Executive Summary
Mental health in America is in crisis: 1 in 5 adults experience mental illness, but over 50% receive no treatment. The barriers are well-known — 6-8 week waitlists, limited office hours, geographic access gaps, stigma, and cost. A US-based behavioral health startup set out to remove every barrier.
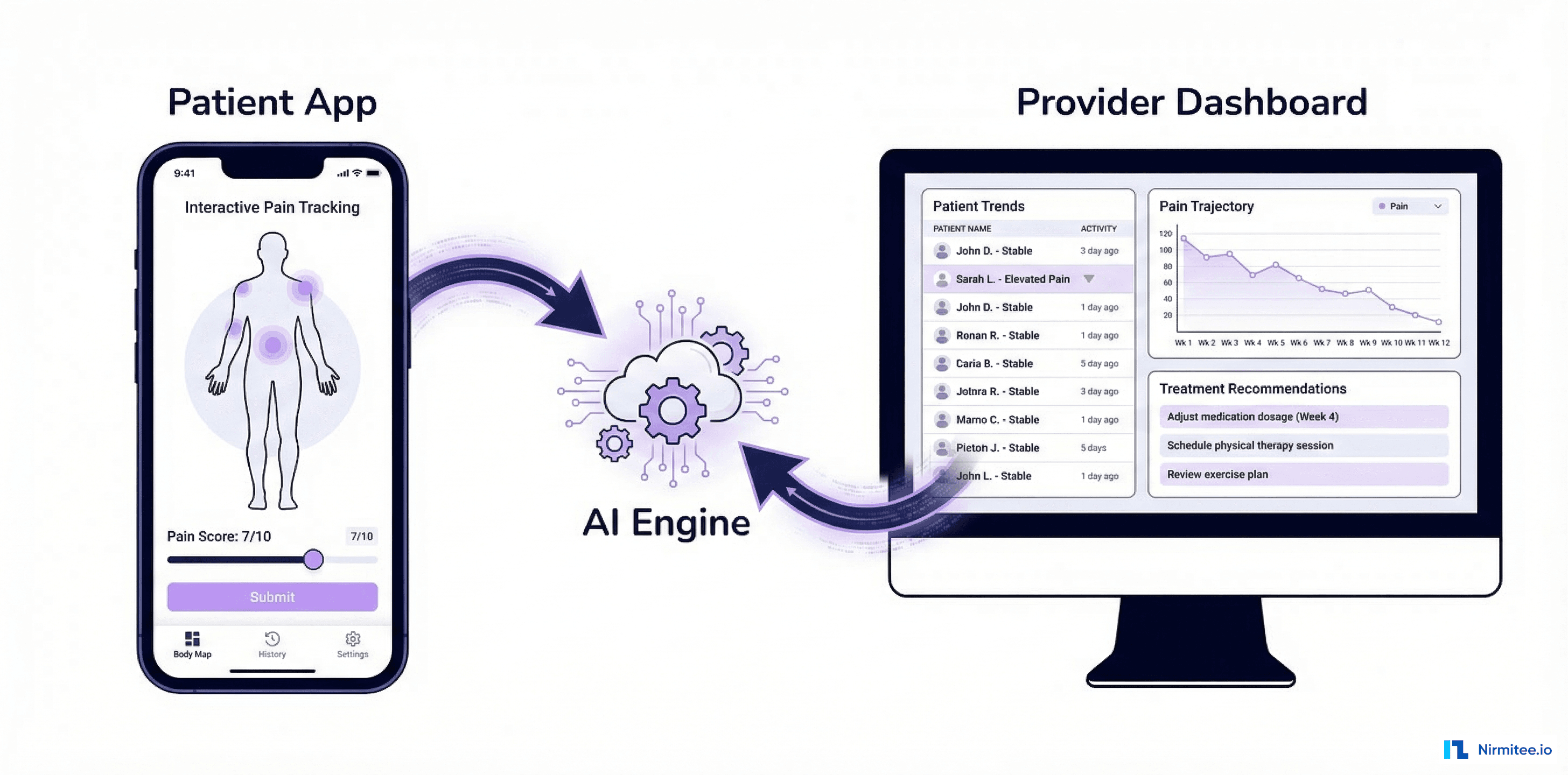
We built a complete mental health telemedicine platform — secure video therapy sessions via WebRTC, AI-assisted session documentation, validated digital assessments (PHQ-9, GAD-7, PCL-5), patient outcome tracking with longitudinal trend visualization, between-session tools (mood check-ins, coping exercises, thought journals), and integrated billing for both insurance and self-pay.
