A 200-bed community hospital in Ohio was losing $1.82 million per year to appointment no-shows. Their no-show rate sat at 18.2%, consistent with the national average that costs U.S. healthcare $150 billion annually. Their scheduling desk ran six and a half full-time staff handling 220 calls per day, with patients waiting an average of 4.2 minutes on hold before reaching a person. After 5 PM and on weekends, patients who needed to book or reschedule went to voicemail.
In September 2024, they deployed an AI scheduling agent. Within 90 days, their no-show rate dropped to 11.3%. After-hours bookings, previously zero, accounted for 34% of new appointments. Three schedulers were redeployed to patient navigation roles. The annual savings hit $420,000 in recaptured revenue alone, before counting the staff redeployment and overtime elimination.
This is not a complex clinical AI project requiring FDA review, SaMD classification, or months of model validation. Appointment scheduling is the simplest, lowest-risk, highest-ROI entry point for any health system exploring AI agents. This article breaks down exactly how it works, what it costs, and how to replicate the results.

Why Scheduling Is the Ideal First AI Agent
Every health system evaluating AI agents faces the same question: where do we start? The answer is almost always scheduling, and not because it is the most exciting use case. It is because scheduling has six characteristics that make it the perfect proof-of-value deployment.
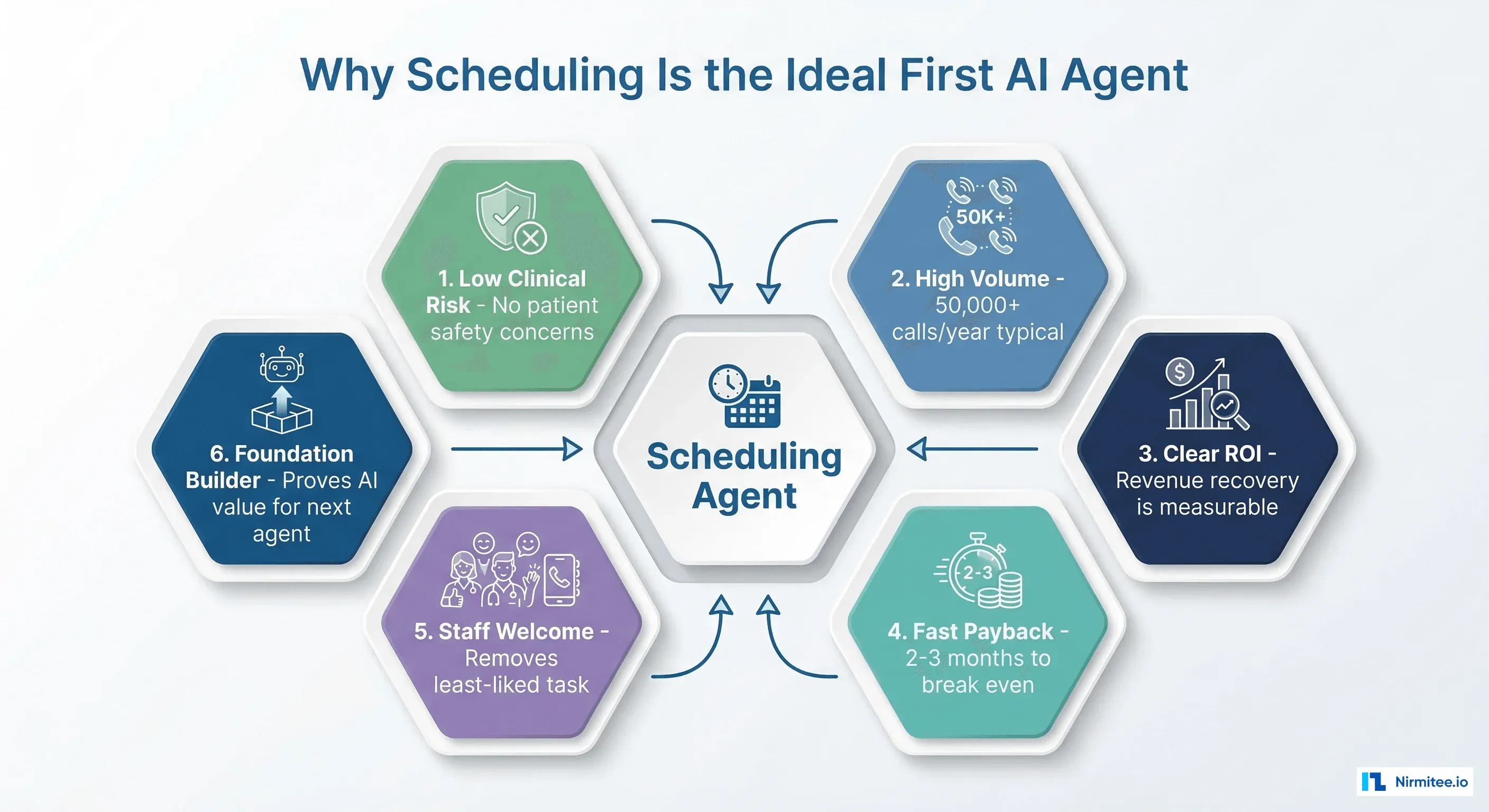
1. Zero Clinical Risk
A scheduling agent does not make clinical decisions. It does not prescribe medications, interpret lab results, or recommend treatments. The worst-case failure mode is a booking error that staff can correct, not a patient safety event. This means no FDA regulatory review, no clinical validation studies, and no medical staff committee approvals before deployment.
2. High Transaction Volume
A 200-bed hospital handles 50,000-80,000 scheduling interactions per year. High volume means small per-transaction savings compound into large annual numbers. AI scheduling solutions are processing hundreds of thousands of transactions across healthcare organizations, giving you confidence in the technology's reliability at scale.
3. Clear, Measurable ROI
