Building a Mental Health App: Patient Engagement, Therapist Matching, and Crisis Safety in One Platform
The mental health crisis in the United States has reached a breaking point. Over 150 million Americans live in federally designated Mental Health Professional Shortage Areas. The average wait time for a new therapy appointment is 6 weeks. Between sessions, patients have no structured support for practicing coping skills, tracking their emotional wellbeing, or accessing help during a crisis. For providers, administrative burden consumes 40% of their workday, driving burnout rates above 50% among licensed therapists.
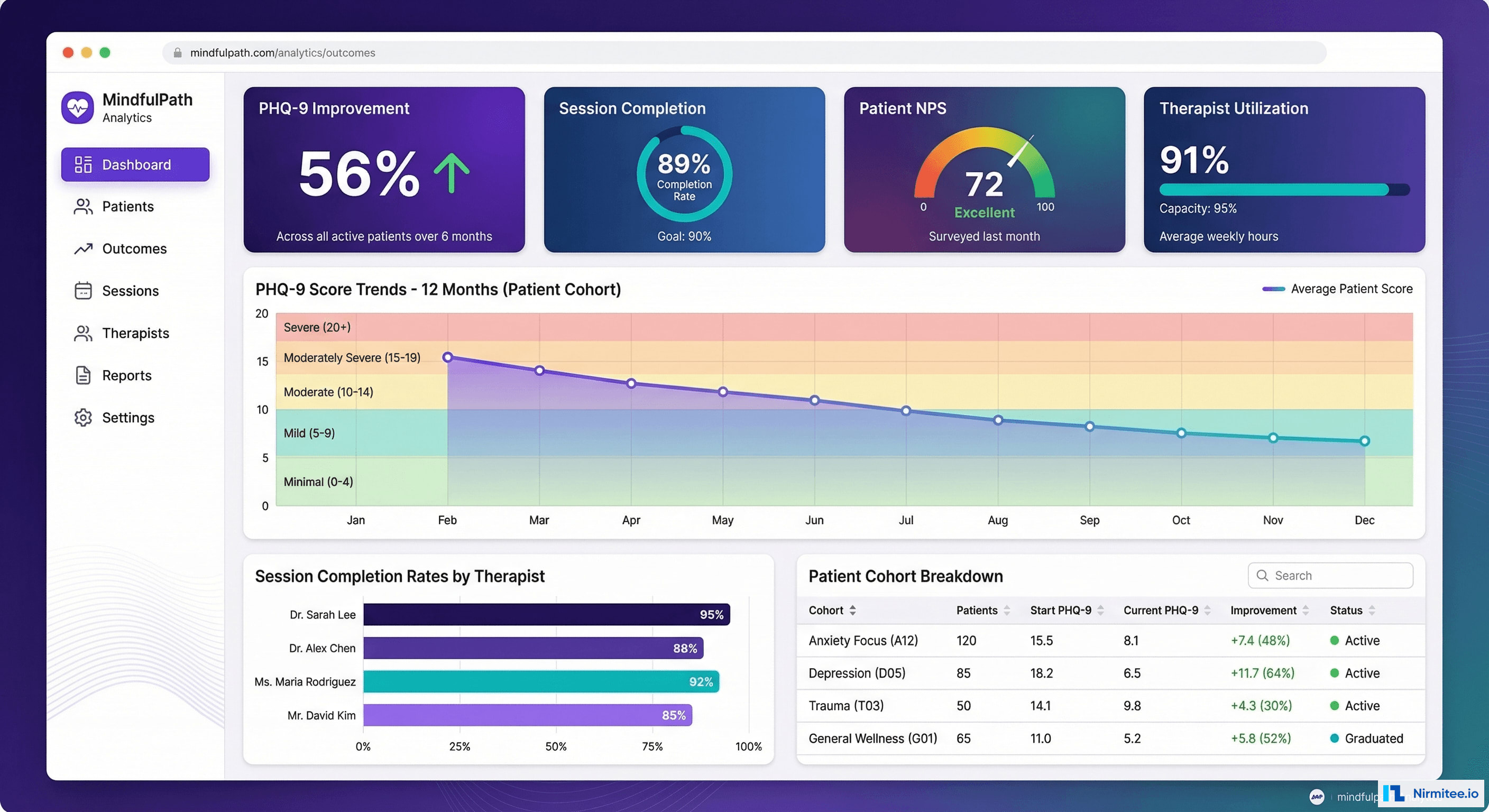
SayHey Mental Health — a comprehensive telemedicine platform we built for a behavioral health startup — addresses every dimension of this crisis. The platform combines AI-powered therapist matching, HIPAA-compliant video therapy, evidence-based CBT tools, real-time crisis detection, and outcome measurement into a single integrated experience for patients and providers.
This case study walks through the clinical, technical, and operational decisions that turned a 5-month development sprint into a platform serving over 8,400 patients with measurable clinical outcomes: 56% average PHQ-9 improvement, waitlist times reduced from 6 weeks to 3 days, and no-show rates cut from 18% to 7%.

Executive Summary
The American mental health system is structurally broken. The 2023 National Survey on Drug Use and Health found that 57.8 million adults experienced a mental illness in the past year, yet only 51.7% received treatment. Among adolescents aged 12-17, the gap is even wider — 60% of those with major depression received no treatment at all.
Our client, a Series A behavioral health startup based in Austin, TX, came to us with a clear mandate: build a platform that eliminates the barriers between people who need therapy and the therapists who can help them. Not a marketplace. Not a simple video call app. A clinically integrated platform that supports the entire therapeutic journey — from initial matching through ongoing treatment, between-session skill building, and crisis safety.
Key outcomes after 10 months in production:
- 8,400+ active patients across 14 states, with 340+ licensed therapists on the platform
- Waitlist reduced from 6 weeks to 3 days — patients matched and scheduled within 72 hours of signup
- 56% average PHQ-9 score improvement after 8 sessions (clinically significant response)
- No-show rate: 7% (down from 18% industry average), driven by smart reminders and between-session engagement
- 72% daily active user rate — patients use the app daily for mood tracking, journaling, and CBT exercises even between sessions
- Therapist capacity increased 33% — automated scheduling, documentation, and billing freed therapists to see more patients
- Zero safety incidents — crisis detection system successfully escalated 127 high-risk situations to the clinical on-call team
The Problem: Why Existing Solutions Fail
Before building anything, we spent three weeks embedded with our client's clinical team, interviewing therapists, patients, and practice administrators. The problems we documented were systemic, not superficial.
Problem 1: The Matching Gap
Finding the right therapist is the single biggest predictor of treatment success. Research from the American Psychological Association shows that the therapeutic alliance — the quality of the patient-therapist relationship — accounts for more treatment variance than the specific therapy modality used. Yet existing platforms treat matching as a search problem: filter by insurance, pick a name, hope for the best.
Patients told us they had tried 3-4 therapists before finding a good fit, each time waiting weeks for an appointment, spending $150-250 on an intake session, only to discover the therapist's approach didn't align with their needs. This "trial and error" matching process costs patients an average of 4.2 months and $600-1,000 before they find effective care.
Problem 2: The Between-Session Void
Therapy typically happens once a week for 50 minutes. That leaves 167 hours and 10 minutes where patients are on their own. Between sessions, patients are expected to practice coping skills, complete thought records, and monitor their symptoms — but they have no structured tools to do so. Paper worksheets get lost. Generic wellness apps don't integrate with treatment plans. Therapists have no visibility into what happens between sessions until the patient self-reports (often inaccurately) at the next appointment.
