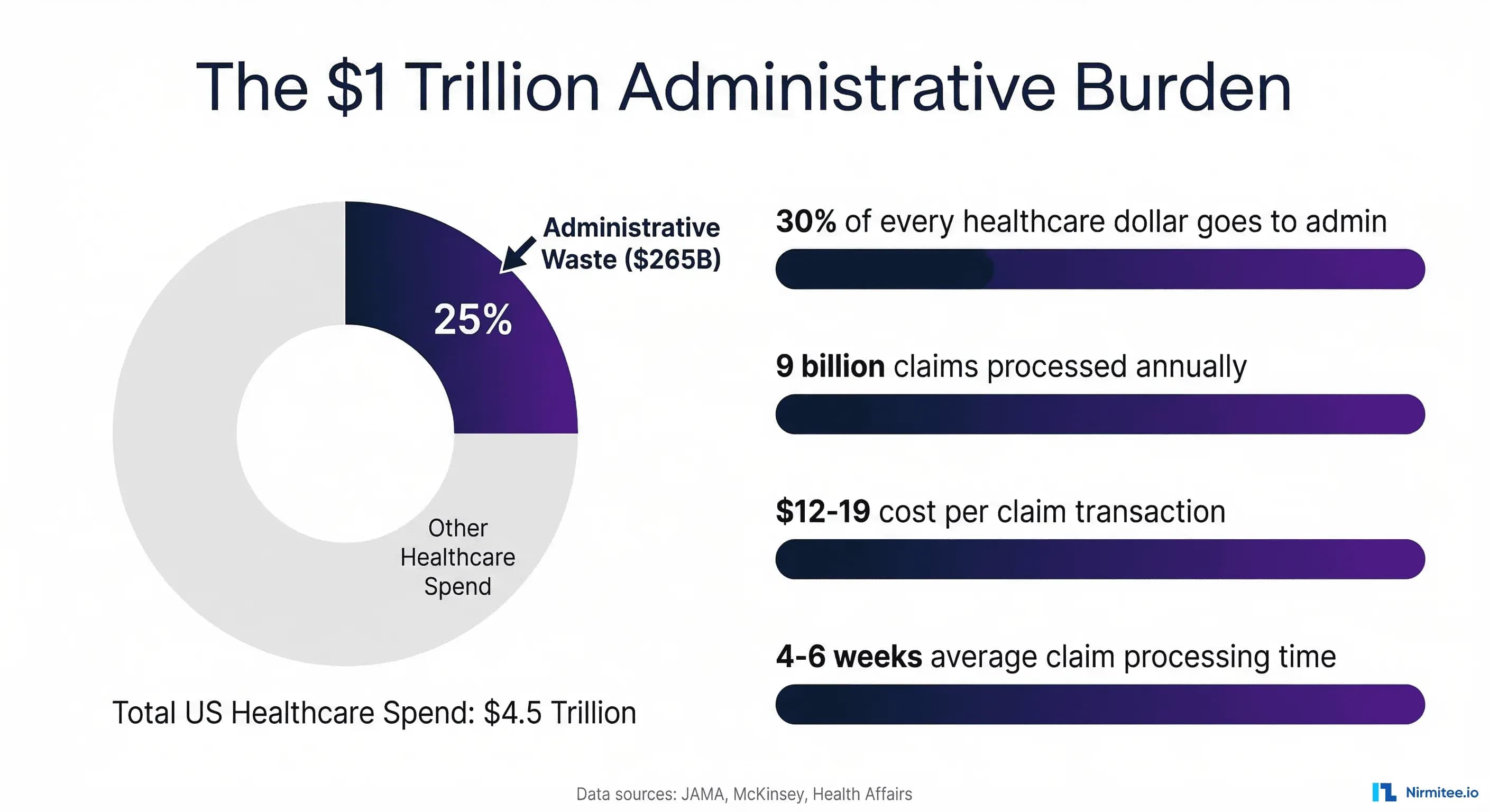
Healthcare organizations in the United States spend more on administration than any other country in the world. According to a landmark JAMA study, wasteful spending in US healthcare ranges from $760 billion to $935 billion annually, with administrative complexity representing the single largest category at $265.6 billion per year.
McKinsey estimates that targeted interventions could eliminate up to $265 billion in administrative waste, roughly 7% of the $4.5 trillion in total healthcare expenditure. For every dollar spent on patient care, approximately 30 cents goes to administrative overhead. This is not a technology problem. It is an operational architecture problem, and workflow automation is the operational architecture solution.
This guide provides a comprehensive, implementation-ready blueprint for eliminating manual processes across the healthcare revenue cycle and clinical operations. Unlike surface-level overviews that list automation benefits without specifics, we cover every automatable workflow with the architecture, tools, integration requirements, and ROI data you need to build a business case and execute.
