Your health system processes 50,000 HL7v2 messages per day across 14 departments. Your EHR vendor just released a FHIR R4 API. A startup partner wants real-time ADT notifications. Your lab system still speaks ASTM. And someone in the C-suite read a Gartner report about "interoperability platforms" and wants a recommendation by Friday.
This is the moment where most healthcare IT teams make a decision that locks them in for 5-10 years. They pick a platform based on a vendor demo, a colleague's recommendation, or whatever showed up first in a Google search. Eighteen months later, they are managing 47 interfaces with duct tape and bash scripts, wondering where it all went wrong.
The healthcare integration market is projected to reach $7.1 billion by 2026, growing at 12.4% CAGR. That growth is driven by regulatory pressure (ONC's HTI-1 mandates USCDI v3 by January 2026), the proliferation of FHIR APIs, and health systems connecting more external partners than ever. The platform you choose determines whether you spend the next five years building interfaces or fighting fires.
This guide gives you the decision framework we use at Nirmitee when advising health systems on integration architecture. No vendor favoritism — just the engineering trade-offs that actually matter.
The Three Integration Architecture Patterns
Before evaluating specific platforms, understand the three fundamental patterns. Every integration platform implements one of these — and each has structural trade-offs that no vendor demo will surface.
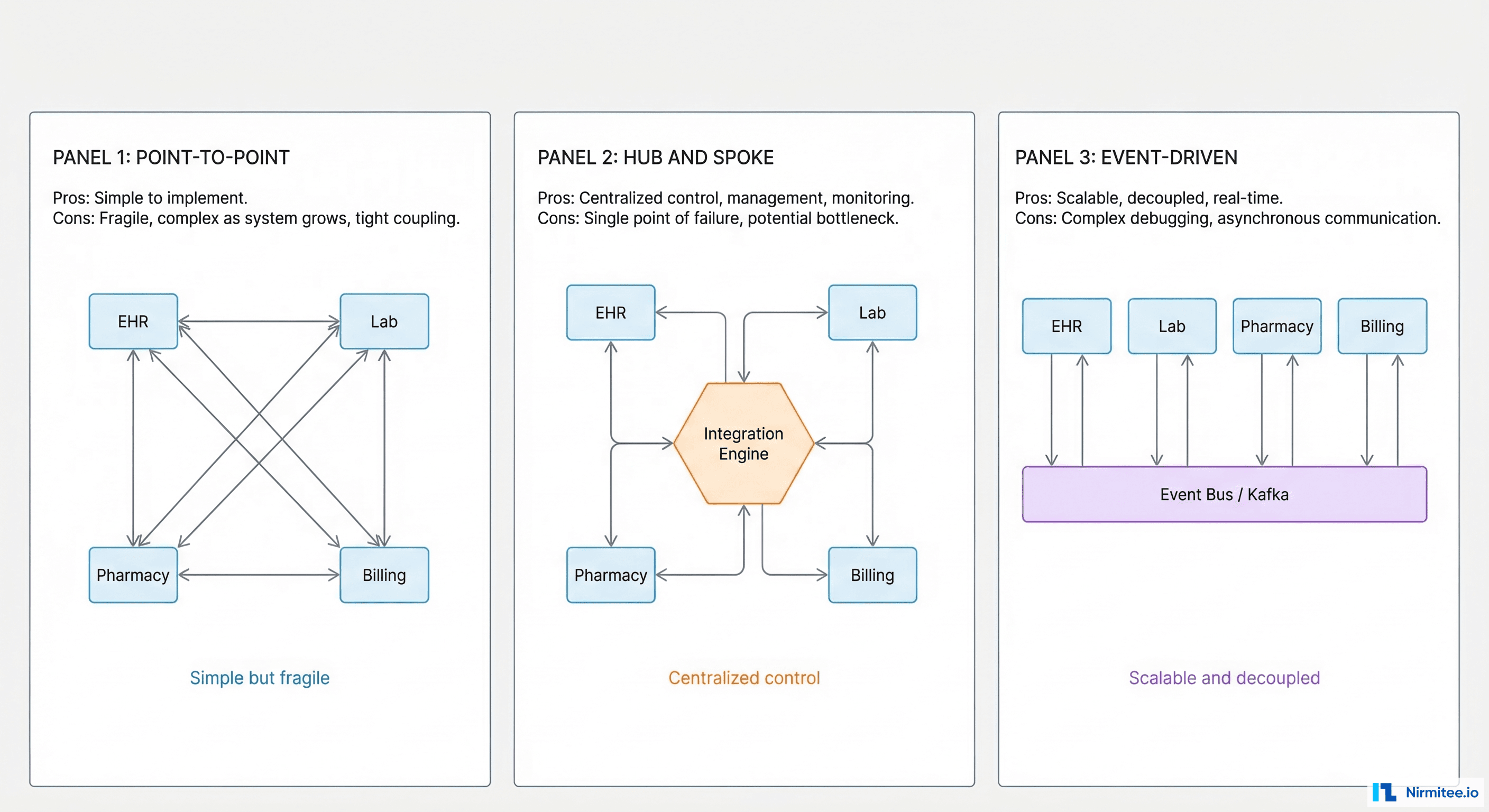
Pattern 1: Point-to-Point
Every system connects directly to every other system. EHR talks to lab, lab talks to pharmacy, pharmacy talks to billing. Simple when you have 3 systems. Catastrophic when you have 15.
