capabilities and responsibilities:
| Milestone | Your Role | Core Capability | Certification Focus |
|---|---|---|---|
| M1 | Identity Provider | ABHA creation, verification, patient discovery | Can your system identify patients digitally? |
| M2 | HIP (Health Information Provider) | Share health records on patient consent | Can you serve FHIR records when asked? |
| M3 | HIU (Health Information User) | Fetch and consume records from other providers | Can you request and display external records? |
| M4 | Claims Participant | NHCX — digital insurance claims exchange | Can you process claims digitally? |
Certification is per-software, not per-facility. You certify your software once through NHA's sandbox exit process, then each facility registers independently in the Health Facility Registry (HFR).
ABDM Implementation Timeline at a Glance
Before diving into each milestone, here's a realistic view of what each phase demands. These estimates assume an experienced integration team working on a mid-size hospital with 3–5 connected software systems:
| Milestone | Typical Dev Time | Key Dependency | Primary Risk |
|---|---|---|---|
| M1 | 3–6 weeks | HFR registration, ABHA API credentials, V3 sandbox access | Aadhaar-mobile mismatch in patient base; linking token persistence |
| M2 | 8–14 weeks | FHIR converter per system type, Fidelius encryption setup | FHIR schema non-compliance on first NHA review; consent artefact expiry handling |
| M3 | 4–6 weeks | Key management infra, HIU data viewer in HIS | Parser fragility on heterogeneous FHIR bundles from external HIPs |
| M4 | 6–12 weeks | NHCX empanelment, insurer-specific ClaimBundle mapping | Claim rejection due to missing clinical evidence FHIR links |
| Functional Testing + WASA | 6–10 weeks | CERT-IN / STQC empanelled agency engagement | First-submission failure (common) adds 2–4 weeks for remediation |
Total sandbox-to-production timeline for M1–M3: typically 6–9 months for a greenfield build; 4–6 months if you're layering onto an existing HMS with a structured integration layer.
ABDM V3 APIs — The Current Standard
Before diving into the milestones, a critical technical point: ABDM V3 APIs are the current standard. NHA's official ABDM Wrapper and all new integrations use V3 exclusively. The older v0.5 and v1.0 APIs are legacy — all new development must target V3.
V3 Gateway base URLs:
- Sandbox:
https://dev.abdm.gov.in/api/hiecm/gateway/v3/with headerX-CM-ID: sbx - Production: Same gateway path with header
X-CM-ID: abdm
Key V3 changes from legacy APIs:
- Discovery is synchronous: In V3, when ABDM sends a patient discovery request, your system returns the response directly in the HTTP body — no more async callback-based discovery
- Linking token at profile share: V3 provides a linking token at the time of scan-and-share (profile share). Your HRP must save this token and use it for HIP-initiated linking — eliminating the separate OTP-based linking flow
- Unified gateway endpoints: Authentication, bridge registration, and service management all live under the
/v3/path - Simplified bridge management:
PATCH /v3/bridge/urlfor registration,GET /v3/bridge-servicesto verify your configuration
V3 authentication:
curl -X POST 'https://dev.abdm.gov.in/api/hiecm/gateway/v3/sessions' \
-H 'Content-Type: application/json' \
-H 'X-CM-ID: sbx' \
-d '{
"clientId": "your-client-id",
"clientSecret": "your-client-secret",
"grantType": "client_credentials"
}'Every Client ID maps to one software instance and one callback URL. The gateway session token is passed in the Authorization header for all subsequent API calls.
Milestone 1 (M1) — ABHA and the Identity Layer
What Happens
M1 is the foundation. Your system must be able to create, verify, and link patient identities using ABHA (Ayushman Bharat Health Account) — the 14-digit unique health identifier for every Indian citizen.