Whether you are a CIO evaluating your first automation investment or a revenue cycle director scaling an existing program, this is the definitive resource for healthcare workflow automation in 2026.
The Manual Process Burden: Why Healthcare Is Drowning in Admin
The US healthcare system processes approximately 9 billion claims per year, with each claim costing $12 to $19 in transaction costs across private payers and providers. Each claim takes an average of 4 to 6 weeks to process and pay.
But claims are only one piece of the administrative puzzle. Behind every claim sits a cascade of manual workflows: scheduling, registration, eligibility verification, prior authorization, documentation, coding, charge capture, submission, follow-up, denial management, appeals, and patient billing.
The Health Affairs analysis of administrative waste found that the United States spends $1,055 per capita on healthcare administration, more than three times Germany's $306 per capita, the second-highest spender. Woolhandler and Himmelstein estimate that total US healthcare administration costs $1.1 trillion annually, with $504 billion classified as excess waste that delivers no patient value.
The operational consequences are equally severe. A 2024 AMA survey of 1,000 practicing physicians found that 93% report care delays due to prior authorization requirements, and 82% of patients sometimes abandon recommended treatment because of authorization barriers.
Staff burnout is endemic: 57% of physicians report that automation of documentation, prior authorizations, and other non-patient-facing tasks could significantly reduce their stress. Meanwhile, initial claim denial rates have climbed to 11.65% to 17% of submitted claims, nearly doubling over the past decade, with the average cost to rework a denied claim reaching $25 to $181.
The question for healthcare leaders in 2026 is not whether to automate. It is about which workflows to automate first, which technology to use, and how to sequence the transformation to maximize ROI with minimal disruption.
The Healthcare Automation Maturity Model: Five Levels
Before selecting specific workflows to automate, healthcare organizations need an honest assessment of their current automation maturity. Based on industry maturity frameworks and our implementation experience across health systems, we define five distinct maturity levels. Most US healthcare organizations in 2026 operate at Level 1 or Level 2. The goal is not to leap to Level 5 overnight but to advance deliberately, building organizational capability at each stage before progressing.
Level 1: Basic Rules (Where Most Start)
At this level, automation consists of simple if-then triggers: appointment reminder emails sent 24 hours before a visit, alert notifications for missing insurance information, auto-routing of referral faxes to specific queues.
These are typically built into the EHR or practice management system. They reduce some manual tasks but do not fundamentally change the workflow. Manual intervention remains the primary operational mode, and processes are often poorly documented.
For clinics and practices, much of this automation ships pre-packaged in our practice management solutions.
Typical capabilities: EHR-based scheduling alerts, template-driven appointment reminders, basic eligibility check triggers, and rule-based claim scrubbing for obvious errors.
Limitation: Each rule handles exactly one scenario. When exceptions occur (which they do 20-40% of the time in healthcare), the workflow falls back entirely to manual processing.
Level 2: RPA (Robotic Process Automation)
RPA introduces software bots that mimic human interactions with digital systems. A bot can log into a payer portal, check claim status, copy the result to a spreadsheet, and repeat for hundreds of claims. This is screen-scraping automation: the bot follows a deterministic script, clicking buttons and filling fields exactly as a human would, but faster and without fatigue.
Typical capabilities: Batch eligibility verification via EDI 270/271 transactions, automated payment posting from ERA/EOB files, claim status checking across payer portals, demographic data transfer between registration and billing systems.
Limitation: Industry research indicates that RPA maintenance accounts for 70-75% of total automation budgets. When a payer portal redesigns its interface, every bot touching that portal breaks simultaneously. RPA works only with structured data and stable interfaces.
Level 3: Intelligent Automation (RPA + ML)
This level combines RPA bots with machine learning models that can handle semi-structured data and make probabilistic decisions. Optical character recognition (OCR) extracts data from scanned documents. Natural language processing (NLP) classifies clinical notes. ML models predict claim denial risk before submission.
Typical capabilities: OCR-based document intake for faxed referrals and authorization requests, ML-powered claim denial prediction (flagging high-risk claims before submission), NLP-assisted coding suggestions from clinical documentation, predictive scheduling that optimizes appointment slots based on historical no-show patterns.
Level 4: Agentic AI (Goal-Oriented Agents)
Agentic AI represents a fundamental shift from task automation to workflow automation. Instead of automating individual steps, an AI agent receives a goal ("process this prior authorization request") and orchestrates the entire workflow: reading clinical documentation, matching to payer criteria, assembling supporting evidence, submitting through the appropriate channel, and monitoring through to resolution.
As we detailed in our guide on 5 healthcare workflows that agentic AI will transform, these agents can reason about exceptions, adapt to changing payer requirements, and improve over time.
Typical capabilities: End-to-end prior authorization from clinical review to submission and tracking, denial root cause analysis with automated appeal generation, intelligent patient communications that understand billing questions and negotiate payment plans, cross-system orchestration spanning EHR, clearinghouse, payer portals, and billing platforms.