The math is unforgiving: n systems require n(n-1)/2 interfaces. Five systems need 10 interfaces. Ten systems need 45. Twenty systems need 190. Each interface is a custom build with its own mapping logic, error handling, and monitoring. When the lab system upgrades their HL7 version, you touch every interface connected to it.
When it works: Small clinics with 2-3 systems and no growth plans. Temporary bridges during migration projects. Proof-of-concept integrations that will be replaced.
When it fails: Any organization planning to add systems, connect external partners, or scale beyond a single site.
Pattern 2: Hub-and-Spoke (Integration Engine)
All systems connect to a central integration engine. The engine handles message routing, transformation, and protocol translation. EHR sends an ADT message to the engine; the engine transforms it and routes copies to lab, pharmacy, and billing in whatever format each system needs.
This is the dominant pattern in US healthcare. Mirth Connect, Rhapsody, Iguana, and Oracle's Integration Cloud all implement hub-and-spoke. The engine becomes your single point of control — and your single point of failure.
When it works: Mid-size health systems (5-50 interfaces), organizations with a dedicated integration team, environments where HL7v2 is the dominant protocol.
When it fails: When the engine cannot handle your message volume. When you need sub-second latency for clinical alerts. When your architecture requires event replay or temporal queries.
Pattern 3: Event-Driven (Message Bus)
Systems publish events to a message bus (Kafka, RabbitMQ, AWS EventBridge). Consumers subscribe to the events they need. No central engine transforms messages — each consumer handles its own transformation.
This pattern decouples producers from consumers. The lab system publishes a "result available" event without knowing or caring who consumes it. Adding a new consumer (a population health dashboard, a research data warehouse) requires zero changes to the producer.
When it works: Large enterprises with 50+ interfaces, real-time analytics requirements, multi-site deployments, organizations building a FHIR data pipeline for AI/ML.
When it fails: When your team lacks distributed systems experience. When most of your integrations are simple HL7v2 pass-through. When you are a 3-person IT shop.
The Decision Framework: 7 Questions That Determine Your Platform
We have evaluated integration platforms for health systems ranging from 5-bed rural clinics to 2,000-bed academic medical centers. These seven questions predict the right architecture with 90%+ accuracy.
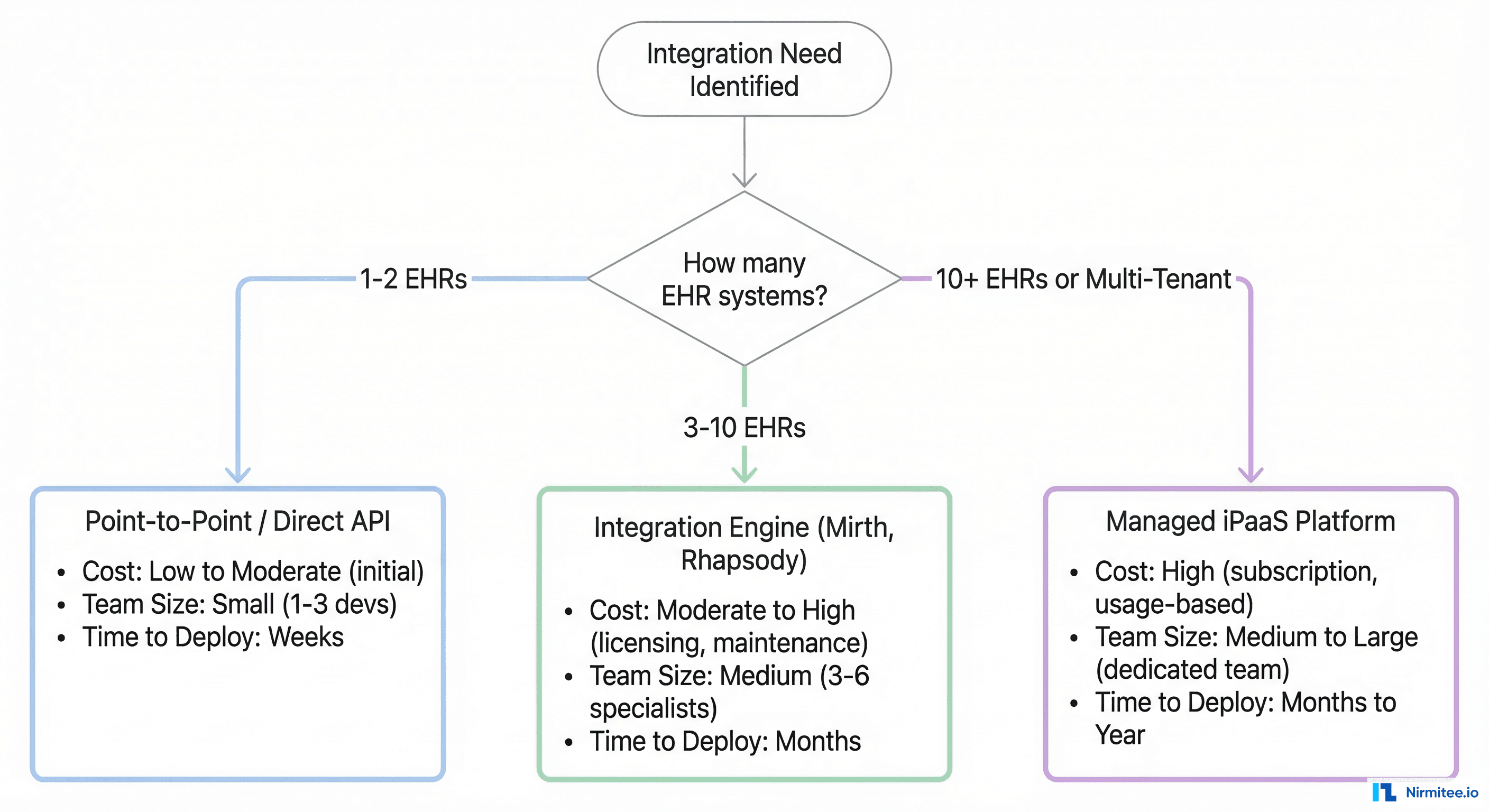
Question 1: How Many Active Interfaces Do You Need in 12 Months?