No-show rate is a number your CFO already tracks. Revenue per appointment is known. The math is direct: if the agent reduces no-shows by 7 percentage points and each missed appointment costs $200 on average, the savings are $200 x (0.07 x annual appointments). No assumptions about soft benefits or long-term cultural change required.
4. Fast Payback (2-3 Months)
With Year 1 total costs around $121,000 and monthly savings around $35,000, the payback period is under 4 months. Most organizations see payback in 2-3 months because the no-show reduction is immediate. Build the full business case and the numbers speak for themselves.
5. Staff Welcome the Change
Phone scheduling is consistently rated the least satisfying task by healthcare administrative staff. The AI agent handles the repetitive calls (booking, rescheduling, cancellations) while staff handle complex cases (multi-provider coordination, insurance disputes, patient complaints). Adoption resistance is minimal because the agent takes work nobody wants.
6. Proves AI Value for the Next Agent
Success with a scheduling agent gives your organization the data, confidence, and executive support to deploy the next agent. The patient journey has six more stages where AI agents deliver measurable ROI. Scheduling is the foundation.
How the Scheduling Agent Works
The agent handles five core workflows that cover 85-90% of scheduling interactions:
Workflow 1: Inbound Appointment Booking
Patient calls or sends a text. The agent identifies the patient (date of birth, last name, or patient ID), determines the visit type (new patient, follow-up, specific complaint), checks provider availability in real time, and books the optimal slot. The entire interaction takes 1.5-2.5 minutes, compared to 6-9 minutes with a human scheduler.
Workflow 2: Insurance Verification
Before confirming the appointment, the agent performs a real-time eligibility check through the clearinghouse API. It verifies coverage is active, checks whether the selected provider is in-network, and confirms whether the visit type requires a referral or prior authorization. Automated insurance verification saves an average of 12 minutes per verification compared to manual phone calls to payers.
Workflow 3: Cancellation and Waitlist Management
When a patient cancels, the agent immediately identifies patients on the waitlist who match the open slot (same provider, same visit type, available at that time). It contacts waitlisted patients by text or phone, and the first to confirm gets the slot. This fills 40-60% of cancellation slots that would otherwise go empty.