The core flows in M1:
- ABHA Creation — Create a new ABHA number via Aadhaar OTP, mobile OTP, or demographic methods
- ABHA Verification — Verify an existing ABHA number presented by a patient at registration
- QR Scan & Share — Patient scans the facility's QR code, and their ABHA profile is auto-shared to your system via the V3 profile share API. In V3, this also provides a linking token that your system must save for subsequent HIP-initiated linking
- Care Context Linking — Link the patient's visit (consultation, admission, lab test) — called a "care context" — to their ABHA. In V3, use the linking token received during profile share for HIP-initiated linking, removing the need for separate OTP-based flows
- Health Facility Registry (HFR) — Register your facility with a valid HFR ID, which becomes your HIP ID in the ABDM network
Key V3 APIs for M1
- ABHA creation and verification APIs (Aadhaar OTP, mobile OTP flows)
- V3 Share Profile API — receives patient profile + linking token during QR scan
- V3 Link Token API — HIP-initiated linking using the saved linking token
- V3 Discovery (synchronous) — respond to patient discovery requests in the HTTP response body
M1 Challenges
- Aadhaar consent management: Many patients don't have Aadhaar-linked mobile numbers, forcing fallback to demographic-based creation which has strict matching rules
- Care context definition: What constitutes a "care context"? An OPD visit? A lab order? An admission episode? This decision must be consistent across your system
- Linking token lifecycle: The linking token provided during V3 profile share must be persisted reliably. If lost, HIP-initiated linking fails and you must fall back to user-initiated discovery — a worse user experience
- QR provisioning: The facility QR code must be correctly provisioned in HFR — misconfiguration breaks the entire scan-and-share flow
M1 in a Multi-Software Environment
Here's where it gets interesting. In a hospital running HIS + LIMS + RIS separately:
- Which system creates the ABHA? Typically the HIS (front desk registration). But the LIMS and RIS also need the ABHA number to link their care contexts
- ABHA and linking token propagation: When HIS receives the ABHA profile and linking token during scan-and-share, it must broadcast both to all downstream systems (LIMS, RIS, pharmacy). If they don't share a patient master, you need an integration layer that stores and distributes the linking token
- Care contexts from different systems: An OPD visit is a care context from HIS. A lab report is a care context from LIMS. A radiology study is a care context from RIS. All must be linked to the same ABHA. The ABDM gateway sees them all coming from one HIP ID — your middleware must aggregate them
Milestone 2 (M2) — HIP: Sharing Health Records
What Happens
M2 is where your system becomes a Health Information Provider (HIP). When a patient or another authorized system requests health records through ABDM, you must serve them — encrypted, in FHIR R4 format, on demand.
The complete M2 data flow:
- Patient grants consent via ABHA app or an HIU application
- ABDM sends consent notification to your HIP via your registered bridge URL
- You acknowledge the consent notification
- ABDM sends health information request with the consent artefact — this includes: consent ID, date range, the requester's encryption public key, a nonce, and a data push URL
- You validate the consent artefact (check expiry, scope, purpose)
- You fetch all matching care contexts from the specified date range
- You convert to FHIR R4 bundles conforming to NRCeS (National Resource Centre for EHR Standards) profiles
- You encrypt using Fidelius (Elliptic Curve Diffie-Hellman key exchange)
- You push encrypted data to the provided data push URL
FHIR Bundle Types You Must Produce
| Bundle Type | Source System | Content |
|---|---|---|
| OPConsultNote | HIS / EMR | Outpatient consultation notes, vitals, diagnosis |
| DischargeSummary | HIS / EMR | Inpatient discharge details, procedures, follow-up |
| DiagnosticReport | LIMS | Lab results — CBC, lipid panel, cultures, etc. |
| Prescription | EMR / Pharmacy | Medication orders, dosage, frequency |
| ImagingStudy | RIS / PACS | Radiology reports, imaging metadata |
| ImmunizationRecord | HIS | Vaccination history |
| WellnessRecord | Wellness apps | Vitals, activity, lifestyle data |
| HealthDocumentRecord | Any | Catch-all for scanned documents, PDFs |
M2 Challenges
- FHIR conversion is the hardest part: Your internal database schema (SQL tables with custom column names) must be mapped to HL7 FHIR R4 bundles conforming to NRCeS profiles. Every field, every coding system (SNOMED CT, LOINC, ICD-10) must be correct. This is not a weekend project
- Fidelius encryption: ABDM uses ECDH (Elliptic Curve Diffie-Hellman) for end-to-end encryption. You generate a key pair, encrypt the FHIR bundle using the requester's public key + your private key + nonces. Getting any parameter wrong means the transfer fails silently
- Bridge URL reachability: Your bridge URL is the single entry point that ABDM's gateway calls. It must be publicly accessible over HTTPS. Network issues, firewall rules, or DNS misconfigurations silently break the entire flow
- Consent expiry: Consents have TTLs. You must validate before serving data — serving data on an expired consent is a compliance violation
- One Client ID, one bridge URL: Each Client ID maps to exactly one callback URL. For multi-facility setups, all callbacks arrive at one URL — your middleware must route internally
M2 in a Multi-Software Environment — The Real Challenge
This is where most integrations either succeed or collapse. When ABDM sends a data request, you need to aggregate records from multiple independent systems:
For hospitals under AB-PMJAY, the stakes and timelines are laid out in our ABDM compliance guide for AB-PMJAY hospitals.
