Part of our complete guide to What Are AI Agents in Healthcare and How Are They Transforming Care Delivery?.
Healthcare is at an inflection point. After years of incremental AI adoption, a fundamental shift is underway: the transition from generative AI tools that assist human workers to agentic AI systems that autonomously execute entire workflows end to end. These are not chatbots with better prompts. They are orchestrated, multi-step agents that read clinical data, make decisions within defined guardrails, take action across systems, and learn from outcomes.
This momentum was already visible on the conference floor — see our take from HIMSS25 on the rise of agentic AI.
The numbers tell the story. According to Deloitte's 2026 health care survey, 61% of healthcare executives are already building or implementing agentic AI initiatives, and 85% plan to increase investment over the next two to three years.
Gartner projects that by 2027, 30% of payers will use agentic AI to optimize payer-provider workflows, reducing manual workloads by 40%. The agentic AI healthcare market itself is projected to reach $33.66 billion by 2035, growing at 45.6% CAGR.
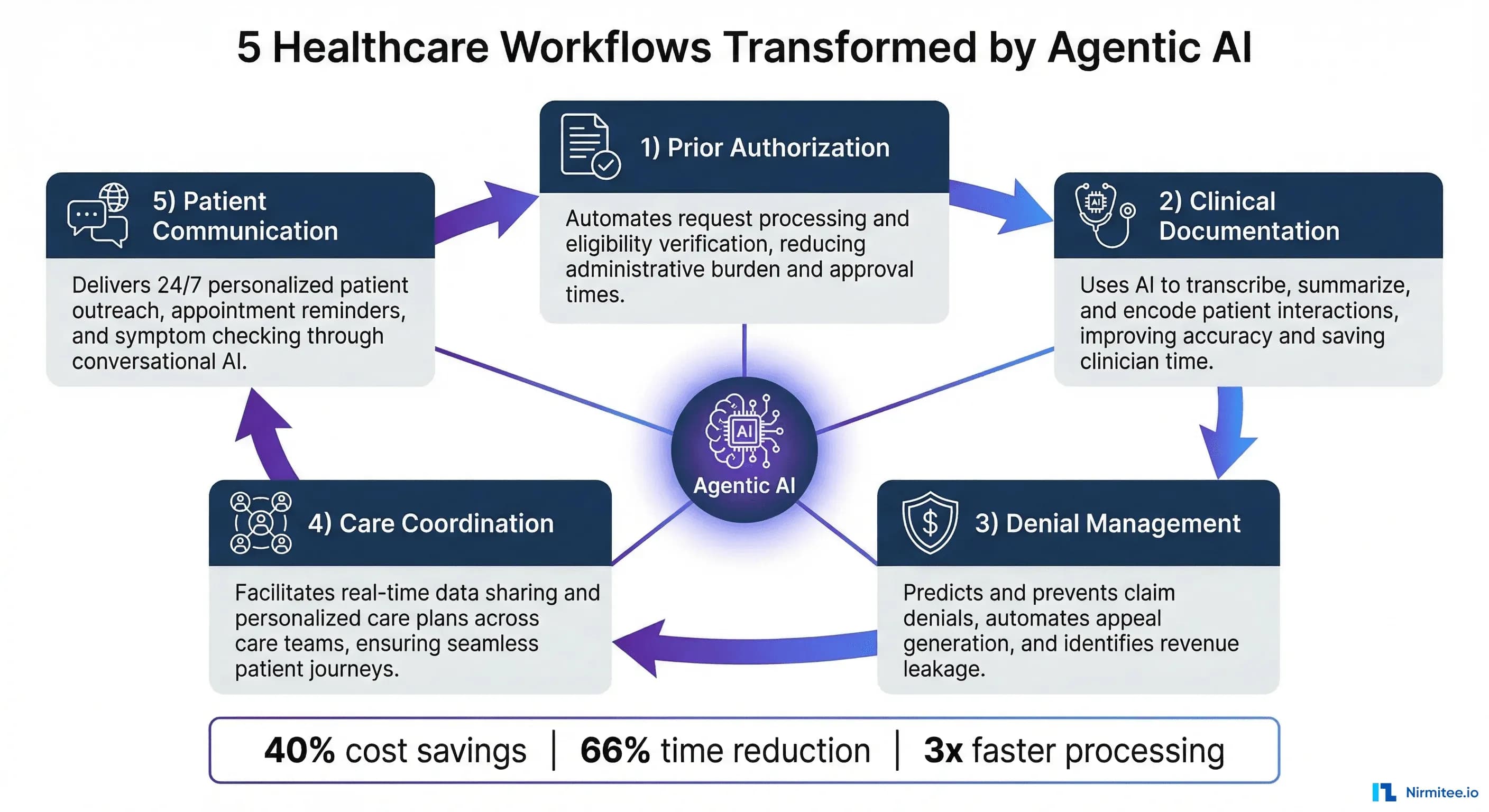
But where exactly will this transformation hit hardest? Which workflows are ripe for autonomous AI agents, and what does the architecture look like in practice? This article examines five healthcare workflows where agentic AI will deliver the most dramatic impact by 2027, with real-world examples, architectural patterns, and projected ROI for each.