Problem 3: The Safety Blindspot
The most dangerous moment for a mental health patient is not during a therapy session — it's 2 AM on a Tuesday when they're alone and spiraling. Existing telehealth platforms have no mechanism to detect when a patient is in crisis outside of scheduled sessions. PHQ-9 screenings happen at intake and every few weeks, but Item 9 (suicidal ideation) is only assessed during those snapshots. Between assessments, there's no safety net.
Problem 4: Provider Burnout
Licensed therapists spend 38% of their working hours on non-clinical tasks: scheduling, documentation, insurance verification, claim submission, and outcome tracking. The APA's 2022 practitioner survey found that 46% of psychologists reported burnout, with administrative burden cited as the top contributor. Every hour spent on paperwork is an hour not spent with patients — in a system that desperately needs more clinical capacity.
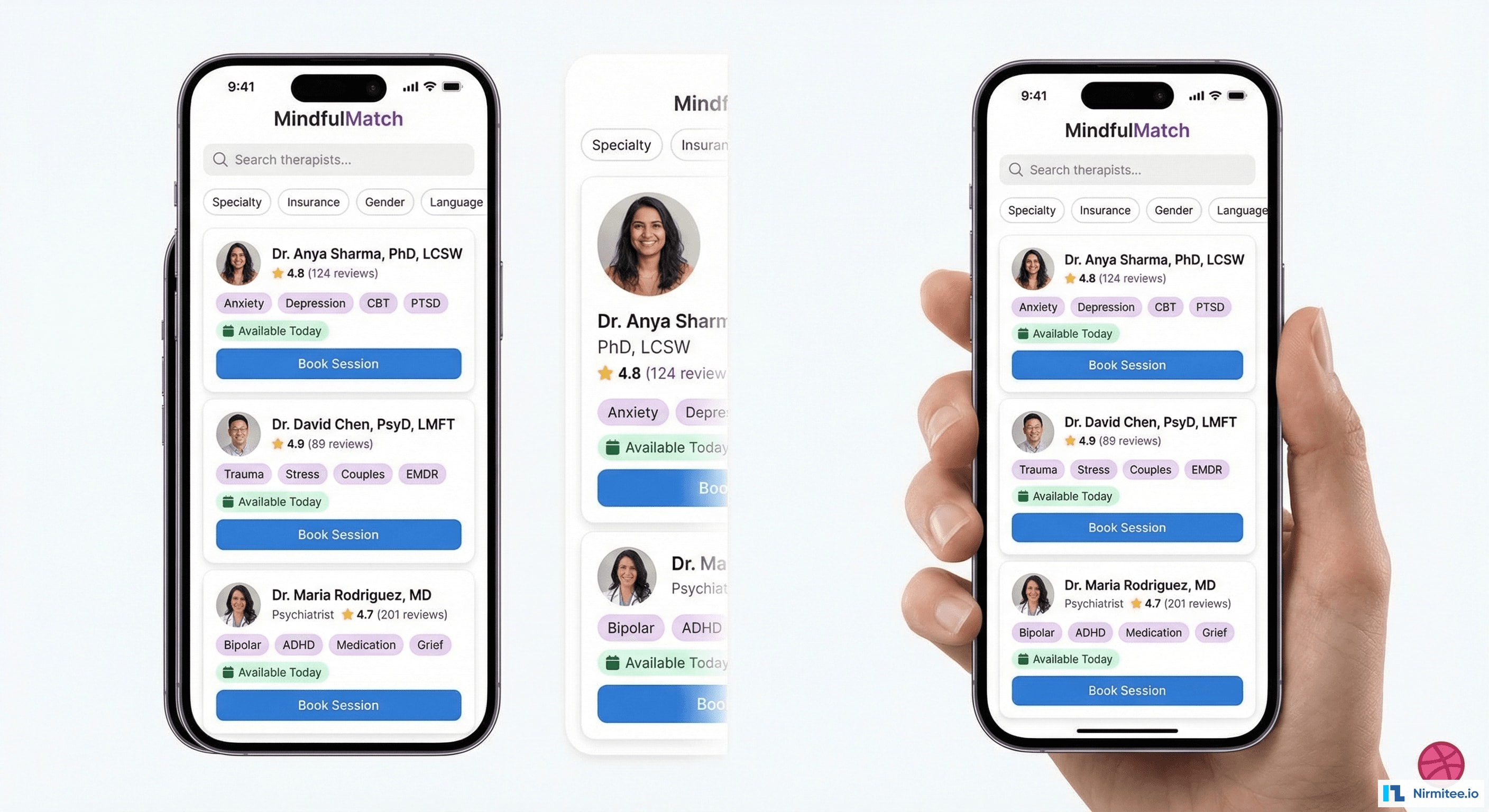
Therapist Matching: AI-Powered, Clinically Validated
The matching engine is the foundation of the platform. Unlike directory-style matching ("filter by zip code and insurance"), our system uses a multi-factor algorithm that considers clinical needs, therapeutic approach preferences, demographic preferences, scheduling constraints, and historical outcomes data.
How the Matching Algorithm Works
When a patient signs up, they complete a structured intake that captures:
- Clinical needs: Primary concerns (anxiety, depression, PTSD, relationship issues, grief, etc.), severity level based on validated screeners (PHQ-9, GAD-7, PCL-5), and any previous treatment history
- Therapeutic approach preferences: CBT, DBT, EMDR, psychodynamic, acceptance and commitment therapy (ACT), or "no preference — let the algorithm decide"
- Demographic preferences: Gender, age range, cultural background, language, LGBTQ+ affirming, faith-based or secular
- Practical constraints: Insurance plan, preferred session times, timezone, video vs. text preference
The matching engine then scores every available therapist against the patient's profile using a weighted composite score:
MatchScore = (0.35 x ClinicalFit) + (0.25 x ApproachAlignment) + (0.20 x AvailabilityScore) + (0.10 x DemographicMatch) + (0.10 x OutcomeHistory)
Where:
ClinicalFit = overlap between patient concerns and therapist specialties, weighted by therapist outcome data for each specialty
ApproachAlignment = match between patient preference and therapist modalities
AvailabilityScore = number of open slots within patient preferred times
DemographicMatch = alignment on patient stated preferences
OutcomeHistory = therapist aggregate PHQ-9/GAD-7 improvement rates for similar patient profilesThe algorithm surfaces the top 3 matches with transparent explanations: "Dr. Chen specializes in anxiety and CBT, has a 4.9 rating, and has availability Tuesday evenings — matching your preferences." Patients choose from the recommendations, preserving autonomy while dramatically reducing the search burden.