Not how many you have today — how many you will have in 12 months. Health systems consistently underestimate this by 40-60%. If you have 20 interfaces today, plan for 30-35 within a year (new EHR modules, payer connections, patient engagement apps, analytics feeds).
- Under 10 interfaces: Point-to-point or a lightweight integration engine. You do not need a $200K/year iPaaS platform.
- 10-50 interfaces: Integration engine (Mirth Connect, Rhapsody, or Iguana). This is the sweet spot for hub-and-spoke.
- 50+ interfaces: Integration engine + event bus hybrid architecture. Pure hub-and-spoke starts breaking at this scale.
Question 2: What Protocols Does Your Environment Actually Use?
Inventory every protocol in your environment. Most health systems discover a longer list than expected:
- HL7 v2.x — Still 80%+ of clinical messaging (ADT, ORM, ORU, SIU)
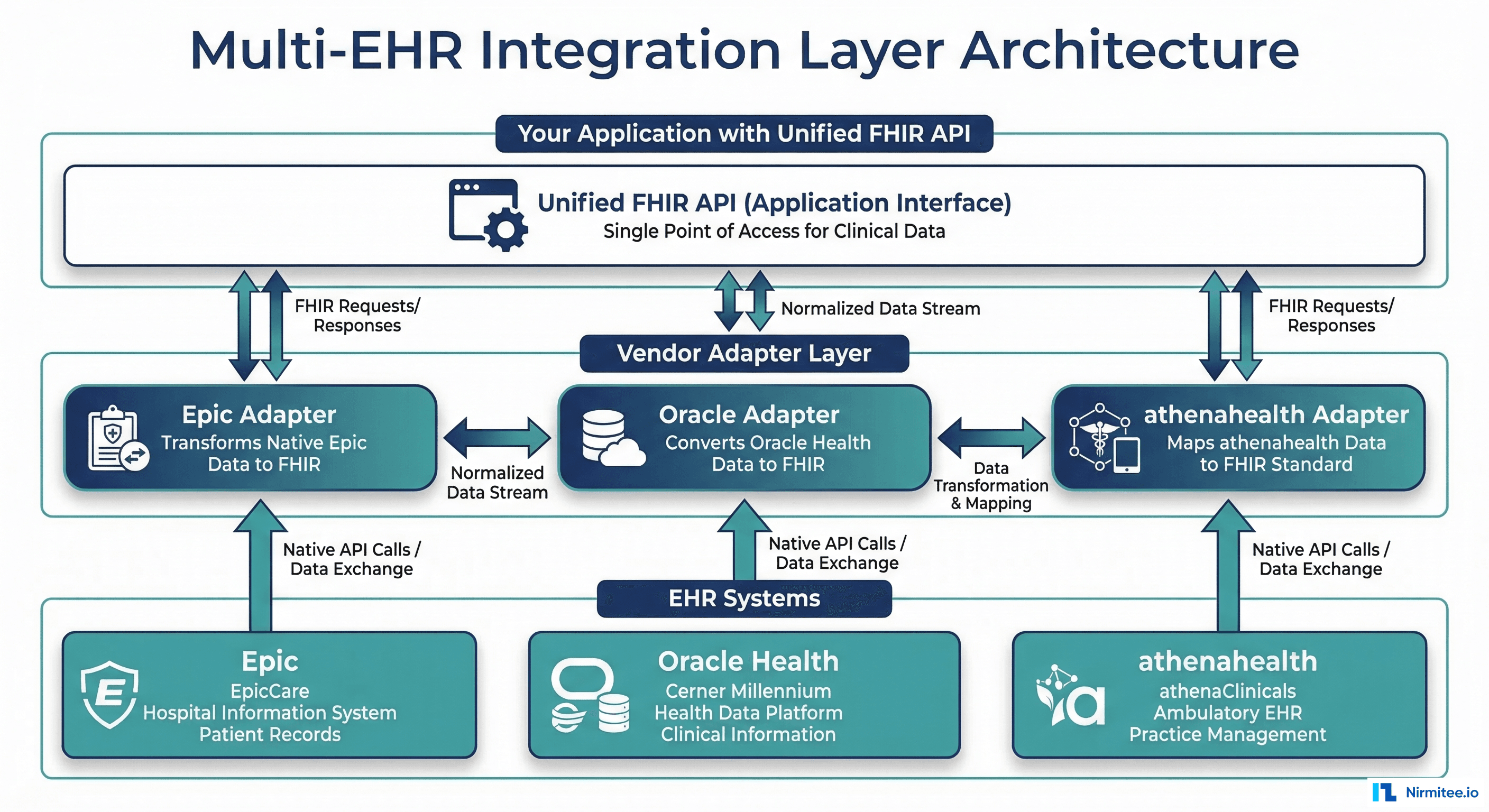
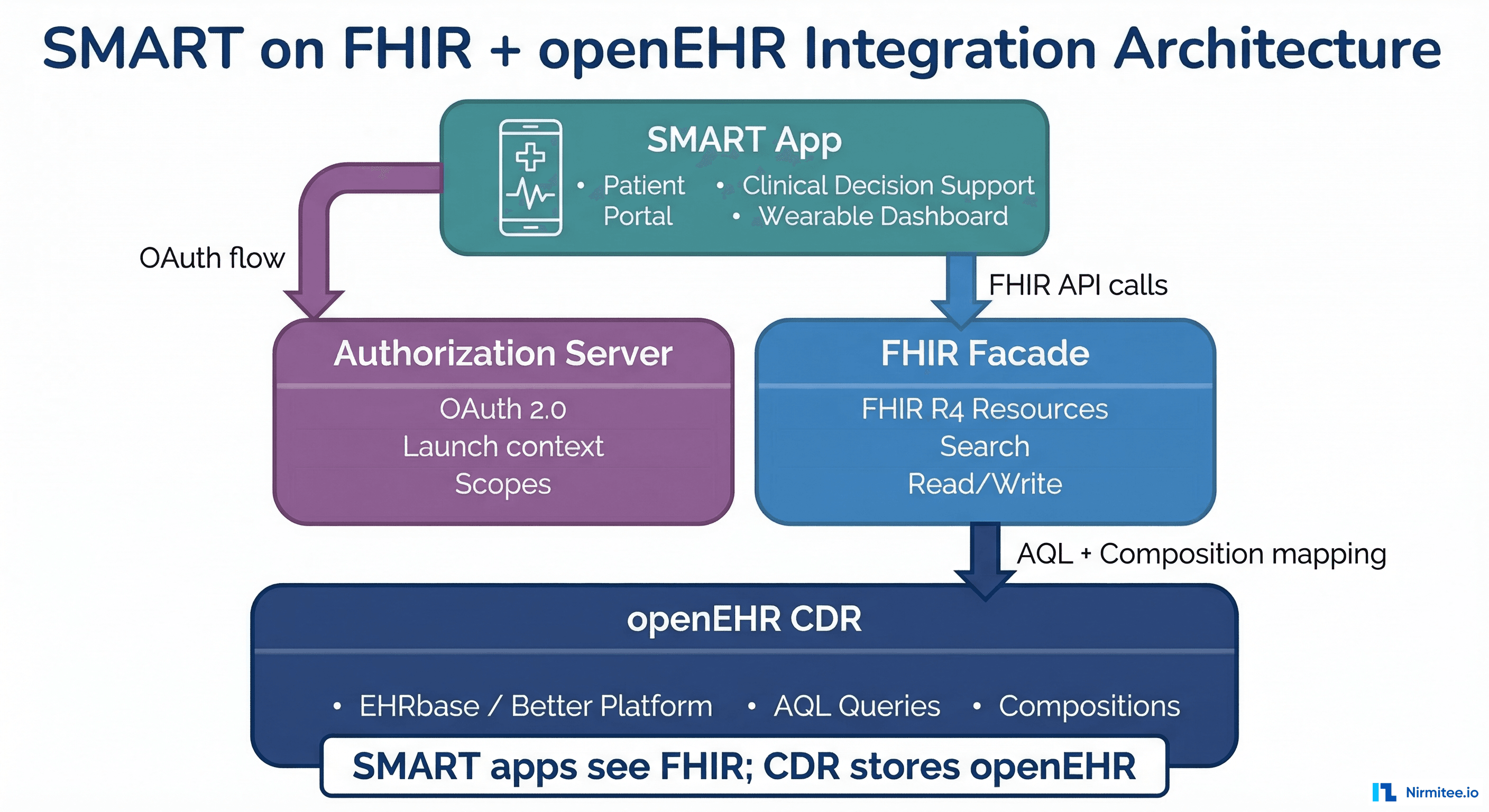
- FHIR R4 — Growing fast for patient access APIs, CDS Hooks, SMART apps
- DICOM — Radiology/imaging (often forgotten in platform evaluations)
- X12 EDI — Claims, eligibility, prior authorization (835, 837, 270/271)
- NCPDP SCRIPT — E-prescribing (NCPDP is not replaceable by FHIR)
- Direct/SMTP — Clinical document exchange (C-CDA via Direct messaging)
- Custom REST/SOAP APIs — Vendor-specific APIs that follow no standard
Your platform must natively support the protocols you use today, not just the ones you aspire to use. A FHIR-only platform is useless when 80% of your interfaces are HL7v2.
Question 3: What Is Your Realistic Engineering Budget?