Workflow 4: Intelligent Reminders
Standard reminder systems send the same message to every patient. The scheduling agent sends risk-adjusted reminders based on the patient's historical no-show probability. High-risk patients get earlier reminders (7 days, 3 days, 1 day, same morning), confirmation requests, and transportation assistance offers. Low-risk patients get a single day-before reminder. This targeted approach reduces no-shows by 35% compared to flat reminder systems.
Workflow 5: After-Hours Booking
The agent operates 24/7. Patients who call at 9 PM, on Saturday, or during lunch breaks can book appointments immediately instead of leaving voicemails. 34% of AI-scheduled appointments are now booked outside traditional business hours, representing entirely new scheduling capacity at zero marginal labor cost.

Technical Architecture
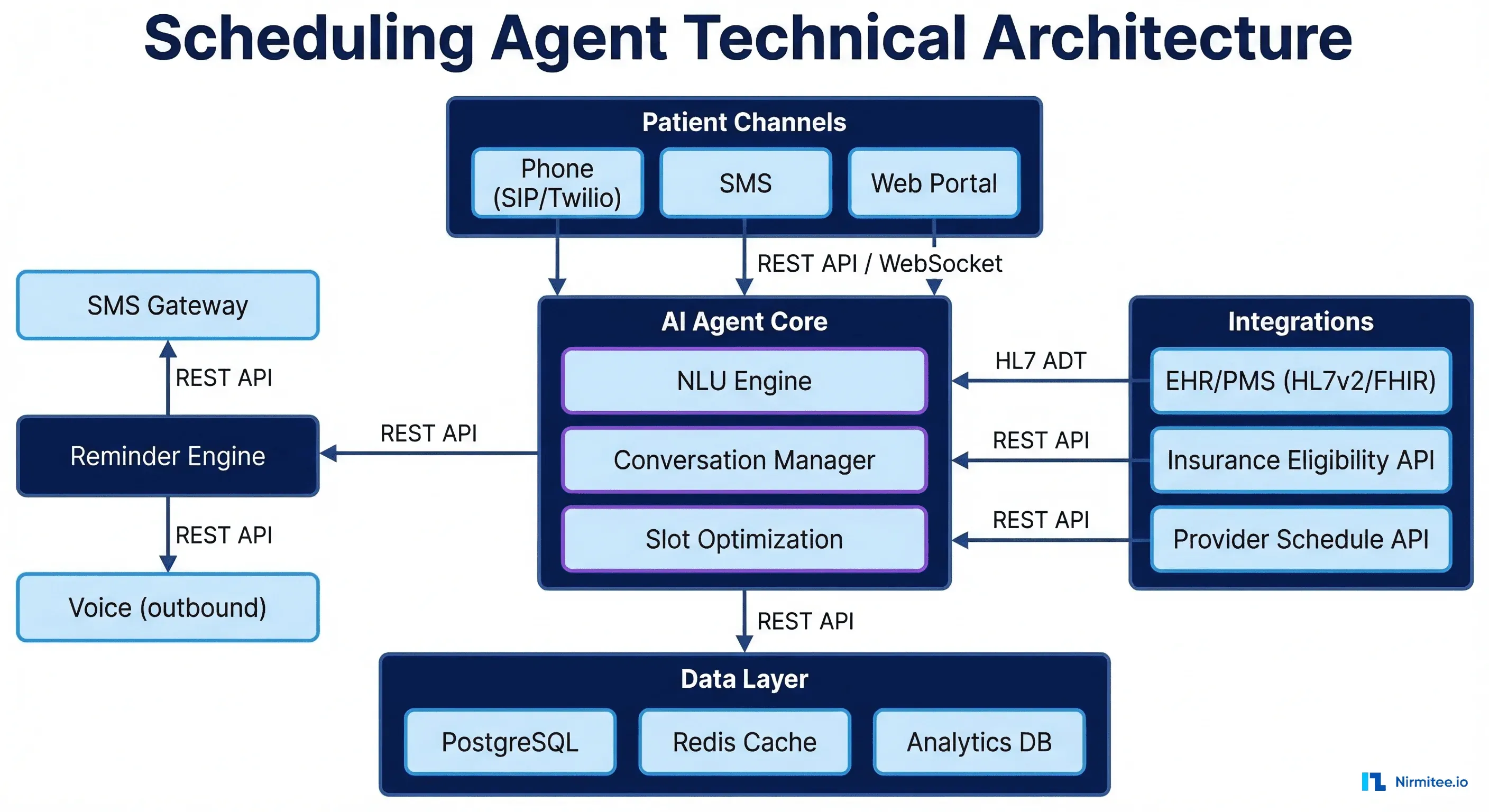
The scheduling agent integrates with your existing systems. It does not replace your EHR, practice management system, or phone system. It sits alongside them.