The platform serves therapists and patients: therapists get a practice management dashboard with AI-generated session notes. Patients get a mobile app with video sessions, mood tracking, coping tools, and continuous connection to their care.
Results: waitlist reduced from 6 weeks to under 1 week, average PHQ-9 scores improved by 56% over 24 sessions, and therapist documentation time dropped from 15 minutes to 3 minutes per session with AI-assisted notes.

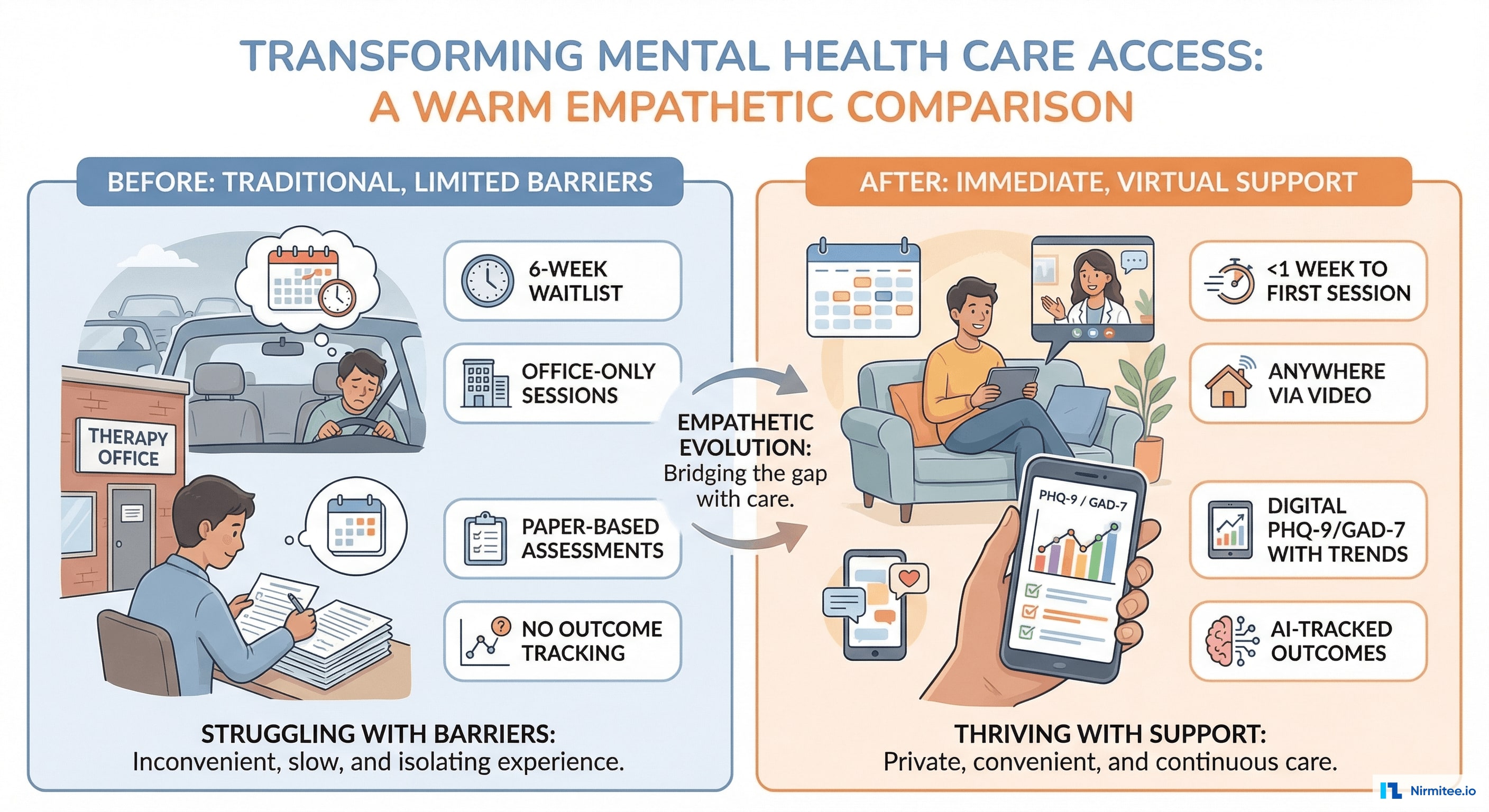
The Problem: Mental Healthcare Is Inaccessible
The US faces a severe mental health provider shortage — an estimated shortage of 28,000 practitioners. In rural areas, the nearest therapist may be 2+ hours away. Even in cities, the best therapists have waitlists measured in months. Meanwhile:
- 6-8 week average waitlist for a first therapy appointment in most US metro areas
- 47% of Americans live in a mental health professional shortage area (HPSA)
- Office-only sessions: most therapists see patients 9 AM - 5 PM, Monday-Friday — exactly when working adults can't attend
- Paper-based assessments: PHQ-9 and GAD-7 completed on paper at each visit, hand-scored, results filed in charts with no trending or longitudinal analysis