Problem 1: Each System Has Its Own Data Model
Your HIS stores consultations in one schema, your LIMS stores lab results in a completely different schema, and your RIS stores radiology in yet another format. Each needs its own FHIR converter:
// Middleware receives ABDM health information request
func handleDataRequest(consentArtefact ConsentArtefact) {
dateRange := consentArtefact.DateRange
patientABHA := consentArtefact.PatientABHA
// Query EACH system for its care contexts
opdNotes := hisClient.GetConsultations(patientABHA, dateRange)
labReports := limsClient.GetReports(patientABHA, dateRange)
radStudies := risClient.GetStudies(patientABHA, dateRange)
prescriptions := pharmacyClient.GetOrders(patientABHA, dateRange)
// Convert each to FHIR using system-specific converters
bundles := []FHIRBundle{}
bundles = append(bundles, convertHISToFHIR(opdNotes)...)
bundles = append(bundles, convertLIMSToFHIR(labReports)...)
bundles = append(bundles, convertRISToFHIR(radStudies)...)
bundles = append(bundles, convertPharmacyToFHIR(prescriptions)...)
// Encrypt all bundles and push
encrypted := fideliusEncrypt(bundles, consentArtefact.PublicKey)
pushToHIU(encrypted, consentArtefact.DataPushURL)
}Problem 2: Patient Identity Mapping Across Systems
Your HIS knows the patient as MRN-12345. Your LIMS knows them as LAB-67890. Your RIS knows them as RAD-11111. When ABDM sends a request with an ABHA number, your middleware must know which patient ID to query in each system.
Solution: Maintain a centralized patient master index that maps ABHA → HIS MRN → LIMS ID → RIS ID → Pharmacy ID. This is the single most critical data structure in your integration layer.
Problem 3: Care Context Registration
Every time a care context is created in ANY system (new OPD visit in HIS, new lab report in LIMS, new radiology study in RIS), it must be registered with ABDM against the patient's ABHA. Your middleware needs event listeners on every system:
- HIS creates a consultation → middleware registers care context with ABDM
- LIMS finalizes a lab report → middleware registers care context
- RIS completes a study → middleware registers care context
If any system fails to notify the middleware, that care context becomes invisible to ABDM — the patient's records are incomplete.
Problem 4: Discovery Across Systems
When ABDM sends a V3 discovery request, your middleware must synchronously query ALL systems, aggregate all care contexts for that patient, and return a unified response in the HTTP body. There is no async callback — you must respond within the request timeout:
{
"patient": { "referenceNumber": "ABHA-1234" },
"careContexts": [
{ "referenceNumber": "OPD-2024-001", "display": "OPD Visit - 15 Jan 2025" },
{ "referenceNumber": "LAB-2024-045", "display": "Blood Work - 15 Jan 2025" },
{ "referenceNumber": "RAD-2024-012", "display": "Chest X-Ray - 16 Jan 2025" },
{ "referenceNumber": "RX-2024-078", "display": "Prescription - 15 Jan 2025" }
]
}Each care context reference must be traceable back to the originating system so the middleware knows where to fetch the actual data during a health information request. The synchronous nature of V3 discovery makes this more demanding — you need all systems to respond fast or risk timeouts.
Milestone 3 (M3) — HIU: Consuming External Records
What Happens
In M3, your system flips roles. Instead of only serving records, you can now request and consume records from other HIPs in the ABDM network. A doctor in your hospital can pull a patient's records from their previous hospital.