Integration platform costs are deceptive. The license fee is 20-30% of total cost of ownership. Here is the real breakdown:
| Cost Component | Mirth Connect (Open Source) | Mirth Connect (Commercial) | Rhapsody / Iguana | Managed iPaaS (Redox, Health Gorilla) |
|---|---|---|---|---|
| Year 1 License/Subscription | $0 | $50K-150K | $80K-250K | $100K-400K |
| Infrastructure (hosting, HA) | $15K-40K | $15K-40K | $10K-30K | $0 (included) |
| Integration Engineers (1-3 FTEs) | $120K-360K | $120K-360K | $120K-360K | $60K-180K (fewer needed) |
| Training and Onboarding | $10K-30K | $5K-15K | $10K-25K | $5K-10K |
| Year 1 Total | $145K-430K | $190K-565K | $220K-665K | $165K-590K |
| 3-Year TCO | $400K-1.1M | $550K-1.4M | $600K-1.6M | $450K-1.5M |
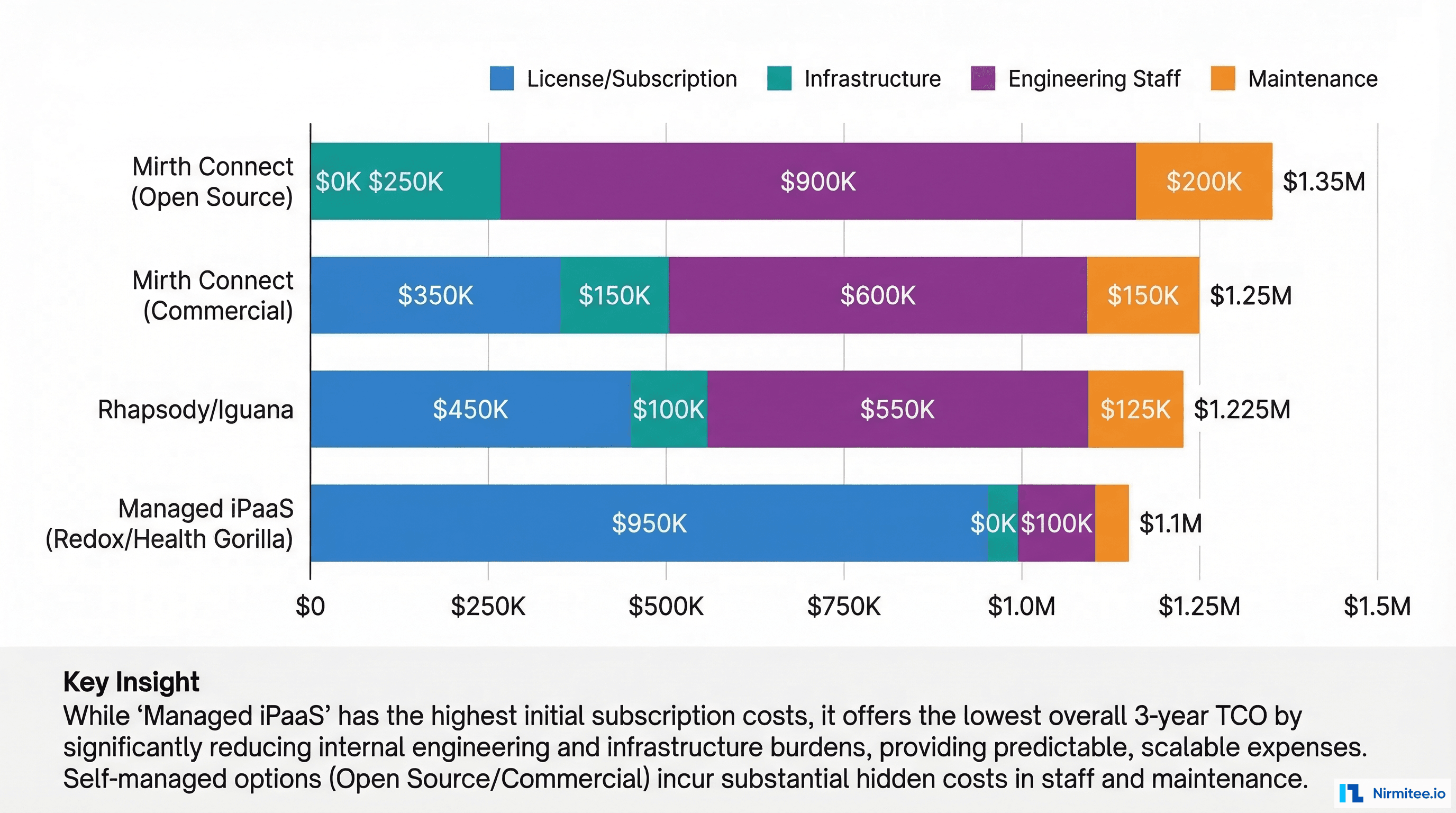
The counterintuitive finding: open-source Mirth Connect is not always the cheapest option. When you factor in the 2-3 senior engineers needed to operate it, a managed iPaaS can be cheaper for small teams. Conversely, at scale (50+ interfaces), the per-interface cost of managed platforms becomes prohibitive.
Question 4: Does Your Team Have Integration Engineering Expertise?
This is the question most organizations skip — and the one that causes the most failures. Hiring and retaining integration engineers is genuinely difficult. The talent pool is small because healthcare integration requires a rare combination of skills: HL7 message parsing, clinical workflow understanding, database administration, and network engineering.
- No dedicated integration team: Managed iPaaS (Redox, Health Gorilla, Particle Health). You are buying expertise, not just software.
- 1-2 integration engineers: Commercial Mirth Connect or Iguana. You need vendor support and a platform that reduces operational overhead.
- 3+ experienced integration engineers: Open-source Mirth Connect or Rhapsody. Your team can operate and customize the platform without vendor hand-holding.
Question 5: What Are Your Compliance and Data Residency Requirements?
Every healthcare integration platform processes PHI. Where that PHI lives and who can access it determines your compliance posture:
- On-premises only: Mirth Connect (self-hosted), Rhapsody (self-hosted), InterSystems HealthShare. Required by some government health systems, VA facilities, and organizations with strict data sovereignty policies.
- Cloud-hosted with BAA: Most platforms offer this. Verify the BAA covers the specific services used, not just "the platform generally."
- Multi-tenant SaaS: Managed iPaaS platforms. Your data transits through shared infrastructure. The BAA and SOC 2 Type II reports are non-negotiable prerequisites.