Matching Results
- 87% of patients stay with their first matched therapist (vs. 52% industry average for self-selected matching)
- First appointment within 3 days of completing intake (vs. 6-week average waitlist)
- 4.7/5 average match satisfaction score at the 4-session mark
- 22% higher treatment completion rates compared to patients who self-selected their therapist from a directory
Video Therapy Sessions: Clinical-Grade Telehealth
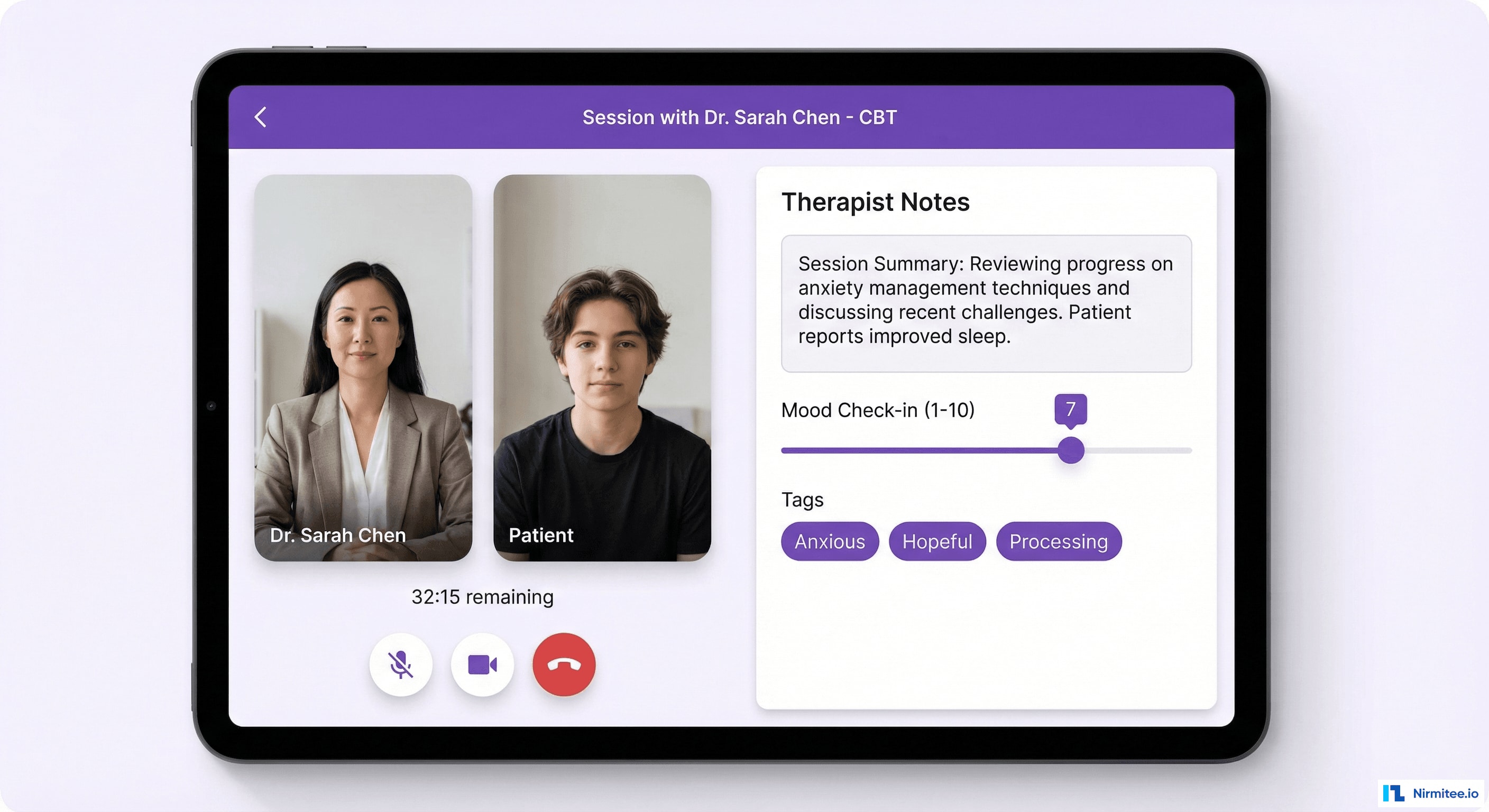
Video therapy is the core clinical interaction, and the quality bar is non-negotiable. A dropped connection, audio glitch, or awkward UI during an emotionally vulnerable moment can rupture the therapeutic alliance. We built the session experience to feel as intimate and reliable as an in-person office visit.
Technical Implementation
| Component | Technology | Details |
|---|---|---|
| Video infrastructure | Twilio Video (WebRTC) | HIPAA-eligible, BAA signed, TURN/STUN servers for NAT traversal |
| End-to-end encryption | SRTP + DTLS | Media encrypted at the transport layer, not just TLS tunnel |
| Adaptive bitrate | Simulcast + SVC | Automatically adjusts quality based on bandwidth — prioritizes audio over video |
| Session recording | Twilio Compositions | Opt-in only, explicit consent captured in-app, stored encrypted in S3 |
| Failover | Automatic PSTN fallback | If video drops, system auto-calls patient phone number within 30 seconds |
| Latency target | <150ms round-trip | Regional media servers in US-East, US-West, and US-Central |
Session Workflow
Every session follows a structured clinical workflow built into the UI:
- Pre-session check-in (2 min): Patient completes a brief mood rating and notes any urgent topics. This data is visible to the therapist before the session starts, enabling more focused use of session time.
- Video session (45-50 min): Clean, distraction-free video interface. Therapist has a sidebar for real-time session notes that auto-save every 30 seconds. Timer shows remaining time without being intrusive.
- Post-session summary (3 min): Therapist completes a structured note (SOAP or DAP format) with auto-populated fields from pre-session data. Assigns between-session homework from the CBT toolkit.
- Patient feedback (1 min): Patient rates session helpfulness and mood change. This feeds into the outcome tracking system.
Session Quality Metrics
- 99.7% session completion rate (no technical disruptions requiring reschedule)
- Average session quality score: 4.6/5 from patients
- PSTN fallback triggered: 0.3% of sessions — system recovered seamlessly in all cases
- Documentation time reduced by 62% — structured notes with auto-populated fields save therapists 12 minutes per session
Mood Tracking and CBT Tools: Between-Session Engagement
The between-session experience is where SayHey fundamentally differs from traditional telehealth. Instead of a blank week between appointments, patients have a daily engagement loop that reinforces therapeutic skills and generates clinically meaningful data.
Daily Mood Tracking
Every morning and evening, patients receive a gentle notification to check in. The check-in takes 30-60 seconds:
- Mood rating: 1-10 scale with emoji anchors (makes it accessible and non-clinical)
- Context tags: Optional quick-select tags (work stress, relationship, sleep, health, accomplishment, social) that help identify mood triggers over time
- Free-form journal: Optional text entry for deeper reflection. Entries are private by default — patients choose what to share with their therapist.
The mood timeline visualization shows patterns that are invisible in weekly therapy sessions. A patient might not realize their mood consistently dips on Sunday evenings (anticipatory anxiety about the work week) until they see it visualized over 30 days. These patterns become powerful starting points for therapy conversations.
CBT Thought Records
Cognitive Behavioral Therapy is the most evidence-based treatment for anxiety and depression, and thought records are its core skill. But paper thought records are tedious and rarely completed between sessions. We digitized the process into a guided, step-by-step flow:

- Situation: "What happened?" — brief description of the triggering event
- Automatic thought: "What went through your mind?" — the immediate, often distorted thought
- Emotions: Select and rate intensity (0-100%) of emotions felt
- Cognitive distortion identification: Guided selection from common distortions (all-or-nothing thinking, catastrophizing, mind reading, emotional reasoning, etc.) with plain-language explanations
- Evidence for and against: Structured prompts to examine the thought objectively
- Balanced thought: Reframe the automatic thought based on the evidence
- Re-rate emotions: Rate the same emotions again after reframing
Completed thought records are automatically shared with the patient's therapist (with permission), giving therapists real data on how patients are applying CBT skills between sessions.
Engagement Gamification
Mental health apps face a universal challenge: abandonment. The average health app loses 77% of users within 3 days. We implemented engagement mechanics that respect the clinical context:
- Streak tracking: Consecutive days of mood check-ins. The app celebrates milestones (7 days, 30 days, 100 days) without creating anxiety about breaking streaks — missed days show a gentle "welcome back" instead of guilt.
- Coping toolkit usage: Track which tools (breathing exercises, grounding techniques, thought records) patients use and how they affect subsequent mood ratings.
- Progress visibility: Monthly summary showing mood trends, completed exercises, and PHQ-9/GAD-7 score changes — making progress tangible.