Core Components
| Component | Technology | Purpose |
|---|---|---|
| Voice Channel | Twilio / Amazon Connect | Inbound/outbound voice with SIP trunking |
| NLU Engine | GPT-4 / Claude | Natural language understanding for patient intent |
| Conversation Manager | Custom orchestrator | Multi-turn dialog flow, context tracking |
| EHR Integration | HL7v2 ADT / FHIR Appointment | Provider schedule read, appointment create/update |
| Eligibility API | Availity / Change Healthcare | Real-time insurance verification (270/271) |
| Reminder Engine | Event-driven (NATS/Redis) | Risk-adjusted outbound reminders |
| Analytics | PostgreSQL + dashboard | No-show tracking, utilization, ROI measurement |
EHR Integration Pattern
# Simplified scheduling agent EHR integration
import httpx
from datetime import datetime, timedelta
class SchedulingAgent:
def __init__(self, fhir_base_url: str, auth_token: str):
self.fhir = httpx.Client(
base_url=fhir_base_url,
headers={"Authorization": f"Bearer {auth_token}"}
)
def find_available_slots(self, provider_id: str, visit_type: str,
date_range_days: int = 14) -> list:
"""Query FHIR Slot resources for provider availability."""
start = datetime.now().isoformat()
end = (datetime.now() + timedelta(days=date_range_days)).isoformat()
response = self.fhir.get("/Slot", params={
"schedule.actor": f"Practitioner/{provider_id}",
"start": f"ge{start}",
"start": f"le{end}",
"status": "free",
"service-type": visit_type,
})
bundle = response.json()
return [entry["resource"] for entry in bundle.get("entry", [])]
def book_appointment(self, patient_id: str, slot_id: str,
reason: str) -> dict:
"""Create a FHIR Appointment resource."""
appointment = {
"resourceType": "Appointment",
"status": "booked",
"slot": [{"reference": f"Slot/{slot_id}"}],
"participant": [
{"actor": {"reference": f"Patient/{patient_id}"},
"status": "accepted"},
],
"reasonCode": [{"text": reason}],
}
response = self.fhir.post("/Appointment", json=appointment)
return response.json()Detailed Cost Breakdown