Level 5: Autonomous Operations (The Horizon)
The emerging frontier is autonomous healthcare operations where AI systems manage entire operational domains with minimal human oversight.
Self-healing workflows detect and resolve their own failures. Continuous learning loops improve performance without manual retraining. Human intervention is reserved for genuinely novel situations and strategic decisions, not routine processing.
Emerging capabilities: Self-optimizing revenue cycle that adjusts submission strategies based on real-time payer behavior, autonomous denial prevention that identifies and addresses root causes before claims are submitted, predictive resource allocation that adjusts staffing and capacity based on anticipated volume patterns.
No US health system operates at Level 5 today. A handful of well-funded health-tech companies are approaching Level 4 for specific workflows. The practical goal for most organizations in 2026 is to progress from Level 1-2 to Level 2-3, with targeted Level 4 deployments for the highest-value workflows like prior authorization and denial management.
10 Healthcare Workflows to Automate, Ranked by ROI
The following ranking is based on a composite score of implementation cost, time to value, annual savings potential, and impact on patient experience. For each workflow, we provide the current manual process, the automation approach, the recommended technology, integration requirements, expected ROI range, and a realistic implementation timeline. This analysis draws on data from industry benchmarks, ROI analyses, and our implementation experience.
1. Patient Scheduling and Reminders (ROI: 300-500%)
Current manual process: Front desk staff spends 15-25 minutes per patient on phone-based scheduling. No-show rates average 18.8% nationally, costing the US healthcare system over $150 billion annually. Rescheduling requires additional phone calls, manual waitlist management, and unfilled appointment slots that directly reduce revenue.
Automation approach: AI-powered scheduling systems that offer online self-scheduling with real-time availability, intelligent appointment matching based on visit type, provider expertise, and patient preferences, and predictive no-show modeling that overbook strategically. Automated multi-channel reminders (SMS, email, voice) sent at optimized intervals reduce no-shows by 15-40%.
Technology: AI scheduling platforms (e.g., Notable, Hyro, custom implementations). Integration with EHR scheduling modules via HL7 ADT messages or FHIR Appointment/Schedule resources.
Integration requirements: Bi-directional EHR scheduling API (FHIR R4 preferred), patient contact database, insurance eligibility feed, provider availability rules engine.
Expected ROI: Studies show 300-500% net ROI with cost recovery in 3-6 months. A mid-size practice with 50 providers can recover $500K-$1.2M annually through reduced no-shows and improved throughput.
Implementation timeline: 4-8 weeks for basic scheduling automation; 8-12 weeks with AI-powered optimization.
2. Registration and Eligibility Verification (ROI: 250-400%)
Current manual process: Registration staff spend 8-15 minutes per patient verifying demographics, insurance information, and benefit details. Manual eligibility checks require logging into multiple payer portals or calling insurance companies. Errors in registration data cascade through the entire revenue cycle, causing claim denials, delayed payments, and patient billing disputes.
Automation approach: Automated real-time eligibility verification via EDI 270/271 transactions at the point of scheduling (not just at check-in). Patient self-registration portals that capture demographics, insurance card images (OCR-processed), and consent forms before the visit. Automated benefit verification that identifies copays, deductibles, and coverage limitations.
Technology: RPA bots for payer portal interactions (Level 2), intelligent document processing for insurance card OCR (Level 3). FHIR Coverage and Patient Resources for standards-based integration.
Integration requirements: EDI 270/271 clearinghouse connection, EHR patient registration module, insurance card OCR engine, patient-facing portal or kiosk application.
Expected ROI: 250-400% within the first year. Eliminates 60-80% of manual verification calls, reduces registration errors by 40-55%, and prevents downstream denials caused by eligibility issues. Average savings: $3-$7 per patient encounter.
Implementation timeline: 3-6 weeks for EDI-based eligibility automation; 6-10 weeks with patient self-service portal.
3. Prior Authorization (ROI: 200-350%)
Current manual process: Clinical and administrative staff spend an average of 35-45 minutes per authorization request. This includes gathering clinical documentation from the EHR, identifying the payer's specific authorization requirements, completing payer-specific forms or portal submissions, and following up on pending requests. Practices submit an average of 43 prior authorizations per physician per week, according to a 2024 AMA survey.
Automation approach: AI agents that read clinical documentation from the EHR, match to payer-specific criteria from an updated policy database, assemble supporting evidence, submit through the payer's preferred channel (portal, fax, or API), and track through to resolution. As we analyzed in our guide on RPA vs agentic AI in healthcare, prior authorization is the canonical use case for agentic AI because it requires clinical reasoning that RPA cannot perform.
Technology: Agentic AI (Level 4) is the recommended approach. RPA alone scores only 3/10 for prior authorization because it cannot interpret clinical documentation or reason about medical necessity. AI agents with NLP can process clinical notes, match to criteria, and make judgment calls about documentation adequacy.