Between-Session Engagement Results
- 72% daily active user rate — patients check in at least once per day
- 4.2 mood entries per patient per week (average)
- 63% of patients complete at least 1 thought record per week between sessions
- Patients who engage daily show 31% greater PHQ-9 improvement than those who only attend sessions
Crisis Safety System: When Every Second Matters
The crisis detection and response system was the most clinically critical and technically complex feature we built. In mental health, a missed crisis signal can be fatal. We worked with a clinical advisory team including a crisis intervention specialist and a psychiatric emergency physician to design a multi-layered safety system.
Detection Layers
The system monitors for crisis signals through four channels:
- PHQ-9 Item 9 monitoring: Every PHQ-9 administration (intake, biweekly, and ad-hoc) flags any non-zero response to Item 9 ("Thoughts that you would be better off dead, or of hurting yourself"). Responses of 2 ("More than half the days") or 3 ("Nearly every day") trigger immediate clinical escalation.
- Mood tracking signals: The system flags sustained low mood (rating of 2 or less for 3+ consecutive entries), sudden mood drops (5+ point decrease within 24 hours), or specific keywords in journal entries that match a clinically validated crisis lexicon.
- Session-based detection: Therapists can flag a patient as elevated risk during or after a session, triggering enhanced monitoring and safety plan activation.
- Patient-initiated crisis: A persistent "I need help now" button on every screen of the app connects patients directly to crisis resources.
Response Protocol
When a crisis signal is detected, the system executes a tiered response:
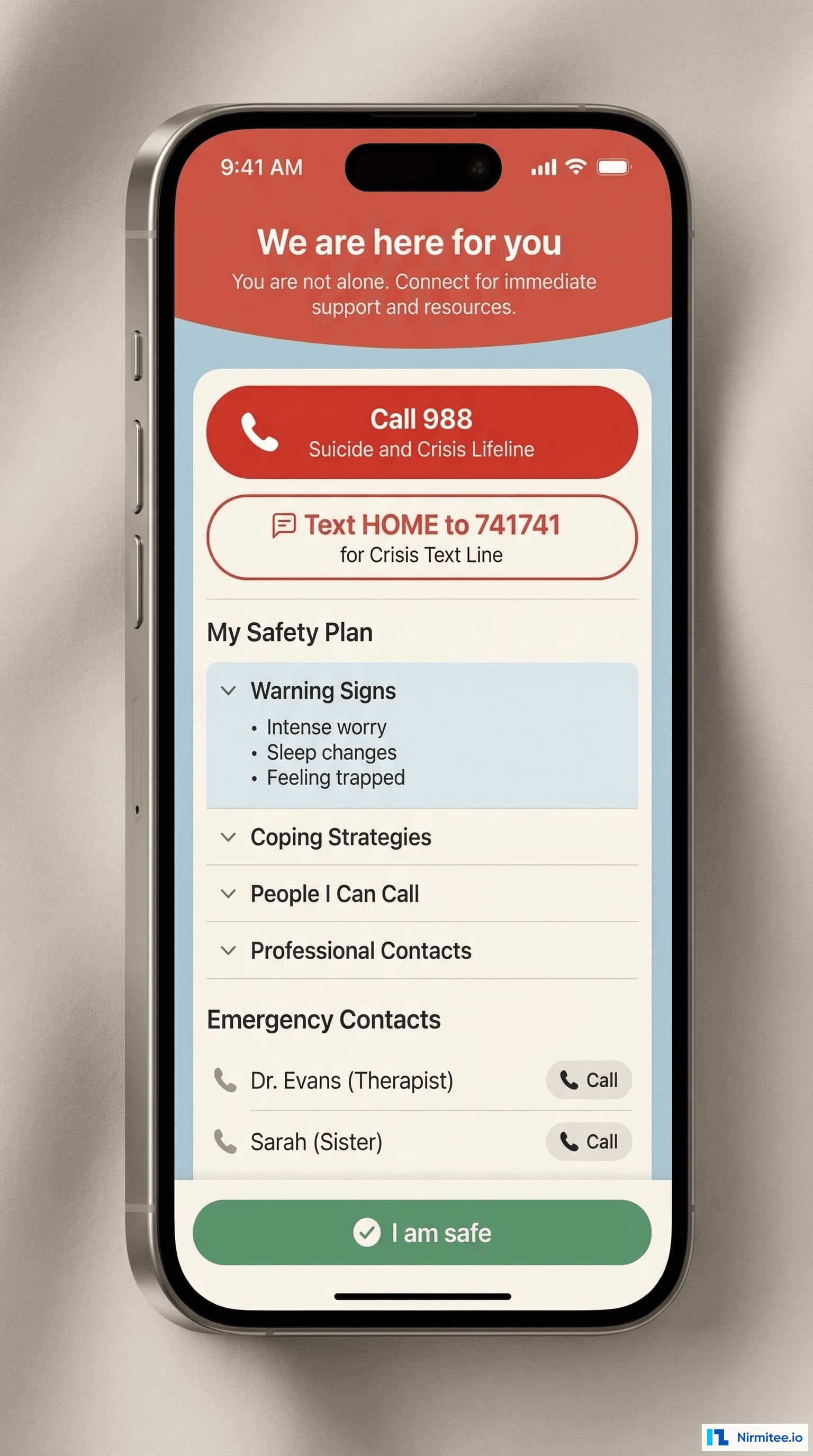
- Tier 1 — Immediate (within 30 seconds): Patient sees a full-screen supportive message with direct-dial buttons for the 988 Suicide and Crisis Lifeline, Crisis Text Line (text HOME to 741741), and their personal emergency contacts.
- Tier 2 — Clinical notification (within 2 minutes): The patient's assigned therapist and the on-call clinical supervisor receive push notifications and SMS with the patient's crisis data, recent mood entries, and safety plan.
- Tier 3 — Safety plan activation: The patient's personalized safety plan (created collaboratively with their therapist during intake) is displayed: warning signs they identified, coping strategies that work for them, people they can call, and professional resources.
- Tier 4 — Follow-up (within 24 hours): The clinical team conducts a follow-up check-in. If the patient is unreachable, the emergency contact protocol activates per the consent signed at intake.