The M3 flow:
- Doctor initiates consent request — your system creates a consent request via the ABDM gateway
- Patient approves in the ABHA app (this step is outside your control)
- ABDM notifies you with the consent artefact via your bridge URL callback
- You request health information from the gateway, providing your public key and nonce
- Remote HIP encrypts and pushes data via ABDM to your data transfer endpoint
- You decrypt using your private key + sender's public key (Fidelius decryption)
- You parse FHIR bundles and display to the doctor
M3 Challenges
- Key management: Each consent request needs a fresh key pair. Store private keys securely (HSM or Vault) until data arrives, then decrypt. Poor key management equals data breaches
- FHIR parsing from heterogeneous sources: Every HIP produces slightly different FHIR bundles. Some are perfectly structured, some barely conform. Your parser must be resilient to variation
- Consent UX: The patient must approve consent in the ABHA app. If they don't, you wait indefinitely. Build proper timeout handling, status polling, and user feedback into the doctor-facing UI
- Data normalization: Records from 10 hospitals use different coding systems and levels of detail. Presenting this coherently to a doctor is a significant UX challenge
M3 in a Multi-Software Environment
When external records arrive, which system should display them?
- Lab reports from another hospital — should they appear in your LIMS? Or in a unified patient view in the HIS?
- Radiology studies from outside — your RIS may not have a viewer for their FHIR format
- The practical answer: build a unified patient health record viewer in the HIS that aggregates both internal records (from your LIMS, RIS, pharmacy) and external records (from ABDM HIU fetch). Don't try to inject external records into each subsystem — it creates more problems than it solves
Milestone 4 (M4) — NHCX: Digital Claims Exchange
What Happens
M4 introduces the National Health Claims Exchange (NHCX) — a standardized, FHIR-based framework for digital insurance claims processing. This is the emerging frontier, gaining momentum as PMJAY (Pradhan Mantri Jan Arogya Yojana) and private insurers push toward digital-first claims. M4 is currently mandatory for PMJAY-empaneled hospitals and is expanding rapidly to state government schemes.
The four core NHCX flows:
- Coverage Eligibility: Before treatment begins, query NHCX to confirm the patient is covered, the scheme is active, and the procedure falls within covered benefits. Returns a CoverageEligibilityResponse FHIR resource
- Pre-Authorization: Submit a ClaimRequest bundle for planned procedures that require prior insurer approval — typically surgeries, high-cost diagnostics, and inpatient admissions. The insurer responds with a ClaimResponse containing approval, denial, or modification
- Claim Submission: After treatment, submit the claim with supporting clinical documents assembled as a FHIR ClaimBundle — diagnosis (ICD-10), procedures (CPT/ICD), prescriptions, lab evidence, and discharge summary
- Payment Notification: Receive payment status and Explanation of Benefits (EOB) via NHCX callback. EOBs include adjudication details — which line items were paid, denied, or partially approved
FHIR Resources Required for M4
| NHCX Flow | Primary FHIR Resource | Supporting Resources | Source System |
|---|---|---|---|
| Coverage Check | CoverageEligibilityRequest | Patient, Coverage | HIS (front desk) |
| Pre-Auth | Claim (pre-auth type) | Condition, Procedure, Practitioner | HIS + Surgical module |
| Claim Submission | Claim (claim type) | DiagnosticReport, MedicationRequest, Encounter | HIS + LIMS + Pharmacy |
| Payment | ClaimResponse, ExplanationOfBenefit | — | NHCX callback (inbound) |
M4 Challenges
- ICD-10 and procedure code discipline: Claims are adjudicated against diagnosis codes. If your HIS stores free-text diagnoses without mapped ICD-10 codes, M4 requires a retroactive data quality fix across your entire patient database
- Pre-auth turnaround: Pre-authorization responses from insurers can take hours to days. Your HIS must show pending pre-auth status clearly to clinical and billing staff, with retry logic for expired requests
- Insurer-specific variations: Different insurers implement NHCX with slightly different required fields and ClaimBundle structures. Your M4 layer needs per-insurer configuration, not a one-size-fits-all bundle
- Rejection handling: Claim denials arrive as ClaimResponse with reason codes. Your billing team needs a workflow to review, correct, and resubmit — this is an operational process change, not just a technical one