Integration requirements: EHR clinical documentation API (FHIR DocumentReference, Condition, Procedure resources), payer policy database, payer submission channel (portal API, Direct messaging, or fax gateway), status tracking system.
Expected ROI: 200-350%. Research shows 60% reduction in PA processing time, 35% decrease in administrative hours. Some organizations report 5x ROI in the first year with denial rates dropping by nearly a third. The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) taking effect January 1, 2026, mandates electronic prior authorization APIs for Medicare Advantage, Medicaid, and CHIP plans, creating both a compliance requirement and an automation enabler.
Implementation timeline: 8-16 weeks for full agentic AI deployment; 4-6 weeks for basic RPA-assisted submission.
4. Referral Management (ROI: 120-200%)
Current manual process: Referral coordinators manually process incoming and outgoing referrals. This involves receiving referral requests (often by fax), verifying insurance and authorization requirements, scheduling with the referred-to provider, and tracking completion. A single referral can generate 5-8 manual touchpoints across multiple staff members and systems.
Automation approach: OCR-driven referral intake that digitizes faxed referrals, intelligent routing based on specialty, insurance, location, and availability. Automated authorization triggering when required. Closed-loop tracking that alerts when referrals are not completed within defined timeframes.
Technology: Intelligent automation (Level 3) combining RPA for system navigation with OCR for document processing and ML for routing optimization. FHIR ServiceRequest resources for standards-based referral exchange.
Integration requirements: Your EHR referral module, fax-to-digital gateway with OCR, provider directory (FHIR PractitionerRole), insurance authorization rules, scheduling system for referred-to providers.
Expected ROI: 120-200%. Reduces referral processing time by 50-65%, improves referral completion rates from ~50% to 80%+, and recaptures revenue from completed referrals that would otherwise have been lost to leakage.
Implementation timeline: 6-10 weeks for automated intake and routing; 10-14 weeks with closed-loop tracking.
5. Clinical Documentation (ROI: 80-150%)
Current manual process: Physicians spend an estimated 2 hours on documentation for every 1 hour of patient care. Clinical documentation directly impacts coding accuracy, reimbursement levels, quality measure reporting, and legal compliance. Incomplete documentation is the root cause of 30-40% of claim denials.
Automation approach: Ambient clinical documentation using AI-powered speech recognition that listens to the patient-provider conversation and generates structured clinical notes. NLP-assisted documentation improvement that identifies missing elements required for accurate coding, quality reporting, and clinical decision support. Computer-assisted documentation (CAD) that suggests diagnosis specificity improvements.
Technology: Ambient documentation runs on agentic AI (Level 4). NLP models for documentation quality analysis. Integration via FHIR DocumentReference, Composition, and ClinicalImpression resources.
Integration requirements: EHR note authoring module API, speech-to-text engine, NLP clinical language model, CDI query system, quality measure rules engine.
Expected ROI: 80-150%. The ROI calculation is complex because the primary benefit is physician time recovery (reducing documentation burden from 2:1 to 1:1 or better), with secondary benefits in coding accuracy, denial reduction, and quality measure compliance. Organizations using ambient documentation report 50-70% reduction in after-hours documentation time.
Implementation timeline: 8-12 weeks for ambient documentation pilot; 12-20 weeks for organization-wide deployment with CDI integration.
6. Order Management (ROI: 100-180%)
Current manual process: Managing clinical orders, from lab tests to imaging studies to prescriptions, involves verifying order appropriateness, checking for duplicates, confirming insurance coverage, routing to the correct fulfillment location, and tracking completion. Order management errors account for 10-15% of clinical workflow inefficiencies.
Automation approach: Rules-based order screening for clinical decision support (duplicate checking, drug interaction alerts, appropriateness criteria). Automated insurance verification and prior authorization triggering for high-cost orders. Intelligent routing based on patient location, urgency, and facility capabilities. Automated result tracking with exception alerts.
Technology: Most order types only need intelligent automation (Level 3). FHIR ServiceRequest, MedicationRequest, and Task resources for interoperable order management.
Integration requirements: The EHR CPOE module, pharmacy system, laboratory information system (LIS), radiology information system (RIS), insurance eligibility and authorization systems.
Expected ROI: 100-180%. Primary savings from reduced duplicate orders (5-8% reduction), improved order completion rates, and faster turnaround times. Secondary benefits from reduced phone calls for order clarification.
Implementation timeline: Plan for 6-10 weeks for rules-based order screening; 10-16 weeks with intelligent routing and tracking.
7. Coding and Charge Capture (ROI: 150-250%)
Current manual process: Certified coders review clinical documentation to assign ICD-10 diagnosis codes and CPT/HCPCS procedure codes. Research indicates that 41% of medical claims contain coding errors that lead to denials, delays, and lost revenue. Manual coding takes 10-20 minutes per encounter, and the US faces a growing shortage of certified coders.