If you are exploring how agentic AI fits into your organization's broader strategy, our deep dive on the role of agentic AI in healthcare workflow optimization provides the foundational framework for what follows.
1. Prior Authorization: From 14-Day Bottleneck to Same-Day Decisions
The Problem
Prior authorization remains one of healthcare's most reviled administrative burdens. The process is a relic of a paper-based era: providers submit clinical documentation to payers, who review it against coverage criteria, often through manual processes that stretch across days or weeks.
The American Medical Association reports that physicians spend an average of 14 hours per week on prior authorization tasks. For hospitals, a single prior auth request costs $11 on average to process, with some complex requests exceeding $50.
The regulatory landscape is shifting fast. The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) now sets hard deadlines for insurers. Medicare Advantage, Medicaid managed care, CHIP, and ACA marketplace plans must answer standard requests within seven days. Urgent requests must be answered within 72 hours. By 2027, these payers must support standardized electronic APIs for authorization tracking and decision rationale access.
Also, the CMS WISeR (Wasteful and Inappropriate Service Reduction) Model, launched in January 2026 across six states, uses AI and machine learning alongside human clinical review to screen prior authorization requests for Medicare services.
How Agentic AI Solves It
An agentic prior authorization system does not simply fill in forms. It operates as an autonomous workflow orchestrator that:
- Reads the clinical context by pulling relevant patient data from the EHR, including diagnoses, lab results, imaging reports, treatment history, and medications
- Assembles the authorization packet by matching clinical evidence against payer-specific coverage criteria, medical policies, and LCD/NCD guidelines
- Submits electronically via FHIR-based APIs or payer portals, with all required documentation attached in the correct format
- Monitors and escalates by tracking submission status, responding to payer information requests, and routing edge cases to human reviewers with a pre-built clinical summary
- Learns from outcomes by analyzing approval and denial patterns to improve future submissions, flagging criteria changes, and payer behavior shifts
Architecture Pattern
The typical agentic prior auth system uses a multi-agent orchestration pattern: a supervisor agent coordinates specialized sub-agents for data retrieval, criteria matching, document assembly, and submission.
The system integrates with EHRs via FHIR R4 APIs, connects to payer portals through X12 278 transactions or proprietary APIs, and maintains a knowledge base of payer policies that is continuously updated.
Critical architectural decisions include the human-in-the-loop threshold: most production systems route cases below a confidence score (typically 0.85-0.90) to human reviewers, while high-confidence cases proceed autonomously. This mirrors the CMS WISeR model's approach, where AI serves as the initial screening layer but human clinicians review all denials.
Expected ROI
MUSC Health reports that AI agents now complete 40% of prior authorizations without human involvement, with the remaining 60% greatly accelerated through AI-assisted assembly. Organizations implementing agentic prior auth systems are seeing:
- 70-80% reduction in staff time per authorization
- 14 days to under 24 hours average turnaround
- $7-9 savings per authorization processed
- 15-20% improvement in first-pass approval rates
By 2027 Prediction
By 2027, 60% of routine prior authorizations at large health systems will be fully autonomous, with human review reserved for complex or novel cases. The combination of CMS mandates for electronic APIs and agentic AI capabilities will make the fax-and-phone prior auth process functionally obsolete for standard procedures.