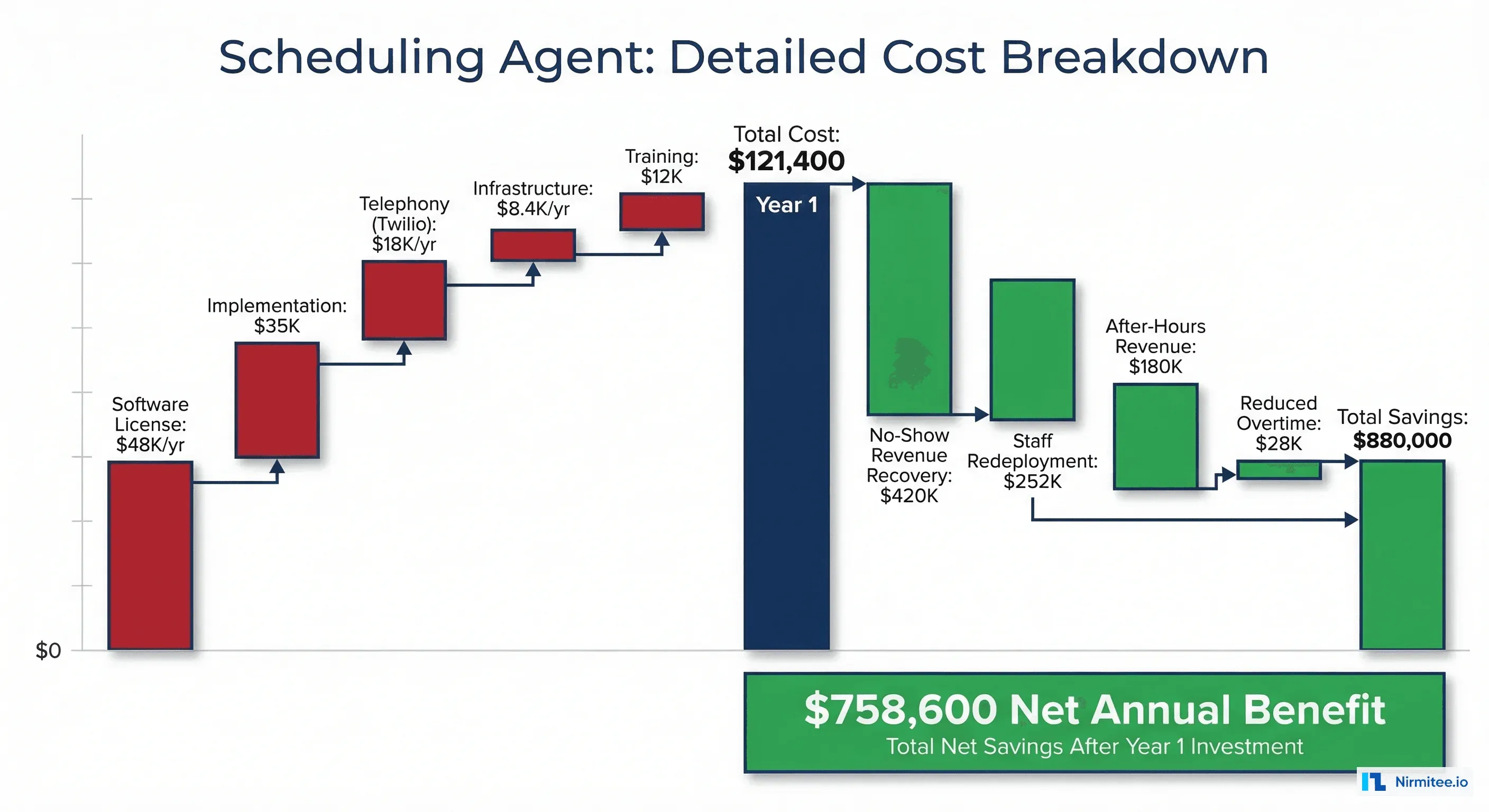
Every number here is based on actual deployment costs at a 200-bed community hospital. Your numbers will vary based on EHR vendor, call volume, and integration complexity.
Year 1 Costs
| Line Item | Type | Annual Cost |
|---|---|---|
| AI agent platform license | Recurring | $48,000 |
| Implementation and configuration | One-time | $35,000 |
| Telephony (Twilio voice + SMS) | Recurring | $18,000 |
| Cloud infrastructure | Recurring | $8,400 |
| Staff training | One-time | $12,000 |
| Year 1 Total | $121,400 | |
| Year 2+ Total | Recurring only | $74,400 |
Annual Savings
| Savings Category | Calculation | Annual Value |
|---|---|---|
| No-show revenue recovery | 6.9% reduction x 55,000 appts x $110 avg | $417,450 |
| Staff redeployment | 3.5 FTEs x $72,000 fully loaded | $252,000 |
| After-hours new revenue | 34% of bookings x new patient value | $180,000 |
| Overtime elimination | Removed peak-hour overflow staffing | $28,000 |
| Waitlist fill rate | 40% of cancellations filled (was 5%) | $96,000 |
| Total Annual Savings | $973,450 |
Year 1 net benefit: $973,450 - $121,400 = $852,050
Year 1 ROI: 702%
Payback period: $121,400 / ($973,450 / 12) = 1.5 months
Implementation Timeline: 12 Weeks to Production
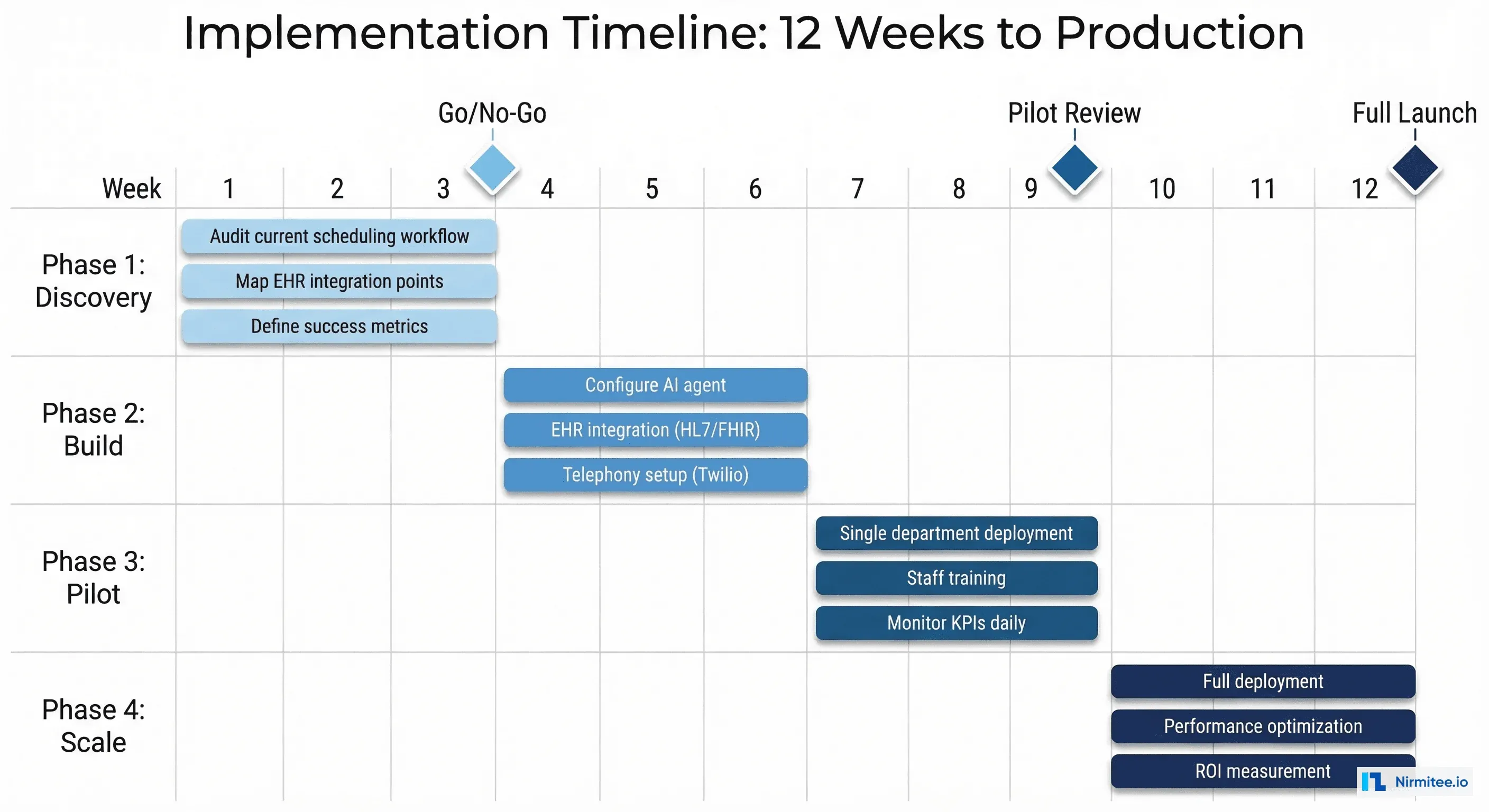
Weeks 1-3: Discovery
- Audit current scheduling workflow: call volumes, peak hours, common call types, current no-show rate
- Map EHR integration points: which scheduling APIs are available, what data format (HL7v2 or FHIR)
- Define success metrics: target no-show rate, target after-hours booking rate, staff redeployment plan
- Get stakeholder sign-off: operations, clinical leadership, IT, and finance
Weeks 4-6: Build
- Configure AI agent conversation flows for top 5 scheduling scenarios
- Integrate with EHR scheduling API (read provider availability, write appointments)
- Set up telephony: inbound routing, outbound reminder infrastructure
- Build the no-show prediction model using 12 months of historical appointment data