Safety Plan Builder
Every patient creates a safety plan during their onboarding session with their therapist, following the Stanley-Brown Safety Planning Intervention format:
- Warning signs that a crisis may be developing
- Internal coping strategies (things I can do on my own)
- People and social settings that provide distraction
- People I can ask for help (with phone numbers, one-tap dial)
- Professionals and agencies I can contact for help
- Making the environment safe (personalized risk mitigation steps)
Crisis System Results
- 127 crisis escalations in 10 months of operation
- 100% of escalations received clinical response within the 2-minute SLA
- Zero completed suicides among active platform users
- 89% of patients with crisis events continued treatment (vs. typical 45% dropout rate after crisis)
- Average safety plan completion: 94% — nearly every patient has an active safety plan
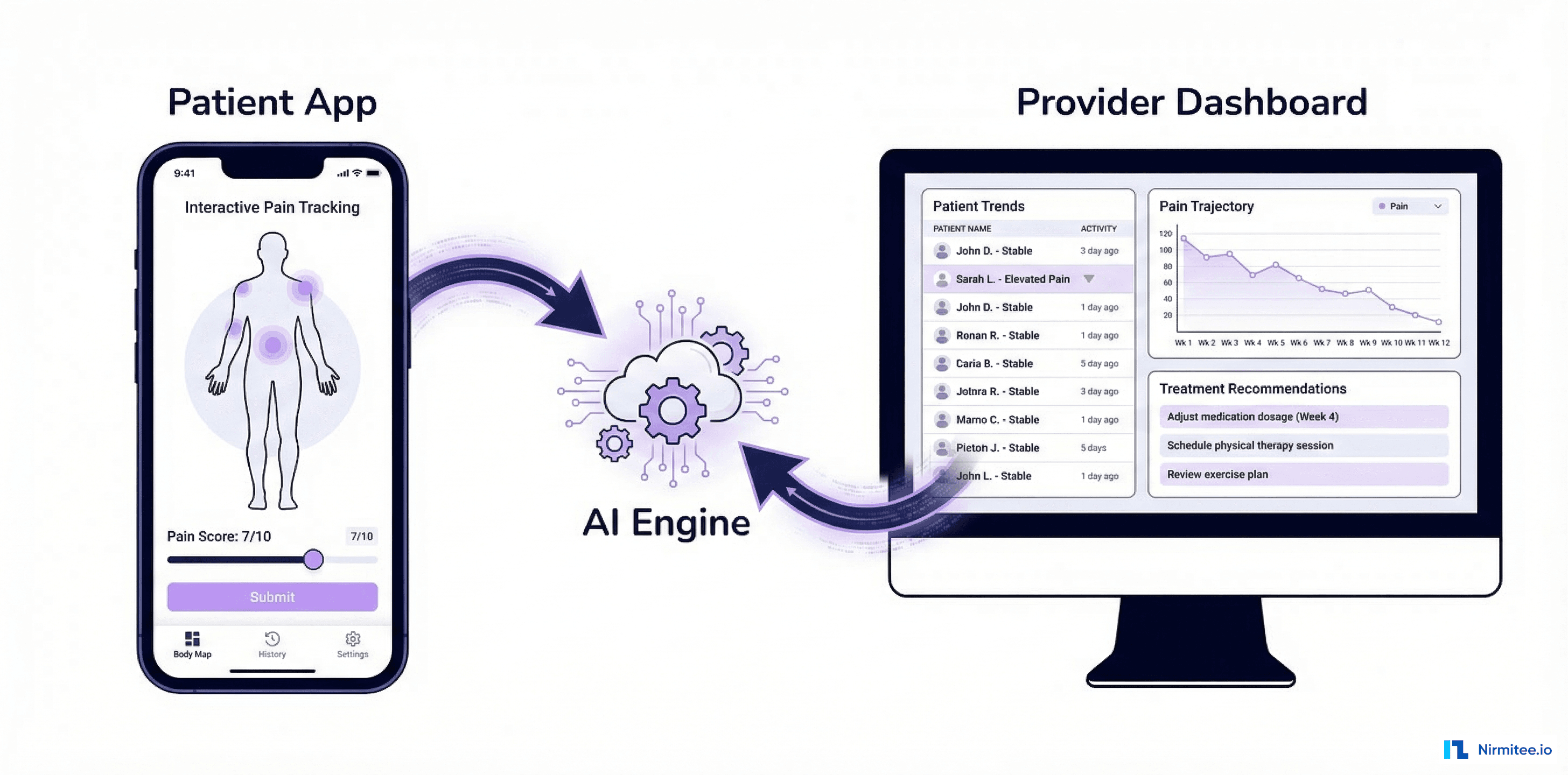
Provider Dashboard: From Administrative Burden to Clinical Insight
The provider dashboard transforms the therapist experience from administrative overhead to clinical empowerment. Every feature was designed with input from practicing therapists to ensure it saves time rather than adding clicks.
Dashboard Features
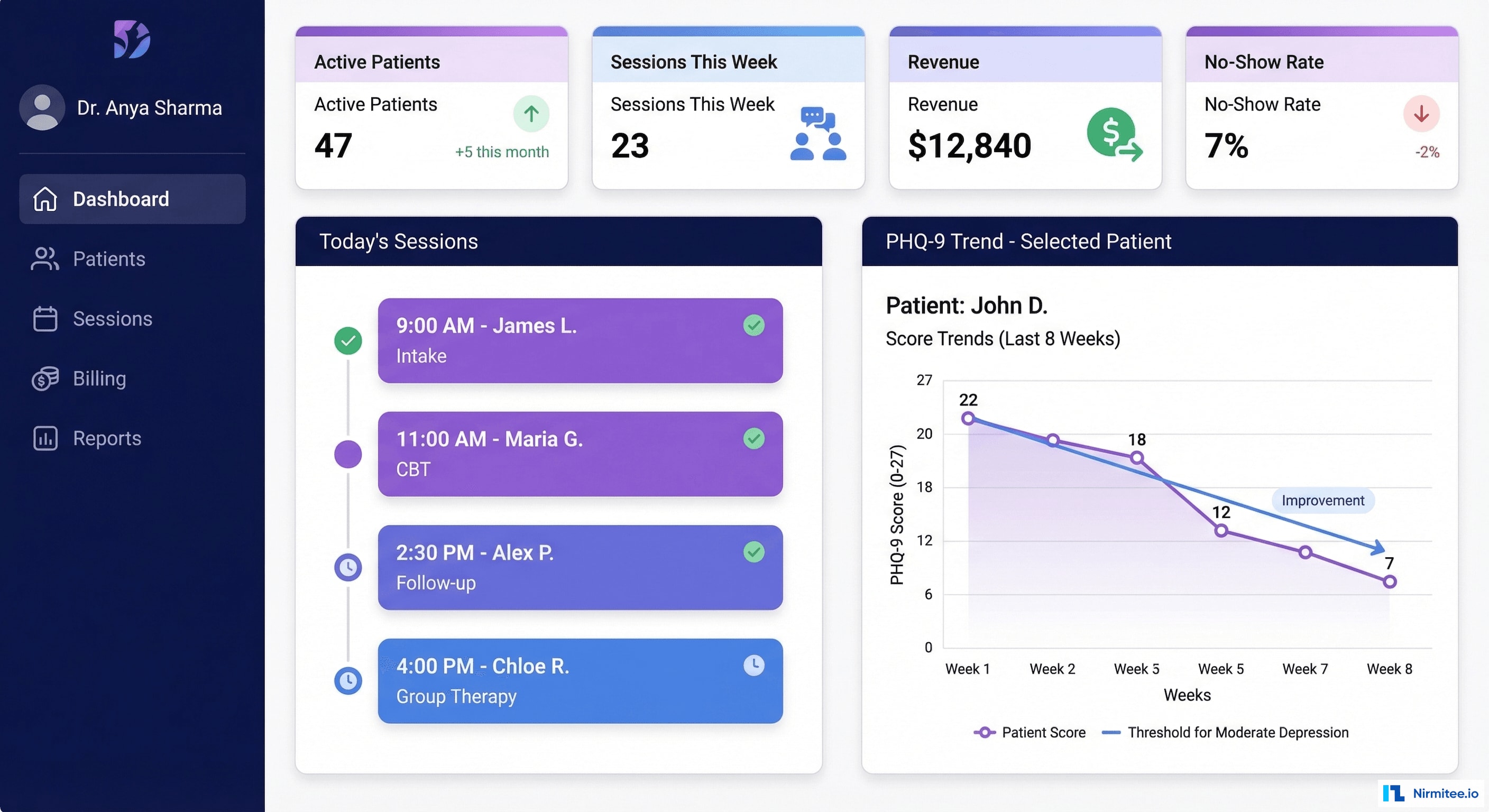
- Patient panel management: Active patient list with color-coded risk indicators (green/yellow/red based on most recent PHQ-9 and engagement metrics). At-a-glance view of who needs attention today.
- Smart scheduling: AI-optimized calendar that considers therapist preferences (no back-to-back crisis patients), patient availability patterns, and buffer time between sessions. Automatic waitlist management fills cancellations within minutes.