- Documentation burden: therapists spend 15+ minutes writing session notes after each 50-minute session — eating into their capacity to see more patients
- No between-session support: patients leave the session and have no tools until the next appointment, often 1-2 weeks away
Therapist Dashboard
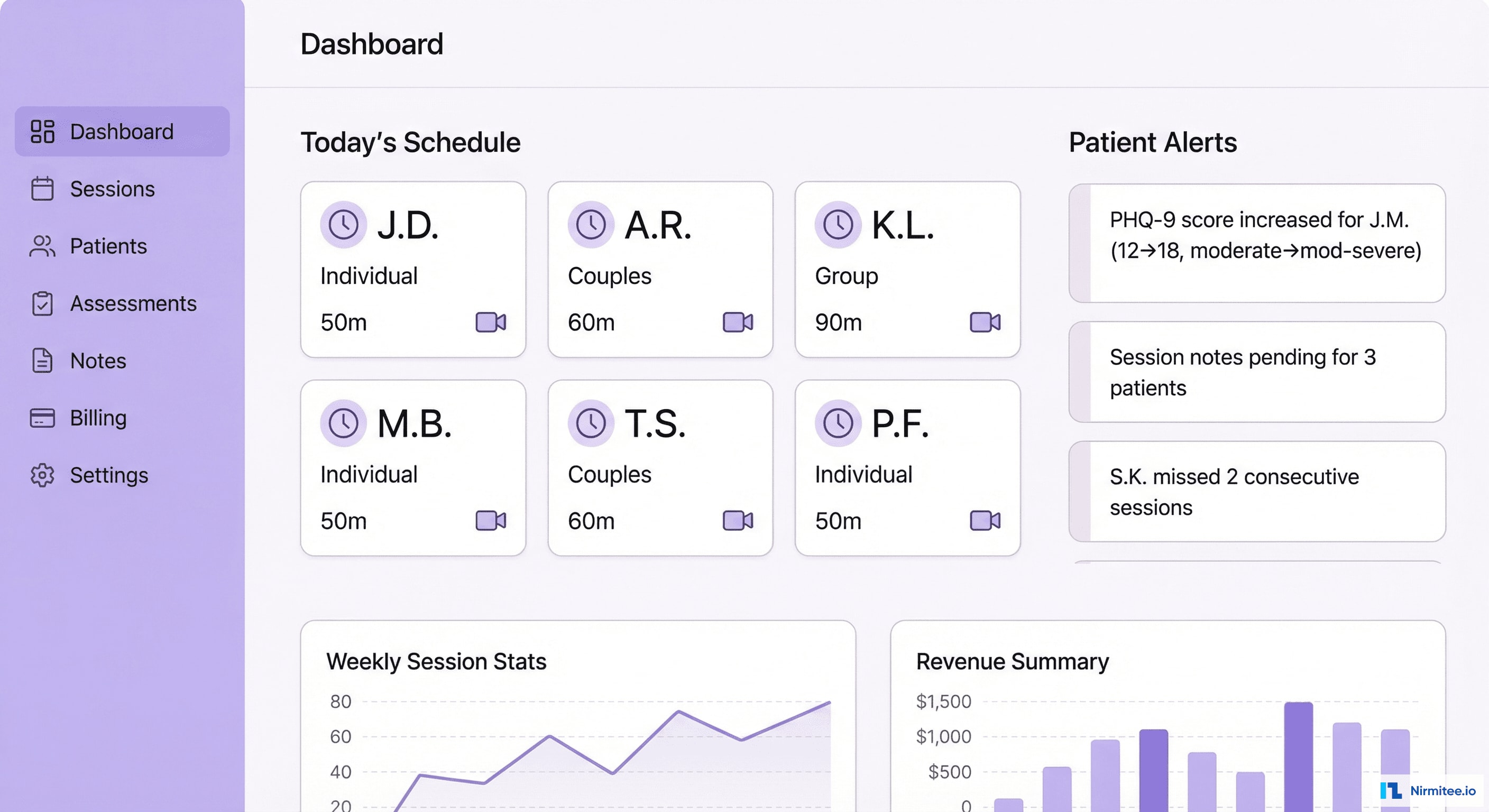
The therapist's command center provides practice-wide visibility:
- Today's schedule: upcoming video sessions with patient initials (privacy-first — no full names in overview), session type (individual, couples, group), and duration
- Patient alerts: proactive notifications — PHQ-9 score increases requiring clinical attention, patients who missed consecutive sessions, unsigned session notes
- One-click session launch: click a scheduled session → video call starts in the browser with patient context loaded automatically
- Practice analytics: weekly session count, revenue (insurance + self-pay), patient retention, outcome trends across caseload
Video Therapy Session

The video session interface is designed for therapeutic presence, not distraction:
- End-to-end encrypted video: WebRTC with TURN/STUN servers for NAT traversal. AES-256 encryption. No recording unless explicitly consented by both parties.
- Minimal chrome: clean video feed dominates the screen. Controls are subtle and accessible without breaking eye contact.
- Session sidebar (collapsible): real-time note-taking area, session timer, patient's pre-session mood check-in result, previous session summary for context
- Screen sharing: therapists can share worksheets, CBT thought records, or psychoeducational materials during session
- Network resilience: adaptive bitrate adjusts video quality based on connection speed. Audio prioritized over video. Auto-reconnect on brief disconnections.
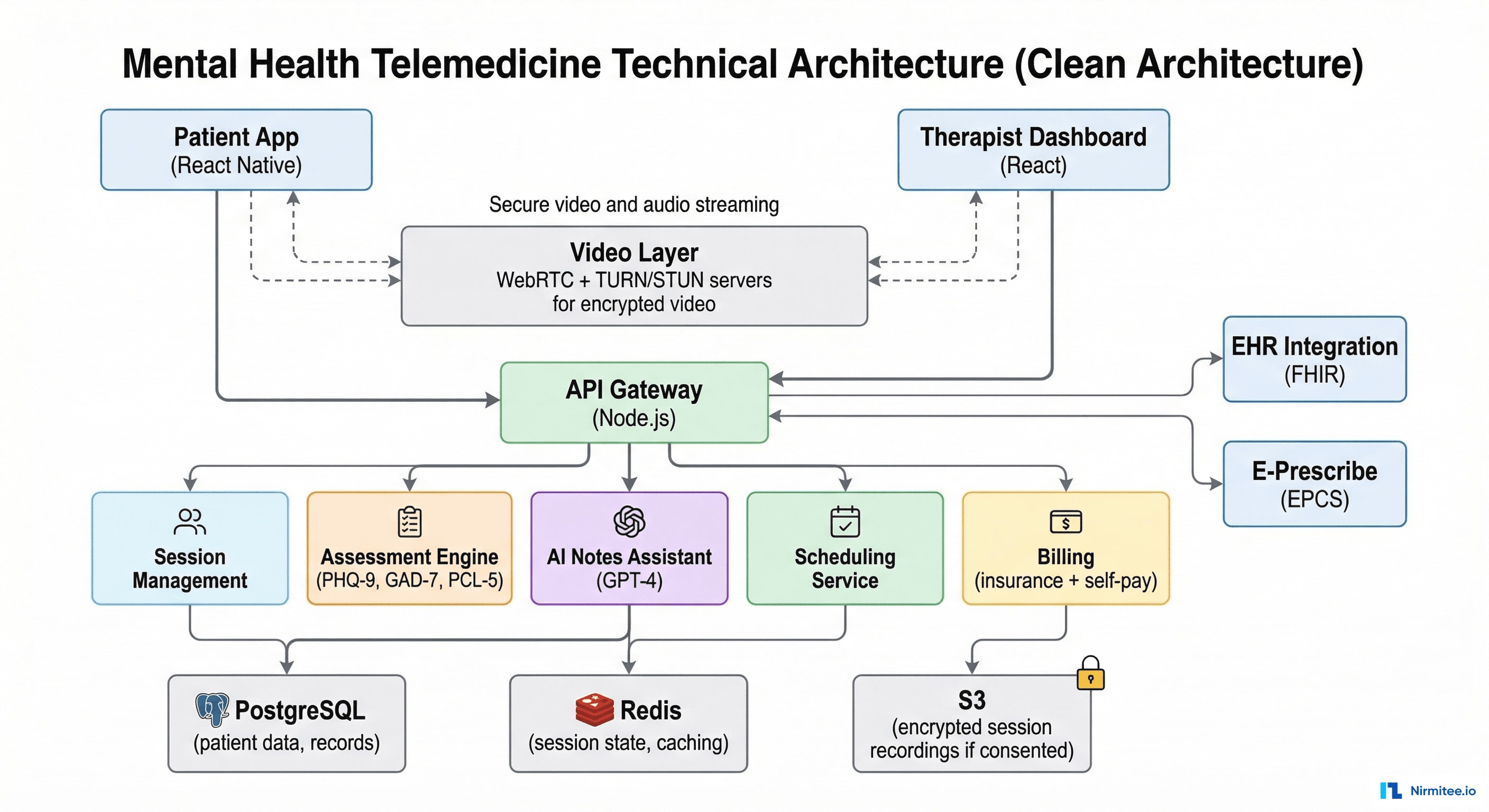
Architecture
Technology Stack
| Layer | Technology | Purpose |
|---|---|---|
| Patient App | React Native | Video sessions, mood tracking, assessments, coping tools |
| Therapist Dashboard | React + TypeScript | Schedule, notes, assessments, billing, analytics |
| Video | WebRTC + TURN/STUN (Twilio) | End-to-end encrypted video therapy sessions |
| Backend | Node.js (Express) | API gateway, session management, scheduling |