- Integrate eligibility verification with clearinghouse
Weeks 7-9: Pilot
- Deploy to one department (typically primary care or orthopedics, highest volume)
- Run AI agent alongside existing staff (patients can press 0 for human at any time)
- Train scheduling staff on exception handling and escalation process
- Monitor daily: call completion rate, booking accuracy, patient satisfaction, escalation rate
Weeks 10-12: Full Deployment
- Roll out to all departments based on pilot learnings
- Enable after-hours autonomous mode (no staff backup required)
- Activate waitlist management and intelligent reminder engine
- Present 30-day results to leadership with ROI comparison to baseline
What Can Go Wrong (and How to Prevent It)
Risk 1: Patients Hate Talking to a Bot
Prevention: The agent must sound natural, not robotic. Modern voice AI (powered by models like GPT-4o) produces natural conversation that most patients do not identify as AI. More importantly, 24/7 availability and zero hold time consistently produce higher satisfaction scores than human-only scheduling in hospital deployment surveys. Always provide a "press 0 for staff" escape hatch.
Risk 2: EHR Integration Fails
Prevention: Validate the EHR scheduling API during discovery (Week 1-3). The most common failure point is that the EHR's scheduling API does not expose real-time slot availability or requires custom middleware. Identify this early and budget for integration engineering. EHR integration is solvable but must be scoped correctly.
Risk 3: Staff See the Agent as a Threat
Prevention: Frame the deployment as staff augmentation, not replacement. Redeployed schedulers move to patient navigation, care coordination, or complex scheduling roles that are more fulfilling and harder to fill externally. Involve scheduling staff in agent design and testing so they have ownership of the outcome.
Risk 4: No-Show Rate Does Not Improve
