Your healthtech product works. You've proven it at one hospital, maybe two. The integration was painful — custom HL7 interfaces, weeks of testing, late-night calls with the hospital's interface analyst. But it works. Now sales has 15 more hospitals in the pipeline, and the CEO wants to know: "How fast can we onboard them?"
The answer depends entirely on whether you built your integration for one hospital or for a hundred. This guide covers the engineering strategy for scaling from MVP to enterprise-grade EHR connectivity.

The MVP Integration Trap
At the MVP stage, your integration probably looks like this: a single connection to a single EHR instance, custom-built for that hospital's specific configuration. Maybe it's an HL7v2 ADT feed, maybe it's a direct FHIR connection to their Epic instance. It works, but it's brittle, manual, and non-transferable.
The trap is assuming that onboarding hospital #2 will take the same effort as hospital #1. It won't — it might take more, because:
- Hospital #2 runs a different EHR (Cerner instead of Epic)
- Same EHR vendor but different version, different modules enabled, different custom fields
- Different network topology (VPN requirements, firewall rules, IP whitelisting)
- Different IT team with different processes, timelines, and risk tolerance
- Different data quality — missing fields you assumed would always be present
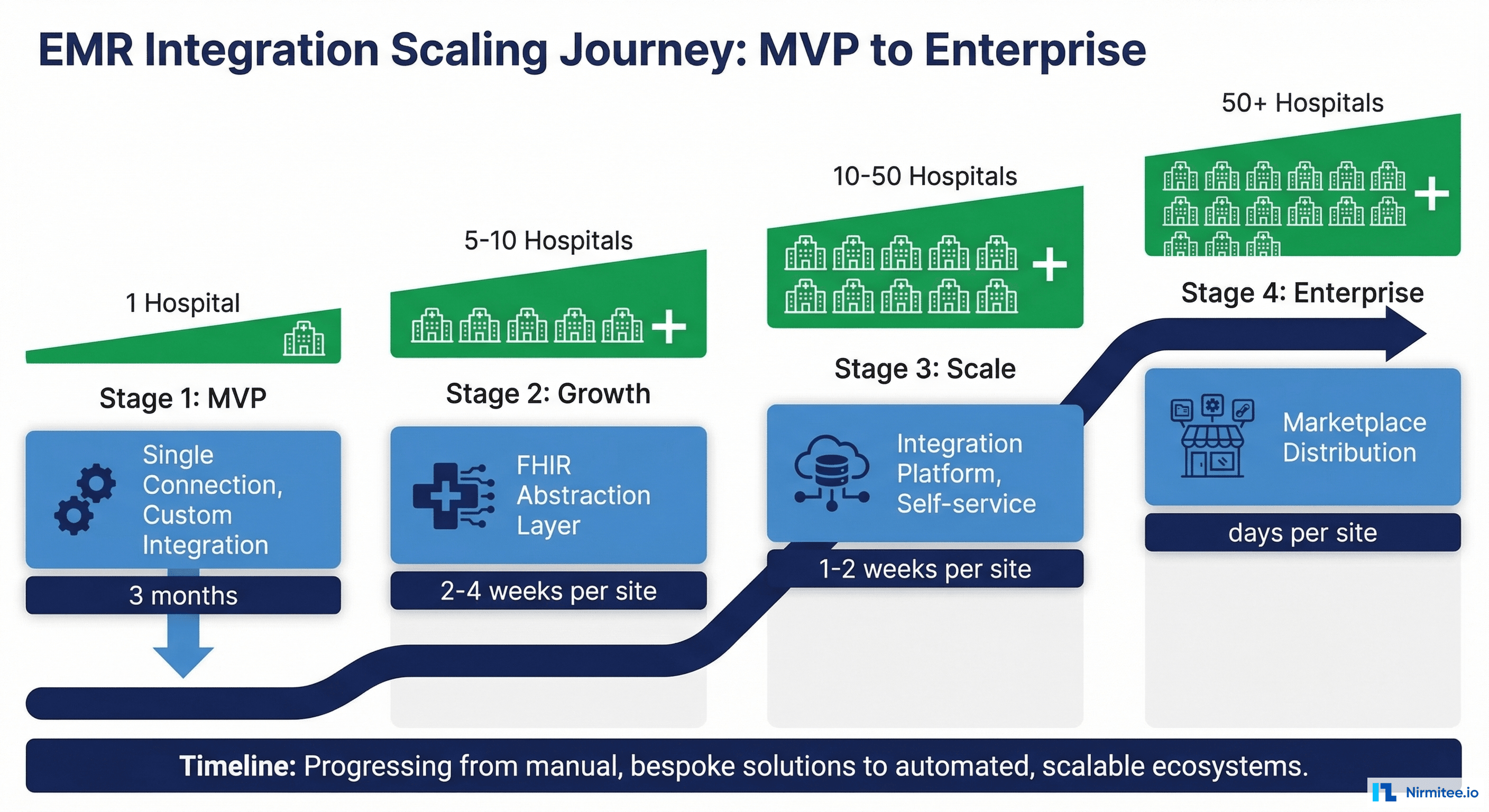
The Four Stages of Integration Maturity
Stage 1: Custom (1-2 hospitals, 2-6 months per site)
Every connection is hand-built. The integration engineer knows each hospital's quirks by heart. Onboarding requires code changes, custom deployment, and manual testing. This is fine for proving product-market fit, but it doesn't scale.