Automation approach: Computer-assisted coding (CAC) that reads clinical documentation using NLP, suggests appropriate codes, verifies compliance with CCI edits and LCD/NCD policies, and flags potential under-coding or over-coding. Automated charge capture that ensures all billable services are captured at the point of care.
Technology: Agentic AI (Level 4) for full NLP-based coding. ML models trained on coding patterns and payer-specific requirements. As analyzed in our comprehensive guide on 12 revenue cycle workflows for automation, coding is one of the highest-impact AI use cases because it sits at the intersection of clinical documentation and financial performance.
Integration requirements: Plan on the EHR clinical documentation API, a coding knowledge base (ICD-10, CPT, HCPCS), CCI edit engine, LCD/NCD policy database, charge capture interface, and practice management billing system.
Expected ROI: 150-250%. AI coding systems report 38% reduction in coding errors and up to 25% decrease in coding-related administrative costs. A 200-provider organization can save $400K-$800K annually through improved coding accuracy and faster turnaround.
Implementation timeline: 8-12 weeks for CAC implementation; 12-20 weeks for full AI coding with charge capture integration.
8. Claims Submission (ROI: 200-300%)
Current manual process: Claims submission involves assembling claim data from multiple sources (demographics, insurance, clinical codes, charges), scrubbing for errors, formatting to payer specifications (837P/837I), and transmitting through a clearinghouse. Claims processors handle 40-60 claims per hour manually, with error rates of 5-15% requiring rework.
Automation approach: Automated claim assembly from EHR and billing system data. AI-powered claim scrubbing that checks for 500+ error patterns beyond basic edits (payer-specific requirements, historical denial patterns, documentation completeness). Intelligent submission routing that selects the optimal clearinghouse or direct submission path. Real-time claim tracking with automated status updates.
Technology: Intelligent automation (Level 3) for claim scrubbing and submission. RPA (Level 2) for basic claim status checking. EDI 837/835/277 transactions for standards-based exchange.
Integration requirements: Practice management billing system, clearinghouse EDI connection, payer-specific submission portals, claim scrubbing rules engine, real-time adjudication tracking.
Expected ROI: 200-300%. Increasing clean claim rates from 80% to 95%+ eliminates rework costs of $25-$181 per denied claim. Staff time on manual claims follow-up decreases by 40%. Organizations report AR days reduced by 15-25 days.
Implementation timeline: Expect 4-8 weeks for automated claim scrubbing; 8-12 weeks with intelligent submission routing and tracking.
9. Denial Management (ROI: 180-280%)
Current manual process: When claims are denied, staff must identify the denial reason, analyze the root cause, determine the appropriate response (correct and resubmit, appeal, write off), execute the response, and track through to resolution. Providers spend approximately $20 billion annually on denial management. The average cost to rework a denied claim increased from $43.84 in 2022 to $57.23 in 2023.
Automation approach: AI-powered denial categorization and root cause analysis. Automated appeal generation with clinical evidence assembly. Pattern detection that identifies systemic denial drivers and recommends preventive actions. Predictive models that flag high-risk claims before submission. As companies like Adonis (which achieved 4x+ revenue growth in 2025) have demonstrated, AI-native denial management platforms are delivering measurable results.
Technology: This is agentic AI (Level 4) territory — root cause analysis and appeal generation. ML models for denial prediction and pattern detection. Basic denial routing and status tracking can stay on RPA (Level 2).
Integration requirements: Clearinghouse remittance feed (EDI 835/277), EHR clinical documentation API, coding history database, payer policy database, appeal submission channels.
Expected ROI: 180-280%. BDO analysis shows that 69% of organizations using AI for denial management report improved claims success rates. Denial overturn rates improve from 45% to 70%+, and the time to resolve denials drops from 30-60 days to 7-14 days.
Implementation timeline: 6-10 weeks for automated categorization and routing; 10-16 weeks with AI-powered appeal generation and predictive prevention.
10. Patient Billing and Collections (ROI: 140-220%)
Current manual process: Patient billing involves generating statements, processing payments, managing payment plans, handling billing inquiries, and pursuing collections on outstanding balances. As patient financial responsibility continues to grow (high-deductible health plans now cover 55% of employer-sponsored enrollees), patient collections have become both more important and more difficult. Manual billing inquiries take 8-15 minutes per call, and collection rates on patient balances average 50-60%.
Automation approach: Statement generation and multi-channel delivery (paper, email, text, portal). AI-powered patient communications that handle billing inquiries, explain charges, check payment plan eligibility, and negotiate within defined parameters. Predictive analytics for propensity-to-pay scoring that optimizes collection strategies. Self-service payment portals and mobile payment options.