2. Clinical Documentation
The Problem
The documentation challenge is not just about time. Incomplete or inaccurate notes cascade into downstream problems: coding errors that trigger claim denials, missed quality metrics, compliance gaps, and fragmented care coordination.
The documentation burden also directly impacts patient experience, as physicians focused on screens rather than patients erode the therapeutic relationship.
How Agentic AI Solves It
Ambient AI documentation systems represent one of the most mature applications of agentic AI in healthcare. These systems go far beyond simple speech-to-text transcription:
- Ambient listening and understanding: Microphone-enabled systems capture the natural physician-patient conversation in real time, using advanced NLP to distinguish between clinical findings, patient concerns, social history, and action items
- Structured note generation: The AI agent generates a complete clinical note organized into standard sections (HPI, ROS, physical exam, assessment, plan) with appropriate medical terminology, ICD-10 codes, and CPT suggestions
- Cross-reference and enrichment: The agent pulls relevant context from the patient's EHR record, including medication lists, allergy alerts, and recent lab results, weaving this into the note for completeness
- Quality validation: Before presenting the note to the physician, the agent checks for documentation completeness against payer requirements, quality measure criteria, and compliance standards
- One-click approval: The physician reviews and signs the note, typically in under two minutes, with AI-flagged items highlighted for attention
Architecture Pattern
Ambient documentation systems use a streaming pipeline architecture: audio capture feeds into a real-time ASR (automatic speech recognition) engine, which outputs a transcript to a clinical NLU (natural language understanding) model.
The NLU model identifies medical entities, relationships, and intent, feeding a structured note generator that maps findings to documentation templates. The entire pipeline operates with sub-second latency, generating notes that are often complete before the visit ends.
The agentic component emerges in the post-generation phase. An autonomous quality agent reviews the note against multiple criteria. An integration agent pushes it to the EHR. A learning agent tracks physician edit patterns to improve future note quality.
Expected ROI
The evidence base for ambient AI documentation is now substantial. Kaiser Permanente's rollout across multiple regions, involving over 63,000 patient encounters, showed significant reductions in after-hours documentation. Healthcare organizations using mature ambient AI platforms report:
- 81% reduction in documentation time (per Commure Ambient AI data)
- 66% decrease in after-hours EHR usage
- 25% reduction in claim denials linked to documentation gaps
- 98% user satisfaction in physician surveys (Catalonia's ALMA deployment)
By 2027 Prediction
By 2027, ambient AI documentation will be standard equipment in 75% of US health system exam rooms. The technology will expand beyond physician notes to capture nursing assessments, therapy sessions, and care team huddles.
Proactive documentation agents will pre-populate visit notes with relevant context before the patient even arrives, transforming documentation from a post-visit chore to a real-time, AI-managed process.
3. Denial Management: From Reactive Recovery to Proactive Prevention
The Problem
Claim denials are hemorrhaging revenue across the US healthcare system. The average denial rate has climbed to about 10-15% in manual RCM environments, with some specialties and payers exceeding 20%. Each denied claim costs an average of $25 or more to reprocess, and up to 60% of denied claims are never reworked at all, representing pure revenue loss. The total cost of denials to the US healthcare system exceeds $260 billion annually.
The denial problem is getting worse, not better. Payers are deploying increasingly advanced algorithms to identify documentation discrepancies, coding inconsistencies, and authorization gaps in milliseconds.
Providers using manual denial management processes simply cannot keep pace with this algorithmic scrutiny. As agentic AI transforms data management in healthcare, denial management is becoming one of its highest-ROI applications.
How Agentic AI Solves It
Agentic AI denial management operates across three layers: prevention, detection, and recovery.