M4 in a Multi-Software / Multi-Facility Environment
- Each facility may be empaneled under different insurance schemes (PMJAY, state schemes, private insurers) — your M4 module must handle per-facility insurer routing
- Claims data spans systems: the diagnosis comes from HIS, lab evidence from LIMS, procedure details from the surgical module, medications from pharmacy — your middleware must assemble a complete ClaimBundle from all four
- For hospital groups, claim batching and reconciliation must work across facilities — a patient admitted at Branch A and transferred to Branch B for surgery generates a multi-facility claim
The Multi-Facility Dimension
Beyond multiple software systems, hospitals often have multiple physical locations. A hospital group with 3-10 branches faces additional challenges:
Architecture Decisions
| Decision | Option A | Option B | Recommendation |
|---|---|---|---|
| Database | Shared multi-tenant DB | Separate DB per facility | Shared with tenant isolation — simpler ops |
| Bridge URL | One for all facilities | One per facility | One bridge, route by HIP ID — single point of management |
| FHIR converter | Single converter | Per-facility converter | Single with facility-aware configuration |
| Key management | Shared key store | Per-facility keys | Centralized Vault with per-facility key paths |
| Patient dedup | Allow duplicates | Merge across facilities | Merge — critical for unified patient view |
Critical Multi-Facility Challenges
- Every facility needs its own HFR registration and HIP ID. Five branches means five HIP IDs. The QR code for scan-and-share is per-facility, not per-organization
- Single bridge URL receives ALL callbacks. Since each Client ID maps to one bridge URL, your router must parse the
hip.idfrom each ABDM request and route to the correct facility's handler. UseGET /v3/bridge-servicesto verify all facilities are correctly registered under your bridge - Patient deduplication across facilities. Same patient visits Facility A and B — your system must recognize it's the same person and merge care contexts. Without this, discovery returns incomplete results
- Consent artefacts can span facilities. A consent may request data from a date range covering visits at multiple of YOUR facilities. You must aggregate across facility databases
- Linking token per facility. In V3, the linking token from scan-and-share is specific to the facility where the patient scanned. If they visit another of your facilities, a new scan-and-share generates a new linking token for that facility's HIP ID
The Complete Picture: Multi-Software + Multi-Facility
The hardest real-world scenario — and the most common one — is a hospital group with multiple facilities, each running multiple software systems from different vendors. Here's what the integration architecture looks like:
ABDM V3 Gateway (NHA)
│
▼
┌──────────────────────────────────────┐
│ ABDM Integration Middleware │
│ (Single Bridge URL per Client ID) │
│ │
│ ┌───────────┐ ┌────────────────┐ │
│ │ HIP ID │ │ FHIR Converter │ │
│ │ Router │ │ Registry │ │
│ └─────┬─────┘ └───────┬────────┘ │
│ │ │ │
│ ┌─────▼────────────────▼──────┐ │
│ │ Patient Master Index │ │
│ │ ABHA → System IDs mapping │ │
│ │ + Linking Token Store │ │
│ └─────────────────────────────┘ │
└──────────┬───────────────────────────┘
│
┌──────┼──────────┐
▼ ▼ ▼
Facility A Facility B Facility C
(HIP: X) (HIP: Y) (HIP: Z)
┌────────┐ ┌────────┐ ┌────────┐
│HIS │ │HIS │ │HIS │
│LIMS │ │LIMS │ │LIMS │
│RIS/PACS│ │Pharmacy│ │RIS │
│Pharmacy│ │ │ │Billing │
└────────┘ └────────┘ └────────┘The middleware is the linchpin. It must:
- Route ABDM callbacks to the correct facility based on HIP ID
- Respond synchronously to V3 discovery requests by querying all systems within the target facility in parallel
- Store linking tokens per patient per facility, received during V3 profile share
- Aggregate care contexts from all systems within a facility
- Convert each system's data to FHIR using system-specific converters
- Merge patient identities across facilities and systems via the centralized patient master
- Handle Fidelius encryption, key pair management, and consent validation centrally
- Monitor every system's availability — if LIMS is down, serve what you can and flag partial data
What an Integrator Must Think About
If you are building ABDM middleware for hospitals (as a product or service), these are your critical considerations:
| Concern | Detail |
|---|---|
| Multi-tenancy | Each customer is a different organization with their own Client ID and HIP IDs. Your middleware must be fully tenant-isolated |