If your compliance team requires all PHI to remain within your network boundary, managed iPaaS is off the table regardless of its other advantages.
Question 6: What Message Volumes Must You Handle?
Message volume determines whether you need horizontal scaling, clustering, or a fundamentally different architecture:
- Under 10,000 messages/day: Any platform handles this. Not a differentiator.
- 10,000-100,000 messages/day: You need a platform with proven clustering support. Mirth Connect can handle 10,000+ messages/hour with proper tuning, but requires deliberate performance engineering.
- 100,000+ messages/day: You need an event-driven architecture (Kafka + integration engine). No single integration engine handles this gracefully without horizontal scaling.
Question 7: How Fast Do New Interfaces Need to Go Live?
This is the question that separates platforms designed for developers from platforms designed for operations teams:
- Managed iPaaS: 2-4 weeks for a standard interface (Epic ADT, Cerner labs). Pre-built connectors do most of the work.
- Commercial integration engine: 4-8 weeks including testing and go-live. Your team builds the channel from templates.
- Open-source Mirth Connect: 4-12 weeks depending on team experience. Full flexibility but no pre-built connectors — everything is custom.
Platform-by-Platform Breakdown
Mirth Connect (NextGen Healthcare)
The most widely deployed open-source integration engine in US healthcare. Mirth Connect has been the default choice for budget-conscious health systems since 2006. In 2024, NextGen transitioned Mirth to a commercial license model for version 4.6+, which changes the calculus significantly.
Strengths: Massive community knowledge base. JavaScript-based channel development (lower barrier than Java). Strong HL7v2 parsing. Self-hosted (full data control). Free for versions up to 4.5.
Weaknesses: FHIR support requires custom development. No native cloud clustering — HA requires manual configuration. The licensing change for 4.6+ removes the primary cost advantage. Security hardening is your responsibility.
Best for: Teams with 2+ integration engineers, organizations with heavy HL7v2 workloads, health systems that need full control over their integration layer.
Rhapsody (Rhapsody Health)
Enterprise-grade integration engine with a visual development environment. Rhapsody positions itself as the "enterprise Mirth" — more polished, better supported, and significantly more expensive.
Strengths: Visual filter/route designer reduces development time. Built-in FHIR R4 support. Enterprise clustering out of the box. Strong vendor support and training. SOC 2 Type II certified cloud offering.
Weaknesses: Proprietary — you cannot inspect or modify the engine's core. License costs are 2-3x Mirth Commercial. Smaller community means fewer open-source examples and troubleshooting resources.
Best for: Large health systems (500+ beds) with budget for enterprise licensing, organizations that value vendor support over community resources, teams transitioning from HL7v2 to FHIR.
Iguana (iNTERFACEWARE)
Canadian-built integration engine with a Lua scripting environment. Iguana is the dark horse — less known than Mirth or Rhapsody but technically capable and well-regarded by teams that use it.
Strengths: Lua scripting is simpler than Java for non-developer integration analysts. Excellent built-in monitoring dashboard. Strong HL7v2 and FHIR support. Responsive vendor support.
Weaknesses: Smaller ecosystem means fewer pre-built components. Lua expertise is rarer than JavaScript or Java. Less name recognition means harder to hire experienced Iguana engineers.
Best for: Mid-size organizations that want a polished UI without Rhapsody's price tag, teams where the integration analysts are not full-time software developers.
Managed iPaaS (Redox, Health Gorilla, Particle Health)
Cloud-hosted platforms that provide pre-built connectors to major EHR systems. You send data in, they handle the transformation and delivery. The managed iPaaS model trades control for speed.
Strengths: Pre-built Epic, Cerner, athenahealth connectors. Dramatically faster time-to-first-interface (days, not weeks). No infrastructure to manage. Smaller engineering team required.
Weaknesses: Per-interface or per-message pricing becomes expensive at scale. You do not control the transformation logic. Data transits through third-party infrastructure. Vendor lock-in is significant — migrating off a managed iPaaS means rebuilding every interface.
Best for: Digital health startups needing fast EHR connectivity, organizations without dedicated integration engineering teams, use cases with under 20 interfaces.