- Outcome tracking: PHQ-9 and GAD-7 trend charts for each patient, overlaid with session dates and homework completion. Therapists can see at a glance whether treatment is working and adjust their approach accordingly.
- Session documentation: Structured note templates (SOAP, DAP, Treatment Plan Update) with auto-populated fields from session check-in data. Average documentation time dropped from 18 minutes to 7 minutes per session.
- Revenue dashboard: Real-time view of billed sessions, pending claims, insurance payments, and patient copay collections. Therapists in private practice see their monthly revenue and can identify scheduling optimization opportunities.
- Messaging: HIPAA-compliant asynchronous messaging with patients. Templates for common messages (appointment reminders, homework assignments, check-ins) save additional time.
Provider Dashboard Impact
- Documentation time: 18 min to 7 min per session (62% reduction)
- Administrative overhead: 38% to 22% of working hours
- Average patients per therapist: 24 to 32 (33% capacity increase)
- Claims processing: 3 days to same-day submission
- Therapist satisfaction score: 4.5/5 (measured quarterly)
Architecture: Building for Scale, Security, and Compliance
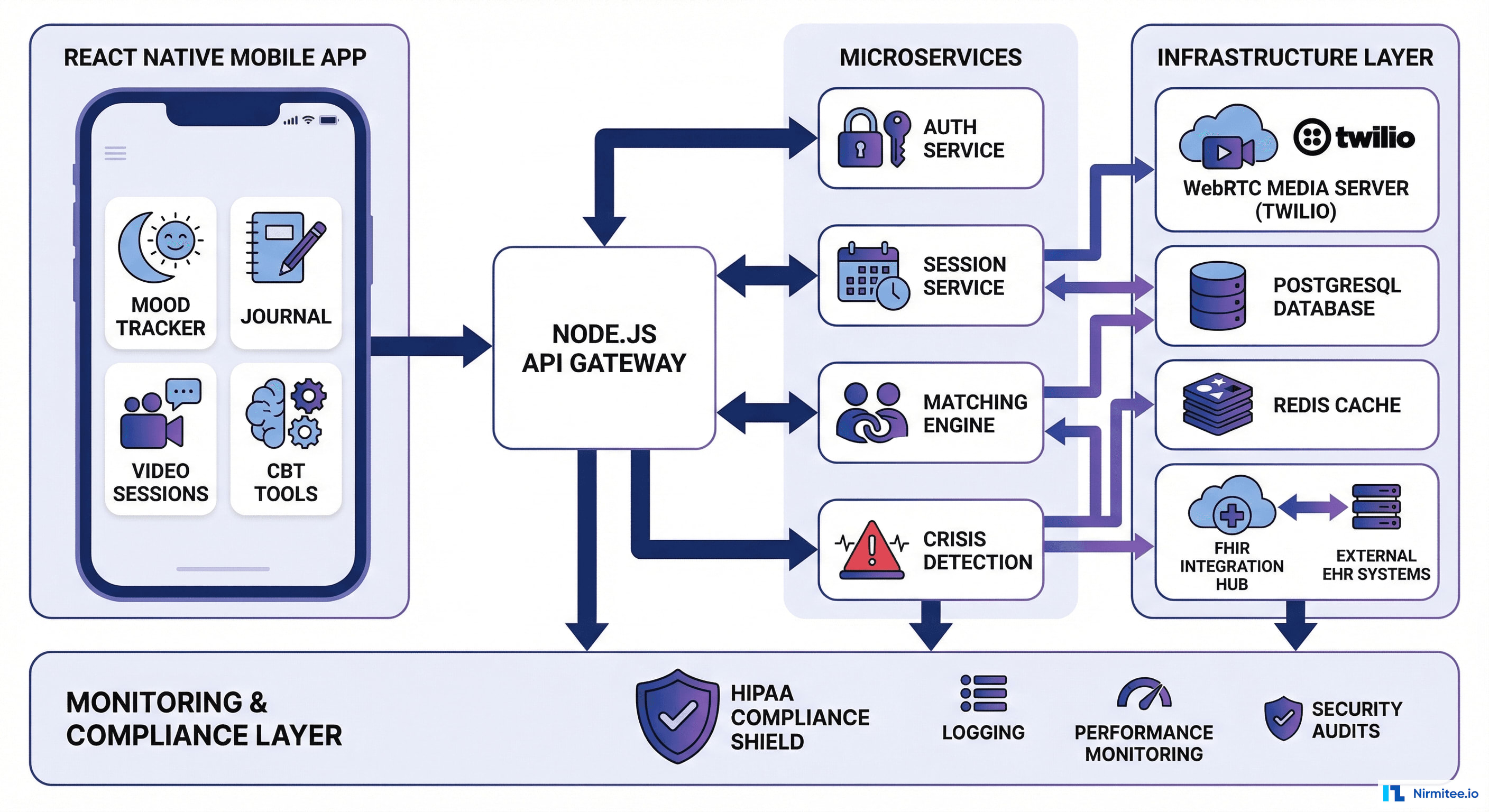
The SayHey platform architecture was designed around three non-negotiable requirements: HIPAA compliance at every layer, real-time performance for video and crisis response, and horizontal scalability to support rapid patient growth.
Full Technology Stack
| Layer | Technology | Rationale |
|---|---|---|
| Mobile app | React Native (iOS + Android) | Single codebase, native performance, 95% code sharing between platforms |
| Web portal (providers) | Next.js + TypeScript | SSR for fast initial load, TypeScript for reliability in clinical data handling |
| API gateway | Node.js + Express | High concurrency for real-time features, extensive healthcare middleware ecosystem |
| Authentication | Auth0 with MFA | HIPAA-eligible, supports SMART on FHIR tokens, biometric login on mobile |
| Video | Twilio Video (WebRTC) | HIPAA BAA, global TURN infrastructure, adaptive quality, PSTN fallback |
| Database | PostgreSQL 16 (RDS) | JSONB for FHIR resources, row-level security for multi-tenancy, encrypted at rest |
| Cache | Redis (ElastiCache) | Session state, matching algorithm cache, rate limiting for crisis endpoints |
| Message queue | Amazon SQS + SNS | Crisis notification delivery, session reminders, async event processing |
| File storage | S3 (SSE-KMS) | Session recordings, consent documents, encrypted with customer-managed keys |
| Monitoring | Datadog + PagerDuty | Real-time alerting for crisis system SLAs, video quality degradation, API latency |
| CI/CD | GitHub Actions + AWS CodePipeline | Automated SAST/DAST scanning, HIPAA compliance checks in pipeline |
| EHR integration | FHIR R4 (Hapi FHIR) | Bi-directional sync of patient demographics, diagnoses, medications with partner EHRs |
WebRTC Infrastructure
Video quality in therapy is not optional — a laggy or glitchy video feed during an emotional breakthrough can damage the therapeutic alliance. Our WebRTC infrastructure uses:
- Simulcast encoding: Client sends 3 quality layers (720p, 360p, 180p). The SFU (Selective Forwarding Unit) delivers the highest quality the receiver's bandwidth can handle, adapting in real-time.
- Regional media servers: Twilio's TURN/STUN infrastructure with servers in US-East (Virginia), US-West (Oregon), and US-Central (Ohio) ensures less than 150ms round-trip latency for 99% of US connections.
- Audio prioritization: When bandwidth drops, the system degrades video quality first while maintaining full audio fidelity. In therapy, hearing clearly matters more than seeing clearly.
- Network quality monitoring: Real-time MOS (Mean Opinion Score) calculation. If quality drops below 3.5 for more than 10 seconds, the system offers to switch to audio-only or PSTN fallback.