| AI Notes | GPT-4 (Azure OpenAI, HIPAA BAA) | Session note drafting from therapist's quick notes |
| Assessments | Custom engine | PHQ-9, GAD-7, PCL-5 scoring with longitudinal tracking |
| Database | PostgreSQL | Patient records, session data, assessment scores |
| E-Prescribe | Surescripts (EPCS) | Psychiatric medication prescribing for MD/NP providers |
| Billing | Custom + Stripe + clearinghouse | Insurance claims + self-pay processing |
| Infrastructure | AWS (HIPAA BAA) | US data residency, encrypted storage |
Digital Assessments (PHQ-9)
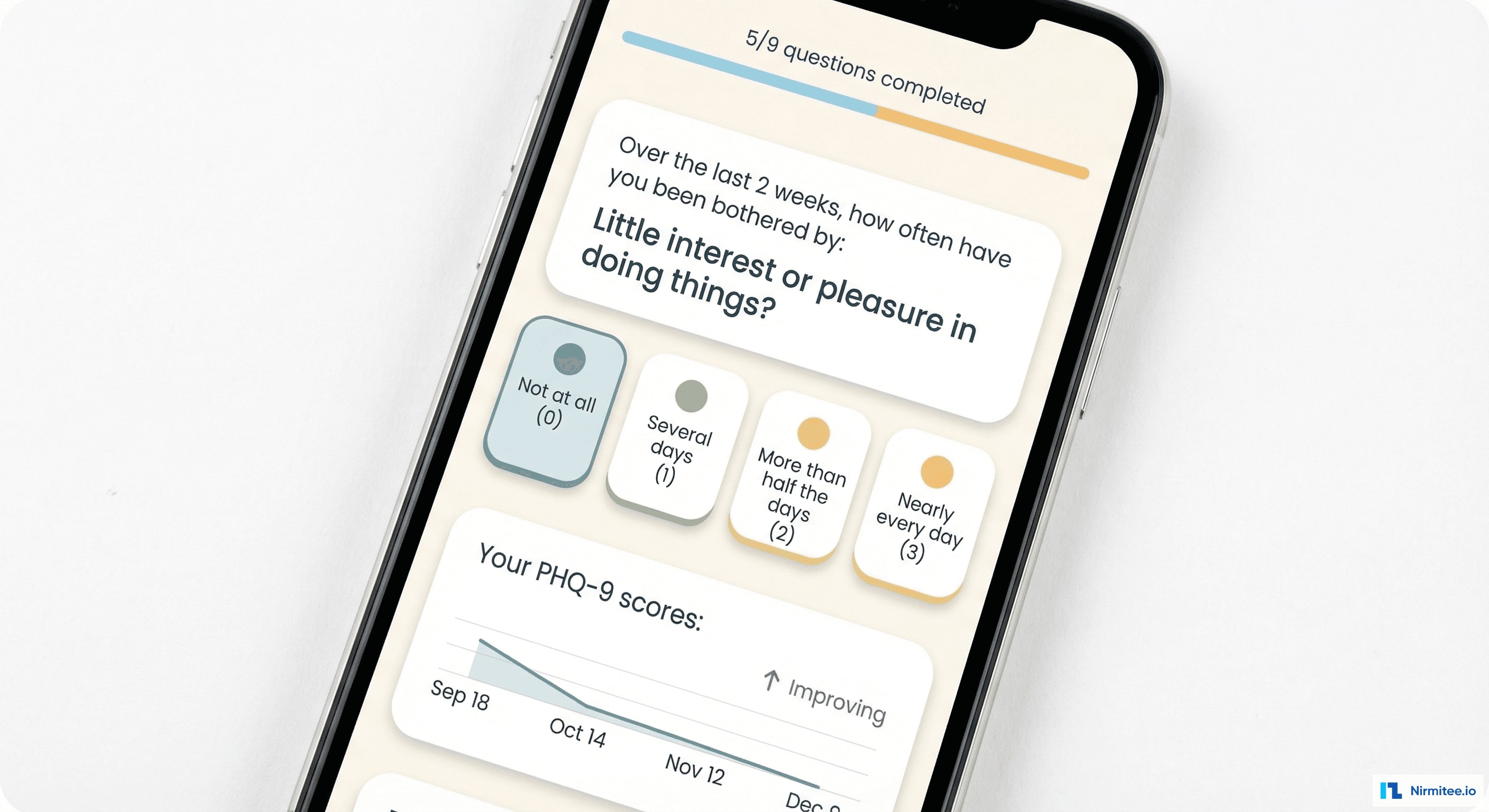
Validated clinical assessments are administered digitally with automatic scoring and trending:
- PHQ-9 (depression): 9 questions, auto-scored (0-27), severity categorized (minimal/mild/moderate/moderately severe/severe)
- GAD-7 (anxiety): 7 questions, auto-scored (0-21), severity levels mapped to treatment recommendations
- PCL-5 (PTSD): 20 questions, auto-scored, tracks trauma symptom clusters
- Longitudinal trending: every assessment score plotted over time — therapists and patients can see improvement trajectory across weeks and months