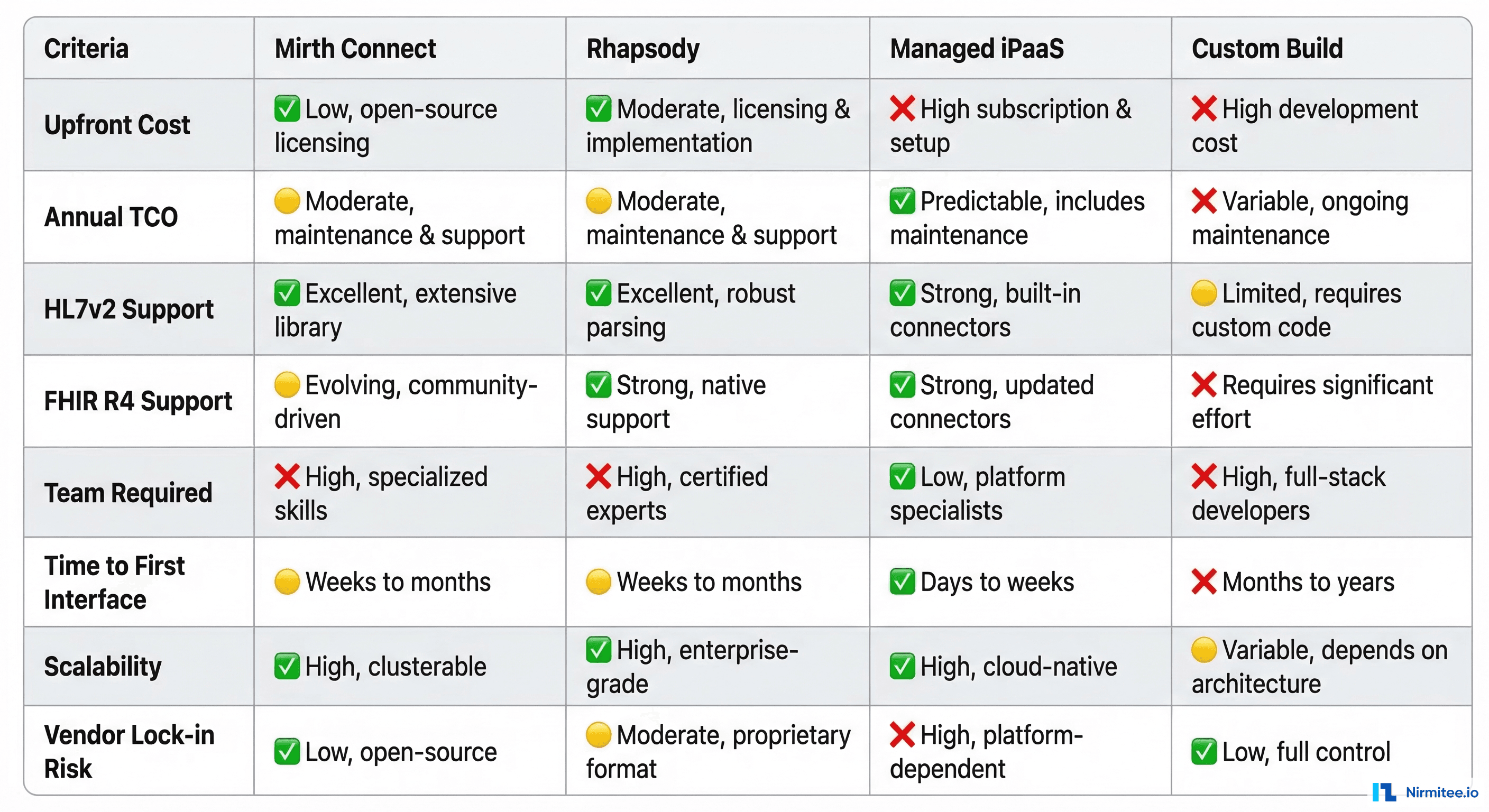
The Build vs. Buy Decision Matrix
Some organizations consider building a custom integration layer. This makes sense in exactly two scenarios:
- You are a health IT vendor building integration as a core product capability (not just connecting your own systems). Your integration layer is a competitive differentiator, not a cost center.
- Your requirements are so specific that no existing platform can meet them without extensive customization — typically involving proprietary protocols, extreme performance requirements, or unique compliance constraints.
For everyone else: buy. The true cost of building and maintaining a healthcare integration engine exceeds the cost of any commercial platform within 18-24 months.
Implementation: The First 90 Days
Regardless of which platform you choose, the first 90 days follow the same pattern:
Days 1-30: Foundation
- Deploy platform in non-production environment
- Establish monitoring and alerting baseline
- Build your first 2-3 interfaces (start with ADT — it touches every downstream system)
- Document your channel naming convention, error handling patterns, and deployment process
Days 31-60: Scale
- Migrate existing point-to-point interfaces to the platform
- Implement HA/DR configuration
- Build automated testing for critical interfaces
- Train the broader team on channel development and troubleshooting
Days 61-90: Operationalize
- Deploy to production
- Establish on-call rotation for integration failures
- Build dashboard showing message volumes, error rates, and latency per interface
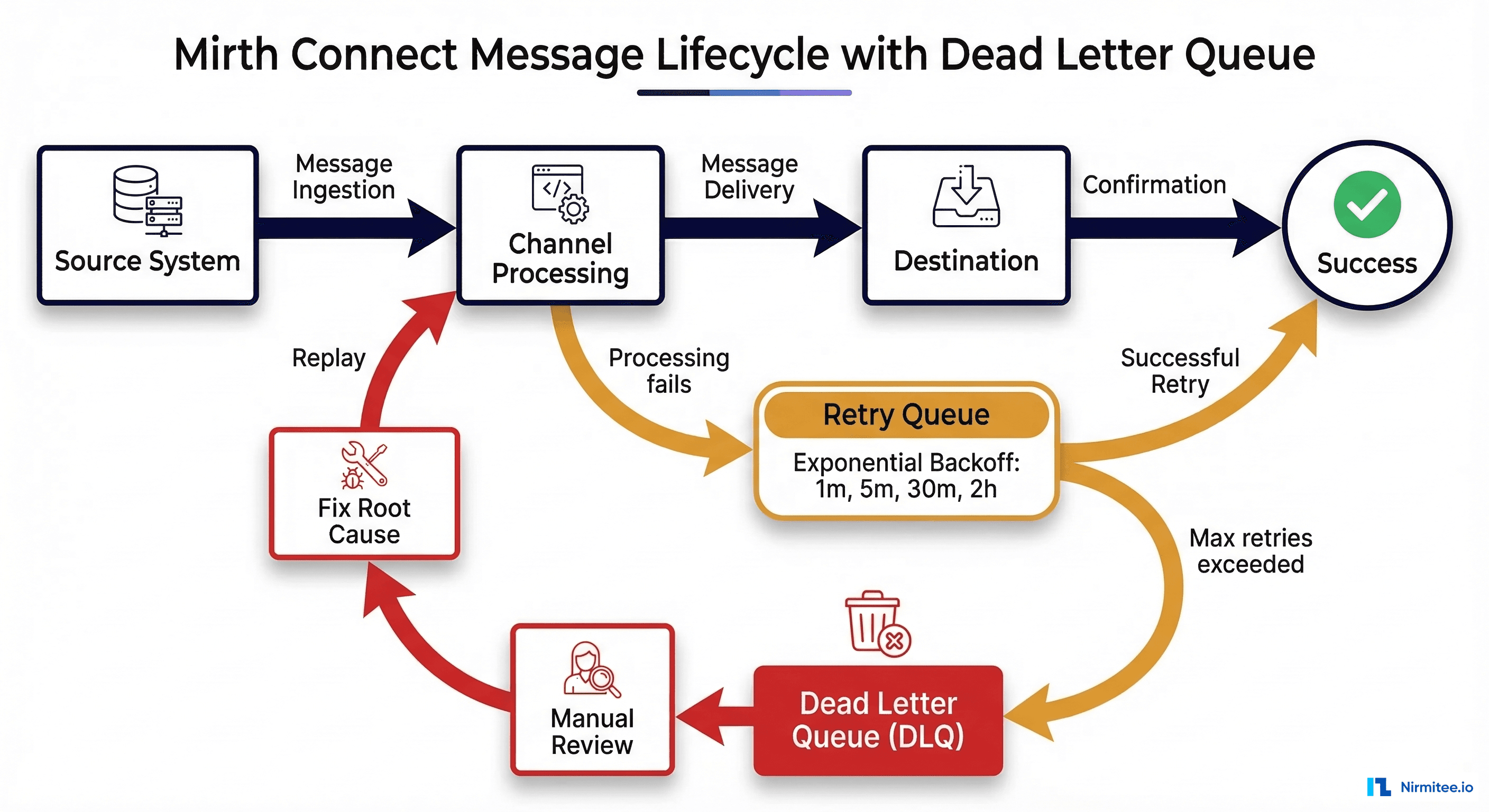
- Create runbooks for the top 10 failure scenarios
The Mistakes We See Most Often
After evaluating integration platforms for dozens of health systems, these are the patterns that predict failure:
Mistake 1: Choosing based on the demo. Every platform demos well with a simple ADT-to-FHIR transformation. Ask to see the platform handle a real-world scenario: a malformed HL7v2 message with missing required segments, a FHIR bundle that exceeds the server's payload limit, a downstream system that is offline for 6 hours. The demo should make you uncomfortable, not impressed.
Mistake 2: Ignoring total cost of ownership. A free open-source engine staffed by three $150K/year engineers costs $450K/year in labor alone. A $200K/year managed iPaaS that needs one engineer at $150K costs $350K. Do the full math before committing.
Mistake 3: Optimizing for today's interface count. You will have 2-3x more interfaces in three years than you have today. Choose a platform that handles your projected scale, not your current state.
Mistake 4: Skipping the implementation planning phase. A platform is not a solution. It is a tool. Without a clear implementation plan — naming conventions, error handling patterns, monitoring strategy, testing approach — even the best platform becomes a mess within 6 months.