Stage 2: Standardized (5-10 hospitals, 2-4 weeks per site)
You've built a FHIR abstraction layer that normalizes the differences between EHR implementations. New hospitals are configured, not coded. You have adapters for Epic, Cerner, and maybe MEDITECH. Onboarding is still engineer-led but follows a repeatable playbook.
Stage 3: Platform (10-50 hospitals, 1-2 weeks per site)
Self-service onboarding tools let your customer success team configure new connections without engineering involvement. Automated testing validates data flow before go-live. You have monitoring dashboards, SLA tracking, and incident management.
Stage 4: Marketplace (50+ hospitals, days per site)
Your app is certified on Epic App Market, Oracle Health app gallery, and other EHR marketplaces. Hospitals install your app like an iPhone app — click, authorize, done. Integration is a feature of the EHR ecosystem, not a separate project.
Building the FHIR Abstraction Layer
The key architectural investment for Stage 2 is a FHIR abstraction layer that sits between your application and the EHR ecosystem. Even though FHIR is a standard, every EHR implements it differently:

class FHIRAbstractionLayer:
"""Normalizes FHIR implementation differences across EHR vendors."""
def __init__(self):
self.adapters = {
"epic": EpicAdapter(),
"cerner": CernerAdapter(),
"meditech": MEDITECHAdapter(),
"athena": AthenaAdapter(),
}
def get_patient(self, tenant_config: dict, patient_id: str) -> dict:
"""Get patient data, normalized across EHR differences."""
adapter = self.adapters[tenant_config["ehr_vendor"]]
raw = adapter.fetch_patient(tenant_config, patient_id)
return self.normalize_patient(raw, tenant_config)
def normalize_patient(self, raw_patient: dict, config: dict) -> dict:
"""Handle vendor-specific extensions and field mapping."""
normalized = {
"id": raw_patient["id"],
"mrn": self._extract_mrn(raw_patient, config),
"name": self._extract_name(raw_patient),
"dob": raw_patient.get("birthDate"),
"gender": raw_patient.get("gender"),
}
# Epic stores MRN in a specific identifier system
# Cerner uses a different system URI
# The adapter handles this transparently
return normalized
def _extract_mrn(self, patient: dict, config: dict) -> str:
"""Extract MRN from vendor-specific identifier systems."""
mrn_system = config.get("mrn_system_uri")
for identifier in patient.get("identifier", []):
if identifier.get("system") == mrn_system:
return identifier["value"]
return NoneThe EHR Market Reality
You don't need to integrate with every EHR. Focus on market share:
- Epic: ~38-40% of US acute care hospitals. Non-negotiable — almost every health system RFP requires Epic integration.
- Oracle Health (Cerner): ~25%. Second priority. Covers the VA, DOD, and many mid-size health systems.
- MEDITECH: ~16%. Critical for community hospitals, which are often your easiest sales.
- athenahealth: ~8%. Strong in ambulatory/outpatient settings.
Epic + Oracle Health + MEDITECH = ~80% market coverage. Add athena and you're at ~88%. That's your integration roadmap priority.
Self-Service Onboarding Pipeline
At Stage 3, your onboarding should be a structured pipeline, not ad-hoc engineering:
- Configure EHR adapter: Select vendor, enter FHIR endpoint URL, configure auth credentials
- Test connection: Automated health check — can we authenticate? Can we read a Patient resource?
- Map custom fields: Hospital-specific identifier systems, custom extensions, local code mappings
- Validate data: Pull sample data for 10 patients, verify all expected fields are populated
- Load test: Simulate production query volume, verify response times under load
- Go live: Enable production traffic with monitoring and alerting active
Build vs Buy: Integration Platforms
You don't have to build everything yourself. Integration platforms can accelerate your timeline:
- Redox: Most widely used healthtech integration platform. Pre-built connections to 500+ health systems. Best for startups that need to ship fast.
- Health Gorilla: Strong in clinical data aggregation. Good for apps that need comprehensive patient records across providers.
- Particle Health: Claims and clinical data from national networks. Good for population health and analytics use cases.
- Direct FHIR: Build your own connections for maximum control, lowest per-transaction cost, and deepest EHR functionality. Best when you've validated your integration patterns and need to optimize cost at scale.
Our recommendation: Start with a platform (Redox) for your first 10 hospitals to validate your integration patterns and get to market fast. Then build direct FHIR connections for your top 2-3 EHR targets to reduce costs and unlock deeper functionality.
Working with Hospital IT Teams
The technical integration is half the battle. The other half is navigating hospital IT processes:
- Security reviews: Every hospital has its own HIPAA security questionnaire. Build a master response document and keep it current. Budget 2-4 weeks for the review process.
- Change management: Hospital IT teams have change windows (often Tuesday and Thursday evenings). Plan your go-lives accordingly.
- Interface analysts: These are your best friends. They know where every HL7 message goes and every FHIR endpoint is configured. Build relationships early.
- Downtime coordination: EHR systems have scheduled maintenance windows. Your integration must handle downtime gracefully — queue messages, retry with backoff, and alert on extended outages.
For a complete framework on the build vs buy decision, see our EHR integration decision guide. For a case study on building a unified FHIR facade across multiple EHRs, read about our multi-EHR FHIR facade.
At Nirmitee, we help healthtech companies scale from MVP integrations to enterprise-grade EHR connectivity. Whether you need a FHIR abstraction layer, multi-tenant architecture, or self-service onboarding tooling, let's talk.