Technology: Conversational billing assistants need agentic AI (Level 4). Intelligent automation (Level 3) for statement generation and payment processing. RPA (Level 2) for batch payment posting.
Integration requirements: Practice management billing system, patient payment portal, payment processing gateway, patient communication platform (SMS, email, IVR), financial assistance eligibility database.
Expected ROI: 140-220%. Patient collection rates improve from 50-60% to 70-80% through better engagement and self-service options. Billing inquiry call volume decreases 30-50%. Staff time on manual payment posting drops by 60-75%.
Implementation timeline: 4-8 weeks for automated billing and self-service payments; 8-14 weeks with AI-powered conversational billing.
Technology Stack Comparison: Choosing the Right Platform
Healthcare organizations evaluating automation platforms face a three-way decision between established RPA platforms, Microsoft's Power Platform ecosystem, and custom AI agent architectures. The right choice depends on your existing technology stack, the complexity of target workflows, internal engineering capability, and budget constraints. Here is the honest comparison based on 2026 market analysis.
UiPath: The Enterprise RPA Leader
UiPath dominates the healthcare RPA market, serving 75% of the top 100 US health systems. At ViVE 2026, UiPath launched agentic AI solutions targeting medical records summarization, claim denial prevention, and prior authorization, developed in partnership with healthcare AI company Genzeon.
Strengths: Pre-built healthcare components (CMS claims conversion, insurance claim capture), enterprise-grade audit trails, HIPAA compliance infrastructure, largest marketplace of reusable automation components, strong RPA + AI hybrid capabilities.
Limitations: Significant upfront capital expenditure ($100K-$300K annually for enterprise licenses), steep learning curve requiring dedicated RPA developers, maintenance-intensive for screen-scraping bots.
Best for: Large health systems (500+ beds) with dedicated IT teams, complex multi-system automation needs, and existing UiPath investments.
Microsoft Power Automate: The Ecosystem Play
Power Automate is the most cost-effective option for organizations already embedded in the Microsoft 365 ecosystem. Combined with Azure AI services (OpenAI, Document Intelligence, Bot Framework), it provides a unified platform for hybrid automation.
Strengths: Native integration with Microsoft 365, Teams, Dynamics, and Azure. Lower cost entry point ($40K-$120K annually). Azure HIPAA BAA for compliant deployment. Citizen-developer friendly low-code interface that allows non-technical staff to build simple automations.
Limitations: Lacks advanced orchestration capabilities compared to UiPath. Browser automation is not as robust for complex healthcare portal interactions. Limited healthcare-specific pre-built components. Not ideal for high-volume, complex RPA scenarios.
Best for: Mid-size organizations (100-500 beds) already on Microsoft 365, organizations prioritizing low-code/citizen-developer approaches, budget-conscious deployments under $150K.
Custom AI Agent Architecture: The Intelligence Play
Custom AI agent architectures use large language models (GPT-4, Claude, Gemini) combined with healthcare-specific fine-tuning, FHIR/HL7 integration layers, and purpose-built orchestration to create agents that reason about clinical and administrative workflows.
Strengths: Highest intelligence ceiling, able to handle complex reasoning workflows (prior auth, denial management, coding) that RPA platforms cannot. API-first integration (FHIR, HL7, X12 EDI) that is more resilient than screen scraping. Model-agnostic (can switch between GPT-4, Claude, open-source models as the market evolves). Non-linear scalability (one agent architecture handles many workflow variations).
Limitations: Requires ML engineering expertise (expensive, scarce talent). Longer development cycles (8-16 weeks per agent vs 2-6 weeks per RPA bot). Higher upfront investment ($150K-$400K). Ongoing API costs for LLM inference.
Best for: Organizations targeting Level 4 agentic automation, technology-forward health systems willing to invest in long-term competitive advantage, workflows requiring clinical reasoning and unstructured data processing.
The Hybrid Recommendation
For most healthcare organizations in 2026, the optimal approach is a hybrid stack: Power Automate or UiPath for structured, repetitive workflows (eligibility verification, payment posting, claim status) combined with custom AI agents for reasoning-intensive workflows (prior authorization, denial management, coding review). This hybrid approach delivers 20-45% lower TCO over three years compared to any single-platform strategy.
Change Management: The Human Side of Healthcare Automation
Technology selection is the easy part. The harder challenge is organizational change management, and it is where most healthcare automation initiatives fail. Industry analysis shows that 30-50% of healthcare automation projects fail to deliver expected ROI, and the primary failure mode is not technology. It is resistance from staff who fear job displacement, clinicians who distrust AI-generated outputs, and middle management that loses control over manual processes they have built their careers around.
Phase 1: Assessment and Buy-In (Months 0-3)
Identify clinical champions: Find 2-3 physicians or nurses who are frustrated with manual processes and willing to advocate for automation. Their credibility with peers is more powerful than any executive mandate.