Mistake 5: Not evaluating migration cost. Ask every vendor: "What does it cost to leave your platform?" If the answer is "rebuild everything," factor that into your TCO. Platforms with standard export formats (FHIR Bundles, HL7v2 message logs, channel configuration as code) give you an exit path.
Frequently Asked Questions
What is the best healthcare integration platform for a small clinic?
For clinics with under 10 interfaces and no dedicated integration team, a managed iPaaS (Redox or Health Gorilla) provides the fastest path to connectivity. The per-interface cost is higher, but the total cost of ownership is lower because you avoid hiring specialized engineers.
Is Mirth Connect still free after the licensing change?
Mirth Connect versions up to 4.5.x remain open-source under the MPL license. Version 4.6+ requires a commercial license from NextGen Healthcare. The open-source community has forked the 4.5 codebase, but long-term viability of the fork is uncertain. For new deployments in 2026, evaluate the commercial license cost against alternatives.
How long does it take to implement a healthcare integration platform?
Platform deployment takes 2-4 weeks. Building your first production interface takes an additional 4-8 weeks. Migrating 20+ existing interfaces typically takes 6-12 months. The platform selection and procurement process itself averages 3-4 months for organizations that do proper due diligence.
Should we use FHIR for all new integrations?
Use FHIR when the source and destination both support it natively. Do not force FHIR into HL7v2 workflows — you will spend more time on the V2-to-FHIR translation than the integration itself. The practical answer in 2026 is a dual-standard architecture: FHIR for new patient-facing APIs and external partnerships, HL7v2 for internal clinical messaging that already works.
What is the biggest risk in choosing a healthcare integration platform?
Vendor lock-in. Every platform creates dependencies — in channel configurations, transformation logic, monitoring dashboards, and team expertise. The mitigation is keeping your transformation logic as portable as possible: document your mappings independent of the platform, version your configurations in Git, and maintain architecture diagrams that describe the logical integration, not the platform-specific implementation.
Need help evaluating integration platforms for your specific environment? At Nirmitee, we have built and migrated integration layers across Mirth Connect, FHIR-native platforms, and custom architectures for health systems and healthtech companies. Talk to our integration team — we will tell you what we would actually pick for your situation, not what earns us the biggest margin.