| Pluggable FHIR converters | Each customer's HIS/LIMS/RIS has a different schema. Your FHIR converter must be configurable per system type and per vendor, not hardcoded |
| Onboarding automation | Each new customer means new HFR registrations, V3 bridge URL configuration, Client ID provisioning, key setup, and system connector configuration |
| Synchronous discovery performance | V3 discovery is synchronous — you must query multiple backend systems and return aggregated results within the HTTP timeout. Invest in caching, parallel queries, and fallback strategies |
| Callback reliability | ABDM's consent and data flow callbacks need guaranteed delivery. Use message queues and retry logic — a dropped callback means a failed consent flow |
| Certification scope | You certify your software once, but each customer's deployment must pass a security assessment (STQC/CERT-IN empaneled agency) |
| Linking token persistence | V3 linking tokens must be reliably stored per patient per facility. Token loss means linking failure, which blocks care context creation |
| Monitoring and alerting | Build dashboards for: consent request success rate, FHIR bundle generation failures, encryption errors, discovery response times, linking token hit rate. When something breaks at 2 AM, you need to know which system at which facility failed |
The Sandbox to Production Journey
The certification path is structured but rigorous:
- Sandbox integration: Register with the V3 sandbox (
X-CM-ID: sbx), implement all APIs, test against the ABDM sandbox environment - Functional testing: NHA's internal team tests your flows against standardized patient journey scenarios
- Security assessment: A STQC/CERT-IN empaneled agency performs OWASP-10 web application security audit and issues a "Safe-to-Host" certificate
- Final approval: NHA grants production access — you switch
X-CM-IDfromsbxtoabdmand use production Client ID/Secret - HFR registration: Register each physical facility in the production HFR, verify with
GET /v3/bridge-services
Key insight: Certification is per-software. But deployment — HFR registration, bridge URL setup, patient data seeding — is per-facility. For a multi-facility group, step 5 is repeated for every branch.
Common Mistakes That Stall ABDM Integration
Most ABDM integration projects don't fail because of technical inability — they stall because of avoidable errors that surface late in the sandbox testing cycle. Here are the patterns we see repeatedly:
1. Losing the V3 Linking Token
The linking token received during scan-and-share (V3 profile share) must be persisted immediately and reliably. If it's stored only in memory or discarded after the session, HIP-initiated linking fails silently. You won't know until NHA's testing team runs the M1 test cases and they fail. Solution: write the token to your patient master index at the moment of receipt, before any other processing.
2. Defining Care Contexts Inconsistently
A care context is the unit of linkable health data — but your HIS, LIMS, and RIS teams will define it differently unless you force alignment early. If HIS treats a care context as an admission episode and LIMS treats it as a single lab result, your middleware produces duplicate linking calls and confusing discovery responses. Define the care context schema once, enforce it across all systems before integration begins.
3. FHIR Bundles That Don't Conform to NRCeS Profiles
The ABDM gateway validates FHIR R4 bundles against NRCeS (National Resource Centre for EHR Standards) profiles — India-specific profiles layered on top of HL7 FHIR R4. Generic FHIR libraries produce standard R4 bundles, not NRCeS-compliant ones. The most common failures: missing required Indian extensions, incorrect SNOMED-CT codes for Indian procedures, and OPConsultNote bundles that omit the mandatory chief complaint Observation. Validate against NRCeS profiles in your test pipeline before submitting to NHA.
4. Bridge URL Misconfiguration
Your ABDM bridge URL is the single point through which the gateway sends all consent notifications, discovery requests, and health information requests. Two common failures: the URL is not publicly accessible from NHA's servers (firewall or VPN issue), and the URL is registered correctly in sandbox but the production registration is done with a different path. Both cause silent failures — the gateway calls you, gets no response, and the flow stalls with no useful error on your side. Always verify with GET /v3/bridge-services after every registration change.