Map current pain points with data: Do not assume you know where the problems are. Time-study 5-10 key workflows: how many minutes per transaction, how many exceptions, how many handoffs between people and systems. Use these numbers to build an evidence-based business case, not vendor-supplied estimates.
Set measurable success criteria before starting: Define what success looks like in numbers: processing time reduction target, error rate target, FTE hours saved target, and financial impact target. Without pre-defined metrics, success becomes subjective and political.
Address job displacement fears directly: Be transparent. Automation will eliminate some tasks, not people. Staff whose repetitive tasks are automated will be retrained for higher-value work: complex exception handling, patient relationship management, quality improvement, and automation governance. Document this commitment in writing.
Phase 2: Pilot and Prove (Months 3-6)
Select 1-2 high-impact, low-risk workflows: Patient scheduling/reminders and eligibility verification are ideal pilot candidates because they have high volume, structured data, measurable outcomes, and limited clinical risk if errors occur.
Train the core team (40 hours minimum): Invest in proper training for the 5-8 staff members who will operate and oversee the automated workflows. This is not a 2-hour demo; it is hands-on training covering normal operations, exception handling, escalation procedures, and basic troubleshooting.
Run a 90-day pilot with parallel operations: Run the automated workflow alongside the manual process for the first 30 days. Compare outputs. Identify discrepancies. Only transition fully after validating accuracy and reliability.
Document and publicize quick wins: Share pilot results widely. A dashboard showing "3,200 eligibility checks automated this month, 47 staff hours saved, 12 denial-causing errors caught" builds momentum for expansion.
Phase 3: Scale and Integrate (Months 6-12)
Expand to 5-10 workflows based on pilot learnings. Cross-train departments. Establish an automation governance board that includes clinical, operational, IT, compliance, and finance leadership. Integrate automated workflows with each other, creating connected automation chains (e.g., scheduling triggers eligibility check, which triggers authorization if needed).
Phase 4: Optimize and Sustain (Months 12-18)
Continuous improvement cycles based on performance data. Staff upskilling programs that develop automation literacy across the organization. Introduction of advanced AI capabilities for the highest-complexity workflows. Build a culture where automation is a tool that empowers staff, not a threat that replaces them.
Regulatory Considerations: HIPAA, State Laws, and Federal Mandates
Healthcare workflow automation operates within one of the most heavily regulated environments in any industry. Non-compliance is not a business risk; it is an existential risk. Key regulatory considerations for 2026:
HIPAA and PHI Protection
Every automated workflow that touches patient data must comply with HIPAA Privacy and Security Rules. This means: Business Associate Agreements (BAAs) with every technology vendor that processes PHI, encryption in transit (TLS 1.2+) and at rest (AES-256) for all data, role-based access controls that limit automation systems to the minimum necessary data, comprehensive audit trails that log every data access, transformation, and transmission, and breach notification procedures that account for automated processing.
For AI-based automation specifically, ensure that PHI used for model training is de-identified in accordance with HIPAA Safe Harbor or Expert Determination methods. LLM-based agents should process PHI only within BAA-covered infrastructure (Azure OpenAI with healthcare BAA, AWS Bedrock with BAA, or on-premises deployment).
CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F)
Taking effect January 1, 2026, this rule mandates that Medicare Advantage, Medicaid, and CHIP plans implement FHIR-based APIs for prior authorization, including a Patient Access API that reports authorization status and a Provider Access API that supports electronic prior authorization requests. This creates both a compliance requirement and a powerful automation enabler: payers must accept electronic authorization requests via standardized APIs, eliminating the payer portal fragmentation that has historically limited automation.
21st Century Cures Act and Information Blocking
The Cures Act prohibits information blocking by healthcare providers, health IT developers, and health information exchanges. Automated workflows must ensure that data flows freely between systems and providers. Automation that restricts or delays information sharing (even unintentionally) could constitute information blocking under ONC regulations.
State-Level AI Regulations
Several states are implementing or considering AI-specific regulations for healthcare. Colorado's AI Act (SB 24-205) requires impact assessments for high-risk AI systems, which may include automated clinical documentation and coding tools. California and New York have proposed similar legislation. Healthcare organizations must monitor state-level requirements and ensure their automation governance includes AI impact assessment capabilities.
Measurement Framework: Proving and Improving Automation ROI
You cannot improve what you do not measure, and you cannot justify continued investment without proving returns. The measurement framework below provides a structured approach to tracking automation performance across four dimensions.
Operational Metrics
- Process cycle time: Measure end-to-end time for each automated workflow. Target: 50-80% reduction from manual baseline. Example: prior authorization from 35 minutes to 7 minutes.
- Manual touchpoints eliminated: Count the number of human interventions per workflow. Target: reduce from 5-8 touchpoints to 1-2 (exception handling only).
- Exception rate: Percentage of transactions requiring human intervention. Target: below 10% for mature automations. If exception rates exceed 20%, the automation needs re-engineering.