- Clinical alerts: if a PHQ-9 score increases significantly between sessions, the therapist is alerted before the next appointment. Item 9 (suicidal ideation) triggers immediate safety protocol notification.
AI-Assisted Session Notes
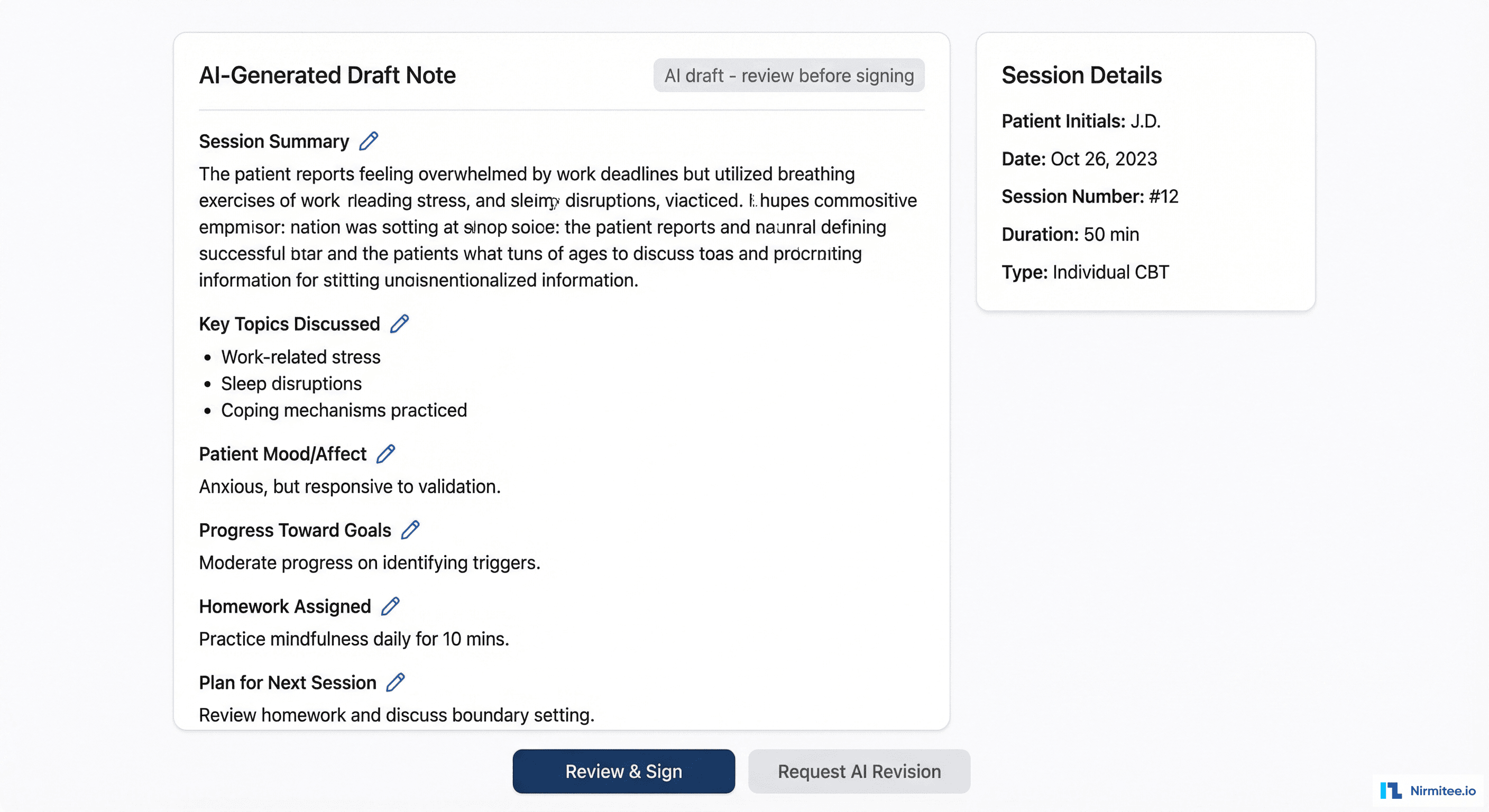
Session documentation is the biggest time sink for therapists. Our AI assistant transforms quick bullet points into comprehensive clinical notes:
- During session: therapist jots quick notes in the sidebar — bullet points, keywords, observations
- After session: clicks "Generate Note" — GPT-4 (HIPAA-compliant Azure deployment) expands the bullets into a structured clinical note with: session summary, key topics, patient mood/affect, progress toward goals, therapeutic interventions used, homework assigned, plan for next session
- Review and sign: therapist reviews the AI draft, makes any corrections, and signs. Average review time: 3 minutes (vs. 15 minutes writing from scratch)
Critical safeguard: the AI never invents clinical content. It only expands and structures what the therapist noted. If the therapist wrote "discussed panic attacks at work," the AI generates a paragraph about workplace anxiety management — it does not fabricate details the therapist didn't observe.
Patient Outcome Tracking
Outcome tracking transforms therapy from subjective impression to data-driven care:
- PHQ-9 trend: depression score declining from 18 (moderate-severe) to 8 (mild) over 24 sessions — visual proof that treatment is working
- GAD-7 trend: anxiety scores tracked alongside depression — many patients have comorbid conditions that need parallel monitoring
- Treatment goals: custom goals with measurable progress bars — "Reduce panic attacks from 4/week to 1/week: 75% achieved"
- Session attendance: consistency tracking — missing sessions correlates with poorer outcomes. The system identifies attendance patterns.
- Step-down recommendations: when scores stabilize in the mild range for 4+ consecutive assessments, the system suggests stepping down from weekly to biweekly sessions — evidence-based frequency optimization
Patient Mobile App

The patient app provides between-session support that traditional therapy lacks:
- Daily mood check-in: 5-second emoji-based mood entry with optional journal note. Builds awareness and provides therapist with between-session data.