5. Treating ABDM as a Weekend API Task
ABDM touches patient registration, facility identity, consent management, clinical records, FHIR conversion, encryption, and data sharing. It is not a single API integration — it is a cross-functional project touching your front desk, IT, clinical, and billing teams. Teams that scope it as a small technical task miss the operational changes (staff training, consent explanation workflows, care context creation at every patient touchpoint) and then scramble before the NHA testing deadline.
6. Skipping the Patient Master Index Design
In a multi-software environment, the centralized patient master index — mapping ABHA numbers to system-specific patient IDs across HIS, LIMS, RIS, and pharmacy — is the most critical data structure in the entire integration. Teams that treat it as an afterthought (mapping ABHA only in HIS, expecting other systems to "just work") hit a hard wall at M2, when the middleware must query all systems in parallel and aggregate care contexts for a single ABHA.
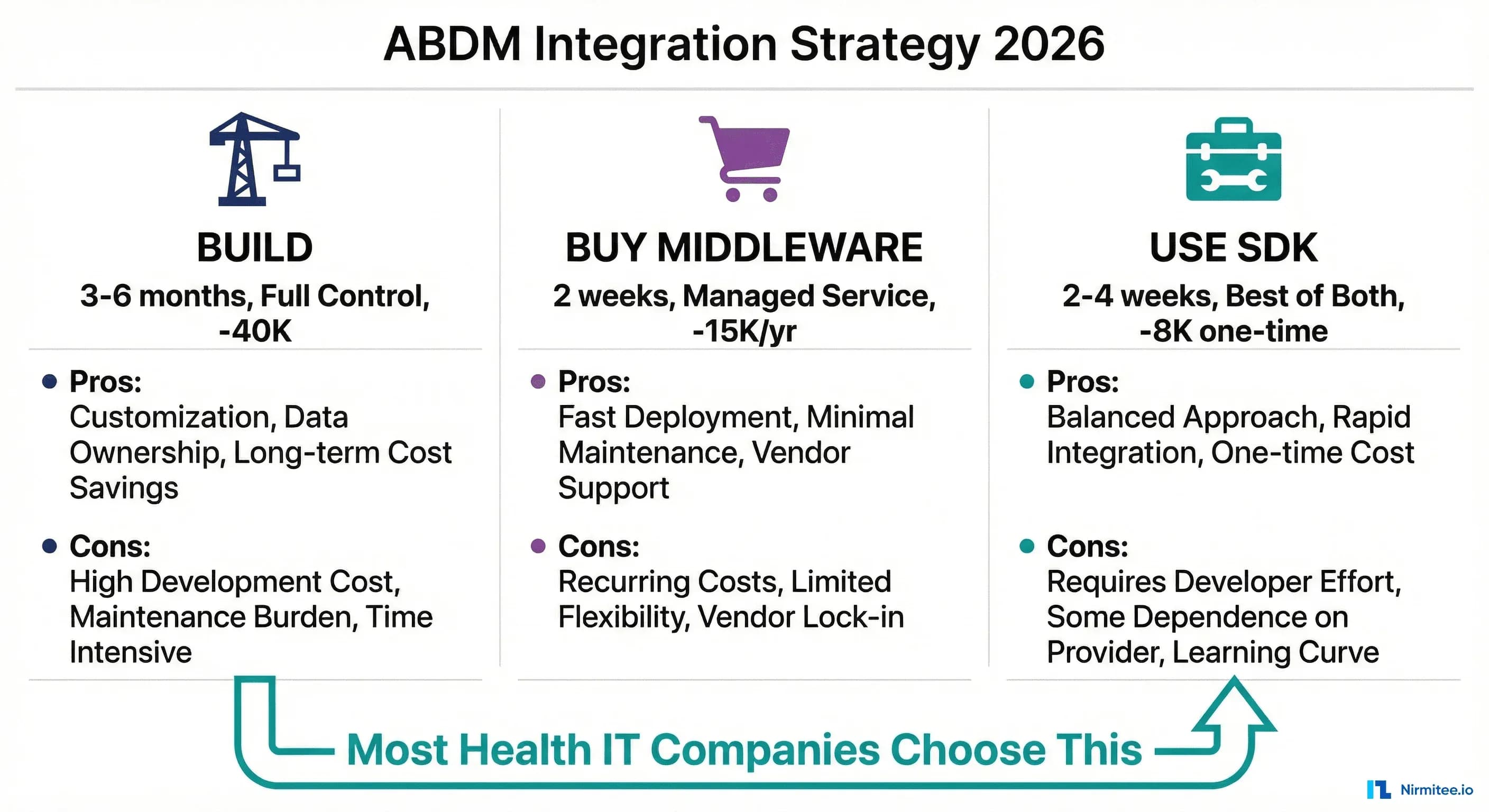
Build vs. Buy vs. Hire an Integrator
Hospital IT teams and HMS vendors ask this question early. Here's a clear-eyed view of the three options:
| Approach | Best For | Effort | Key Risk |
|---|---|---|---|
| Build in-house | Large HMS vendors with dedicated engineering teams and existing FHIR infrastructure | High — 6–12 months for M1–M3 from scratch | FHIR expertise gap; NRCeS profile compliance failures on first submission |
| HMS with built-in ABDM | Hospitals switching to a new HMS that's already ABDM-certified | Low — follow the HMS vendor's onboarding | Locked into one HMS vendor; multi-software environments not covered |
| Third-party integrator | Hospitals with existing multi-vendor software that can't switch HMS; HMS vendors needing faster certification | Medium — your team owns configuration and HFR setup; integrator owns the middleware | Integration quality varies widely; insist on production-certified references |
The third option — a specialist integrator with a pre-built middleware layer — typically cuts the M1–M3 timeline significantly for hospitals already running 3+ software systems, because the FHIR converter library, Fidelius encryption module, and patient master architecture are built once and configured per customer rather than rebuilt from scratch.
How Nirmitee Approaches ABDM Integration