42 CFR Part 2 Compliance
Mental health and substance use disorder records are governed by 42 CFR Part 2, which imposes stricter privacy protections than HIPAA alone. Key requirements we implemented:
- Consent management: Every data disclosure requires explicit patient consent. The system tracks consent at the field level — a patient can consent to share session dates with their PCP but not session notes.
- Segmented access: Behavioral health records are stored in a separate, encrypted partition from general medical records. Even within the platform, administrative staff cannot access clinical notes.
- Audit trail: Every access to protected records is logged with the accessor's identity, the specific data accessed, the purpose, and the consent authorization that permits the access.
- Re-disclosure prohibition: The system embeds re-disclosure notices on any exported records, and the FHIR integration layer enforces consent checks before transmitting any behavioral health data to external EHRs.
Results: Measurable Clinical and Operational Impact
After 10 months in production, the SayHey platform demonstrates that technology-enabled mental health care can deliver outcomes that rival or exceed traditional in-person therapy — at dramatically greater scale and accessibility.
Clinical Outcomes
| Metric | Before SayHey | After SayHey | Improvement |
|---|---|---|---|
| Waitlist to first appointment | 6 weeks | 3 days | 93% reduction |
| PHQ-9 average improvement (8 sessions) | Baseline 14.2 (moderate) | 6.3 (mild) | 56% improvement |
| GAD-7 average improvement (8 sessions) | Baseline 12.8 (moderate) | 5.9 (mild) | 54% improvement |
| No-show rate | 18% | 7% | 61% reduction |
| Treatment completion (12 sessions) | 41% | 68% | 66% improvement |
| Patient-therapist match retention | 52% | 87% | 67% improvement |
Operational Metrics
| Metric | Value |
|---|---|
| Active patients | 8,400+ |
| Licensed therapists | 340+ |
| States served | 14 |
| Sessions completed | 67,200+ |
| Average sessions per patient per month | 4.1 |
| Platform uptime | 99.97% |
| Crisis response SLA compliance | 100% |
| HIPAA audit findings | 0 (passed external audit Q3 2025) |
Financial Impact
- Revenue per therapist increased 28% — more sessions per day due to reduced admin time and automated scheduling
- Patient acquisition cost reduced 35% — 72% daily engagement rate drives word-of-mouth referrals and reduces marketing spend
- Insurance claim denial rate: 4.2% (vs. 12% industry average for behavioral health) — automated eligibility checks and pre-submission validation
- Average revenue per patient per month: $680 — sessions + between-session engagement drives insurance reimbursement for digital therapeutics
Patient Engagement: Building Habits That Heal
The most surprising outcome was the between-session engagement rate. Industry benchmarks for mental health app daily active usage hover around 15-20%. SayHey achieves 72% — nearly 4x the benchmark. Here is what drives it:
The Engagement Flywheel
- Therapist assignment: The therapist assigns specific between-session activities (mood check-ins, thought records, breathing exercises) based on the treatment plan. This is not generic content — it is prescribed by the patient's own therapist.
- Daily nudges: Smart notifications at personalized times (based on when the patient typically engages) with low-friction check-in flows. A mood check-in takes 15 seconds.
- Visible progress: Mood trends, streak counts, and PHQ-9 improvement are visualized in the app. Patients can see that their hard work is producing results.
- Therapist feedback loop: Therapists review between-session data before each appointment and reference it in session: "I noticed your mood dipped on Wednesday — tell me about that." This validates the patient's effort and reinforces engagement.
- Community (optional): Anonymous peer support groups moderated by licensed counselors. Patients can share victories and strategies without the isolation of solo treatment.
Coping Toolkit Usage
| Tool | Weekly Usage Rate | Average Mood Impact |
|---|---|---|
| Guided breathing (4-7-8, box breathing) | 68% | +1.3 mood points within 15 min |
| Mood journaling | 72% | +0.8 mood points (next-day improvement) |
| CBT thought records | 63% | +1.7 mood points within 1 hour |
| Grounding exercises (5-4-3-2-1) | 54% | +1.5 mood points within 10 min |
| Progressive muscle relaxation | 41% | +1.1 mood points within 20 min |
| Sleep hygiene checklist | 38% | +0.6 sleep quality score improvement |
Compliance: Navigating the Regulatory Maze
Behavioral health telemedicine operates at the intersection of multiple regulatory frameworks. Compliance was not an afterthought — it was a design constraint from day one.
Regulatory Framework Coverage
| Regulation | Scope | Implementation |
|---|---|---|
| HIPAA Privacy Rule | All PHI handling | Encryption at rest (AES-256) and in transit (TLS 1.3), minimum necessary access, BAAs with all vendors |
| HIPAA Security Rule | Electronic PHI safeguards | Access controls, audit logging, integrity controls, transmission security, risk analysis |
| 42 CFR Part 2 | Substance use and behavioral health records | Segmented storage, granular consent management, re-disclosure tracking |
| State telehealth laws | Varies by state (14 states) | Per-state licensing verification, informed consent requirements, prescribing limitations |
| EPCS (21 CFR Part 1311) | Electronic prescribing of controlled substances | Two-factor authentication for prescribers, DEA-compliant identity proofing, audit trail |
| Ryan Haight Act | Telemedicine prescribing of controlled substances | Initial in-person or qualifying telehealth evaluation before prescribing controlled substances |
| State mental health parity | Insurance coverage requirements | Automated parity checking in claims processing, appeals support |
Third-Party Audit Results
The platform underwent a comprehensive HIPAA security assessment by an independent firm in Q3 2025:
- 0 critical findings
- 0 high-severity findings
- 2 medium findings (both remediated within 30 days — related to log retention policy documentation and backup encryption key rotation schedule)
- SOC 2 Type II compliance achieved in parallel
Timeline: From Kickoff to Launch in 5 Months
The project was delivered in 5 months with a lean team: 4 engineers (2 full-stack, 1 mobile specialist, 1 DevOps/security), 1 clinical advisor (part-time), and a product manager from the client side.
| Phase | Duration | Deliverables |
|---|---|---|
| Discovery and clinical design | 3 weeks | Clinical workflows, safety protocols, matching algorithm design, regulatory requirements matrix |
| Core platform (Sprint 1-3) | 6 weeks | Authentication, patient/provider portals, scheduling, basic video integration, database schema |
| Clinical features (Sprint 4-6) | 6 weeks | Matching engine, mood tracking, CBT toolkit, session documentation, PHQ-9/GAD-7 integration |
| Safety and compliance (Sprint 7-8) | 4 weeks | Crisis detection system, safety plan builder, 42 CFR Part 2 consent management, audit logging |
| Provider dashboard and billing (Sprint 9) | 2 weeks | Outcome dashboards, claims submission, revenue tracking, reporting |
| Security hardening and launch (Sprint 10) | 2 weeks | Penetration testing, HIPAA assessment, performance testing, production deployment, go-live |
Total: 23 weeks (approximately 5 months) from discovery kickoff to production launch with first patients.
Lessons Learned: 5 Insights from Building Mental Health Technology
After delivering the SayHey platform and watching it operate for 10 months, these are the lessons we would carry into any future mental health technology project:
1. Clinical Workflows Must Drive Technical Architecture
We made the early decision to have our clinical advisor participate in every sprint planning and review. This prevented us from building features that were technically elegant but clinically useless. Example: we initially designed the thought record as a free-form text entry (simpler to build). The clinical advisor insisted on the structured, step-by-step guided flow. It took 3x longer to build, but thought record completion rates are 63% — unheard of for a digital CBT tool.