Prevention: No-shows are driven by multiple factors, not just reminders. The agent must address root causes: difficulty rescheduling (agent makes it effortless), transportation barriers (agent offers telehealth alternative), and forgetfulness (risk-adjusted reminder cadence). If the no-show rate does not improve after 30 days, audit which patient segments are still no-showing and why.
Measuring Success
Track these KPIs weekly from day one of the pilot:
| KPI | Baseline | 30-Day Target | 90-Day Target |
|---|---|---|---|
| No-show rate | 18.2% | 15% | 11-12% |
| Call completion rate | N/A | 80% | 90% |
| Average booking time | 8.5 min | 3 min | 2 min |
| After-hours bookings | 0% | 20% | 34% |
| Patient satisfaction (CSAT) | 72% | 75% | 82% |
| Escalation to human rate | N/A | 25% | 12% |
| Cancellation slot fill rate | 5% | 25% | 40% |
What Comes After Scheduling
Once the scheduling agent proves value, the natural next steps follow the patient journey:
- Month 4-6: Add intake automation, extending the pre-visit workflow the scheduling agent already starts
- Month 6-9: Add post-discharge follow-up, leveraging the same voice/text channels
- Month 9-12: Add prior authorization automation for the highest dollar savings
- Year 2: Clinical decision support and chronic disease management agents
Each subsequent agent is easier to deploy because the infrastructure (telephony, EHR integration, analytics, change management processes) is already in place from the scheduling deployment.
Getting Started
If your health system's no-show rate is above 10%, you are leaving money on the table that an AI scheduling agent can recapture within 90 days. The investment is modest ($121,000 Year 1), the risk is minimal (no clinical decisions involved), and the payback is fast (under 3 months).
At Nirmitee, we build and deploy scheduling agents for health systems of all sizes. From 50-bed community hospitals to multi-site health systems, our team handles the EHR integration, voice AI configuration, and analytics setup so your scheduling agent is live in 12 weeks or less.