At Nirmitee, we have built production ABDM integration across all milestones using V3 APIs. Our approach addresses the multi-software reality head-on:
- Middleware-first architecture: A single integration layer that sits between the ABDM V3 gateway and any combination of hospital software systems. Connect your HIS, LIMS, RIS, pharmacy — whatever you run
- Pluggable FHIR converters: System-specific adapters that map your existing data to NRCeS-compliant FHIR R4 bundles without requiring changes to your source systems
- Centralized patient master with linking token store: ABHA-to-system-ID mapping across all connected systems and facilities, with reliable V3 linking token persistence
- Multi-facility routing: Single bridge URL with intelligent routing by HIP ID, handling synchronous discovery aggregation and consent spanning across facilities
- Performance-optimized discovery: Parallel querying of backend systems to meet V3's synchronous discovery requirements within timeout constraints
Whether you're a hospital group looking to achieve ABDM compliance across branches, or a health-tech company building ABDM-certified software, the multi-software integration challenge is the one that matters most. Talk to our team about getting it right the first time.
Building interoperable healthcare systems is complex. Our Healthcare Interoperability Solutions team has deep experience shipping production integrations. We also offer specialized Custom Healthcare Software Development services. Talk to our team to get started.
Need a hands-on developer walkthrough from sandbox to production? See: ABDM Integration Step-by-Step: Developer Walkthrough from Sandbox Registration to Production Go-Live
Explore ABDM and India digital health
Milestones and certification
- ABDM Integration Step-by-Step
- ABDM Certification Process Explained
- Building an ABDM HIP from Scratch
- Building an ABDM HIU from Scratch
- Why ABDM M2 Certification Breaks Most Development Teams
FHIR bundles and health records
- Why Your ABDM FHIR Bundles Show NA in PHR
- Understanding ABDM FHIR Bundles, A Complete Guide from Zero to Expert
- ABDM FHIR Bundles in Action — A Complete Patient Journey from Hospital...
Troubleshooting and debugging
Strategy, compliance and migration
- ABDM Compliance for AB-PMJAY Hospitals
- Implementing ABDM Fidelius Encryption in Node.js: The Complete Guide
- ABDM V3 API Migration Guide
- Build vs Buy vs SDK: Choosing Your ABDM Integration Strategy in 2026