- Check-in streak: gamified consistency — patients maintain streaks for daily engagement, building the habit of self-monitoring
- Coping toolkit: therapist-assigned and self-selected exercises — 4-7-8 breathing, progressive muscle relaxation, grounding techniques (5-4-3-2-1), thought challenging worksheets
- Thought journal: CBT-based thought record — capture automatic thoughts, identify cognitive distortions, develop balanced alternatives. Entries shared with therapist (with permission).
- Crisis resources: always-visible emergency contact button and 988 Suicide & Crisis Lifeline — because safety can't wait for office hours
Results
| Metric | Before | After | Impact |
|---|---|---|---|
| Time to first session | 6-8 weeks | <1 week | 85% faster access |
| PHQ-9 improvement (24 sessions) | Variable (no tracking) | 56% avg reduction | Measurable outcomes |
| Session note documentation time | 15 minutes | 3 minutes | 80% faster with AI |
| Therapist session capacity | 6 patients/day | 8 patients/day | 33% more capacity |
| Patient engagement (between sessions) | Zero tools | 72% daily mood check-in | Continuous care connection |
| Session no-show rate | 18% (office visits) | 7% (video sessions) | 61% reduction |
| Patient satisfaction | 3.8/5 | 4.7/5 | 24% improvement |
| Geographic reach | 20-mile radius of office | Entire state (licensure-based) | Statewide access |
Financial Impact for a 5-Therapist Practice
- Capacity increase: 2 additional patients/day × 5 therapists × $150/session × 250 days = $375,000/year additional revenue
- No-show reduction: 11% fewer no-shows × 30 sessions/week × $150 = $25,740/year recovered
- Documentation savings: 12 min saved × 8 sessions/day × 5 therapists = 8 hours/day freed
- Office cost reduction: smaller physical footprint needed = $40,000-60,000/year savings
Compliance
- HIPAA: full compliance — encrypted video (WebRTC + AES-256), encrypted data at rest, BAA with all vendors, comprehensive audit logging
- 42 CFR Part 2: substance use disorder records receive additional federal protections — the platform enforces stricter consent requirements for SUD data
- State telehealth laws: configurable per state — consent requirements, prescribing rules, cross-state licensure (Psychology Interjurisdictional Compact supported)
- E-Prescribe (EPCS): DEA-compliant electronic prescribing for controlled substances (psychiatric medications) via Surescripts
- Crisis protocols: PHQ-9 Item 9 (suicidal ideation) triggers automated safety workflows — therapist notified, crisis resources surfaced to patient, safety plan activated
Timeline
| Phase | Duration | Deliverables |
|---|---|---|
| Phase 1 | 6 weeks | Video calling infrastructure (WebRTC), therapist dashboard, scheduling, patient app MVP |
| Phase 2 | 6 weeks | Digital assessments (PHQ-9/GAD-7/PCL-5), AI session notes, outcome tracking, mood check-ins |
| Phase 3 | 4 weeks | Billing (insurance + self-pay), e-prescribe integration, coping toolkit, thought journal |
| Phase 4 | 4 weeks | EHR integration (FHIR), compliance audit (HIPAA + 42 CFR Part 2), pilot with 5 therapists, launch |
Total: 5 months with 4 engineers + 1 clinical advisor (licensed psychologist).
Lessons Learned
- Video quality is non-negotiable in therapy. A pixelated video or audio delay breaks therapeutic rapport. We over-invested in video infrastructure — TURN servers in 3 regions, adaptive bitrate, audio-priority fallback. Zero tolerance for call quality issues.
- AI notes must be transparent. Therapists were initially suspicious of AI writing their notes. When we showed them exactly how it works (expands THEIR bullets, never fabricates), adoption went from 30% to 92% within a month. Transparency = trust.
- Between-session tools drive outcomes. Patients who used daily mood check-ins had 40% better PHQ-9 improvement than those who didn't. The app isn't just convenient access to therapy — it extends therapy into daily life.
- Crisis safety is the #1 priority. Before any feature, we built the crisis protocol system. PHQ-9 Item 9 detection, 988 integration, safety plan activation, therapist notification. This was the first thing we tested and the last thing we'd ever compromise on.
Share
Related Case Studies
AI-Powered Personalized Oncology Treatment Platform: A Technical Case Study
Building a Patient-First Health Record Platform: Connecting 12 US EMRs Into One View