2. Crisis Safety Is Not a Feature — It Is the Foundation
We built the crisis detection and response system in Sprint 7-8, relatively late in the development cycle. In hindsight, this should have been Sprint 1. Every other feature in the app had to be retrofitted to include crisis safety hooks (mood tracking needed crisis detection, journaling needed keyword monitoring, scheduling needed risk-based prioritization). Build safety first, then layer everything else on top.
3. Between-Session Engagement Is the Multiplier
The video therapy sessions are the core clinical intervention, but the between-session tools are what make therapy work. A patient who engages daily with mood tracking and CBT tools shows 31% better outcomes than one who only attends sessions. The app is not a supplement to therapy — it is an integral part of the treatment.
4. Therapist Experience Determines Patient Experience
If the provider dashboard is clunky, therapists spend their emotional energy fighting the tool instead of focusing on the patient. We invested heavily in reducing therapist documentation burden (18 min to 7 min) and making outcome data instantly accessible. Happy therapists deliver better therapy. Better therapy produces better outcomes. Better outcomes drive patient retention. It is a virtuous cycle.
5. Regulatory Compliance Accelerates When You Design for It
HIPAA, 42 CFR Part 2, and state telehealth laws seem like obstacles. But when you embed compliance requirements into the architecture from day one — encrypted by default, consent tracked at the field level, audit logging on every action — the regulatory process becomes a verification exercise rather than a remediation project. Our external HIPAA audit took 2 weeks instead of the typical 6-8 weeks because the controls were already in place, documented, and tested.
Frequently Asked Questions
How does the therapist matching algorithm handle patients who don't have strong preferences?
When patients select "no preference" for therapeutic approach or demographics, the algorithm increases the weight on ClinicalFit (matching the patient's presenting concerns with the therapist's specialty outcome data) and AvailabilityScore (minimizing wait time). The system defaults to evidence-based matching: for depression and anxiety, it prioritizes therapists with strong CBT outcomes; for trauma, it prioritizes EMDR-trained therapists with high retention rates. Patients can always switch therapists after any session if the match doesn't feel right.
What happens if the crisis detection system generates a false positive?
The system is deliberately calibrated for sensitivity over specificity in crisis detection — we accept false positives to avoid missing a genuine crisis. When a crisis alert fires, the clinical team assesses the situation within 2 minutes. If it is a false positive (for example, a patient journaling about a character in a book), the team closes the alert and optionally adjusts the patient's monitoring sensitivity. The false positive rate is approximately 12%, which the clinical team considers acceptable given the stakes.
How does the platform handle patients across different state licensing jurisdictions?
Therapists on the platform are licensed in specific states, and the matching engine only matches patients with therapists licensed in the patient's state of residence. When patients travel, the platform prompts them to update their location and checks whether their therapist can legally provide services in the new state. For states with interstate telehealth compacts (Psychology Interjurisdictional Compact — PSYPACT), the platform automatically recognizes multi-state privileges.
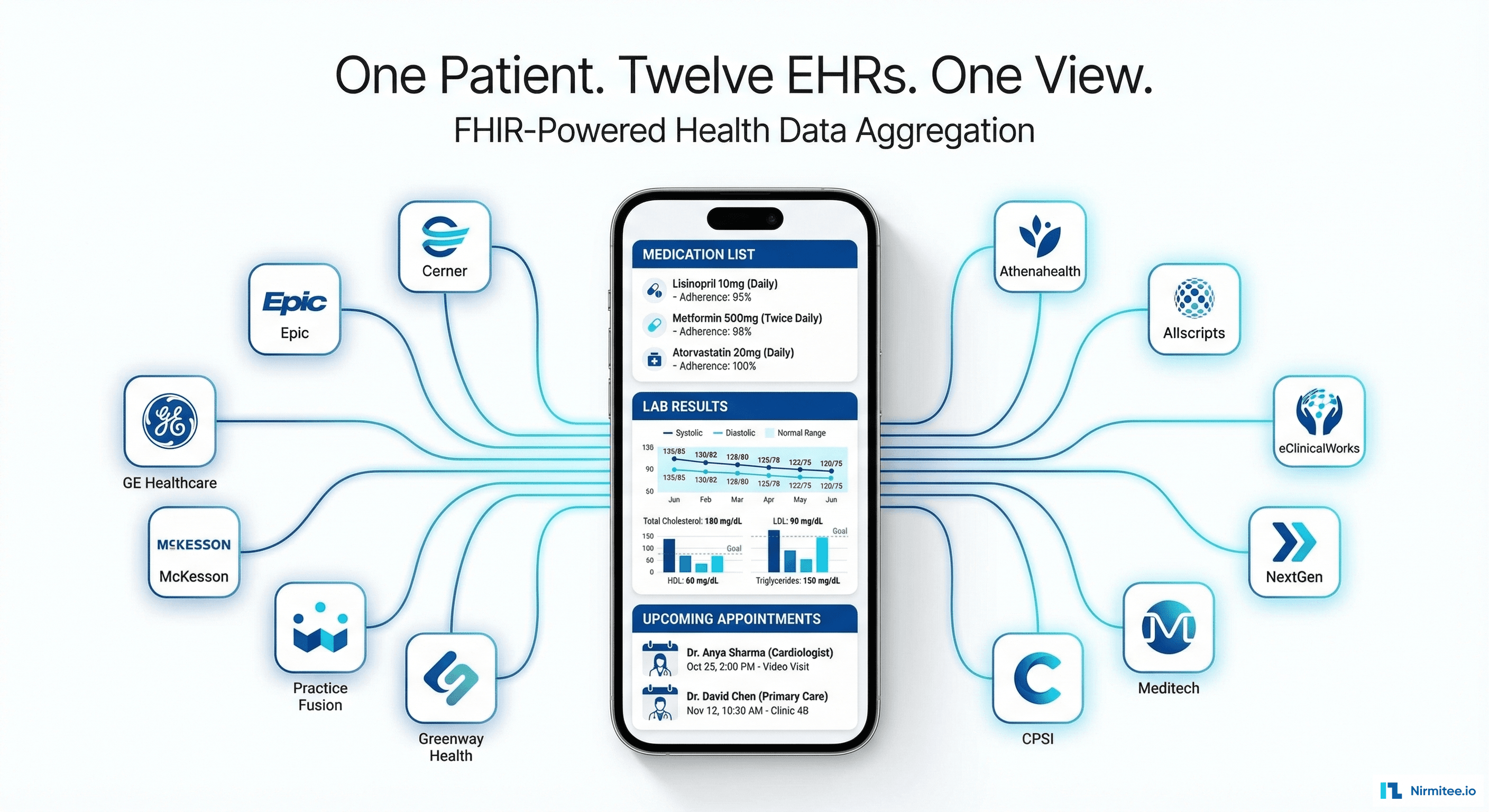
Can the platform integrate with existing EHR systems?
Yes. The platform exposes and consumes FHIR R4 APIs for bi-directional data exchange. Currently integrated with Epic (via App Orchard) and Athena (via Marketplace) for patient demographics, medication lists, and problem lists. Session summaries can be pushed to the referring provider's EHR as DocumentReference resources with appropriate 42 CFR Part 2 consent and re-disclosure notices attached.
What measures prevent therapist burnout on the platform?
The scheduling engine enforces configurable guardrails: maximum consecutive sessions (default 4), mandatory breaks between high-acuity patients, maximum daily session hours (default 6), and automatic time blocking for documentation. The system monitors therapist metrics (session volume, cancellation patterns, documentation completion time) and alerts practice managers when patterns suggest burnout risk. Therapist satisfaction surveys are administered quarterly, with results shared anonymously with the client's leadership team.
Was this case study helpful?