- First-pass resolution rate: Percentage of transactions completed without rework. Target: 90%+ for Level 3 automations, 95%+ for Level 4.
Financial Metrics
- Cost per transaction: Total cost (technology + staff + overhead) divided by transactions processed. Compare to manual cost per transaction. Target: 60-80% reduction.
- Revenue recovered: Dollar value of revenue captured through improved clean claim rates, successful denial appeals, and reduced write-offs. This is often the largest single ROI component.
- FTE hours saved per month: Measure actual staff hours freed by automation. Track how those hours are redeployed (higher-value tasks vs. eliminated positions). Target: 700-980 hours annually per automated workflow, based on industry benchmarks.
- ROI percentage: (Total benefits minus total costs) divided by total costs, expressed as a percentage. Target: 200%+ in Year 1 for high-ROI workflows (scheduling, eligibility, claims). The average ROI for AI in healthcare is $3.20 for every $1 invested.
Quality Metrics
- Error rate: Track errors introduced by automation (false positives, incorrect data transformations, missed exceptions). Compare to manual error rates. Target: 50%+ reduction.
- Clean claim rate: Percentage of claims accepted on first submission. Target: 95%+ (up from industry average of 80-85%). Each percentage point improvement represents significant revenue recovery.
- Patient satisfaction scores: Measure impact on patient experience through scheduling convenience, billing transparency, and communication quality. Use HCAHPS or CG-CAHPS for standardized measurement.
- Compliance audit pass rate: Track performance on HIPAA audits, coding audits, and regulatory compliance reviews. Automation should improve compliance by creating consistent, auditable processes.
Strategic Metrics
- Automation coverage: Percentage of total addressable workflows that are automated at Level 2 or higher. Track progression quarter over quarter.
- Staff satisfaction and engagement: Survey staff working with automated systems quarterly. Track whether automation is perceived as empowering or threatening.
- Time-to-automation: How quickly can new workflows be automated? As organizational capability matures, this should decrease from 8-12 weeks to 3-4 weeks for standard workflow types.
Implementation Roadmap: A Phased Approach for 2026
Based on the ROI rankings and maturity model above, here is a realistic 18-month roadmap for a mid-size healthcare organization (200-500 beds) starting from Level 1-2 maturity:
Quarter 1: Quick Wins (Months 1-3)
Deploy automation for the two highest-ROI, lowest-complexity workflows: patient scheduling/reminders and eligibility verification. Use RPA or Power Automate for structured, repetitive tasks. Establish baseline metrics for all target workflows. Build the business case for expanded investment using pilot results.
Budget: $75K-$150K. Expected savings: $200K-$400K annually once stabilized.
Quarter 2: Revenue Cycle Core (Months 4-6)
Add claims submission automation (AI-powered scrubbing) and basic denial management (automated categorization and routing). Begin the prior authorization automation initiative (longer implementation cycle). These workflows drive the largest direct financial impact.
Budget: $150K-$300K. Expected savings: $500K-$1M annually once stabilized.
Quarter 3-4: Intelligence Layer (Months 7-12)
Deploy agentic AI for prior authorization (full workflow), denial management (root cause analysis and appeal generation), and coding review. Integrate automated workflows into connected chains. Build the orchestration layer that routes work to the appropriate technology.
Budget: $200K-$400K. Expected savings: $800K-$1.5M annually once stabilized.
Quarter 5-6: Optimization and Expansion (Months 13-18)
Expand to clinical documentation, order management, referral management, and patient billing. Optimize existing automations based on 6-12 months of performance data. Build continuous improvement capabilities. Develop internal automation expertise for ongoing development and maintenance.
Budget: $150K-$300K. Expected savings: $1.2M-$2.5M annually once all workflows are stabilized.
Total 18-month investment: $575K-$1.15M. Total annual savings at steady state: $2.7M-$5.4M. Payback period: 6-12 months for the full program.
Conclusion
Healthcare workflow automation is not an emerging technology. It is mature, proven, and delivers measurable ROI across thousands of healthcare organizations. The CMS Interoperability and Prior Authorization Final Rule, taking effect in January 2026, combined with the rapid maturation of agentic AI, has created a unique window where the technology, the regulatory environment, and the economic pressure are all aligned.
The organizations that will lead healthcare operations in 2028 are the ones making automation investments today, not in pilot programs that generate reports, but in production deployments that eliminate manual processes, recover revenue, reduce staff burnout, and improve patient experience.
The $265 billion administrative waste problem is not going to solve itself. It is going to be automated away, workflow by workflow, by the organizations willing to invest in the operational architecture to do it.
Start with scheduling and eligibility. Prove value in 90 days. Scale to the full revenue cycle within 18 months. The ROI data is unambiguous, the technology is ready, and the cost of inaction is $1 trillion per year and growing.