Prevention Layer:
- Pre-submission audit agent: Reviews every claim before submission, checking documentation completeness, coding accuracy, authorization status, and payer-specific requirements
- Predictive denial scoring: Assigns a denial probability to each claim based on historical patterns, payer behavior, coding combinations, and documentation quality, flagging high-risk claims for human review
- Real-time coding validation: Cross-references CPT, ICD-10, and modifier combinations against NCCI edits, LCD/NCD policies, and payer-specific rules
Detection Layer:
- Denial pattern analysis agent: Continuously monitors denial data streams, identifying trending denial reasons, payer policy changes, and systemic issues across departments or providers
- Root cause classification: Automatically categorizes denials by root cause (medical necessity, missing info, coding error, auth required, timely filing) and routes to appropriate remediation workflows
Recovery Layer:
- Appeal drafting agent: Generates customized appeal letters with supporting clinical evidence, peer-reviewed citations, and payer-specific argumentation strategies
- Automated resubmission: Corrects and resubmits claims with straightforward fixes (missing modifiers, incorrect place of service) without human intervention
- Outcome tracking and learning: Records appeal outcomes, identifies winning strategies by denial type and payer, and continuously refines the prevention layer
Architecture Pattern
Denial management agents use a closed-loop learning architecture. The prevention agent and recovery agent share a common knowledge graph of payer policies, denial patterns, and appeal outcomes. Every denial that enters the system enriches this graph, making future prevention more accurate. The system connects to clearinghouses for real-time remittance data, EHRs for clinical documentation, and coding engines for validation.
Expected ROI
Organizations deploying AI-native denial management report transformative results:
- Denial rate drops from 10-15% to about 5.7%
- Cost per denied claim reprocess: from $25+ to under $1.50
- Clean claim rate improves from 75-85% to above 95%
- Appeal success rate increases by 30-40% with AI-drafted appeals
- Net revenue recovery of 2-4% of total patient revenue
By 2027 Prediction
By 2027, the denial management paradigm will invert. Instead of reactive "deny and appeal" cycles, agentic AI will enable proactive, zero-touch claim adjudication where 90%+ of routine claims are clean on first submission. Health systems that fail to adopt AI-powered denial prevention will face widening revenue gaps as payer algorithms grow more advanced. The $260 billion denial problem will shrink by an estimated 35-45% at AI-enabled organizations.
4. Care Coordination: AI as the Orchestrator Across Fragmented Systems
The Problem
Care coordination failures are one of the most expensive and dangerous problems in US healthcare. An estimated 80% of serious medical errors involve miscommunication during care transitions. Post-discharge follow-up gaps contribute to a 15-20% hospital readmission rate within 30 days, costing Medicare alone over $26 billion annually.
The root cause is systemic fragmentation: patients navigate across primary care physicians, specialists, hospitals, post-acute facilities, home health agencies, and pharmacies, with no single entity maintaining a unified view of their care journey.
Care coordinators, where they exist, are overwhelmed. A typical coordinator manages 150-200 patients, manually tracking referrals, scheduling follow-ups, confirming medication reconciliation, and monitoring care plan adherence across disparate systems that rarely communicate with each other.
How Agentic AI Solves It
An agentic care coordination system acts as a persistent, always-on orchestrator that maintains a unified longitudinal patient record and proactively manages transitions across the care continuum:
- Discharge planning agent: Triggers 48 hours before anticipated discharge, assembles the care transition package (medications, follow-up appointments, patient education, DME orders), and coordinates with receiving providers.
- Referral management agent: Tracks every referral from initiation to completion, automatically scheduling appointments, sending clinical summaries to specialists, and alerting coordinators when referrals stall.
- Follow-up scheduling agent: Ensures post-discharge and post-procedure follow-ups are scheduled within guideline-recommended timeframes, with automated patient outreach via preferred communication channels.
- Medication reconciliation agent: Cross-references discharge medications against pre-admission regimens, specialty prescriptions, and pharmacy fill data, flagging conflicts, duplications, and gaps.
- Risk stratification agent: Continuously scores patients for readmission risk, social determinants of health barriers, and care plan non-adherence, escalating high-risk patients to human care teams.
Architecture Pattern
Care coordination agents require a federated integration architecture that connects to multiple EHR instances, HIE networks, pharmacy systems, and community services directories.
The observability framework for agentic AI in healthcare becomes critical here, as care coordination agents operate across organizational boundaries where failures can have clinical consequences.
The orchestration layer uses event-driven architecture: ADT (admit/discharge/transfer) messages, lab result notifications, referral status updates, and scheduling events all trigger appropriate agent actions.
A unified patient timeline aggregates data from all connected sources, giving the coordination agent complete situational awareness.
Expected ROI
Early deployments of AI-powered care coordination show compelling results:
- 35% reduction in discharge-to-admission delays for post-acute transitions
- 20-30% decrease in 30-day readmission rates
- 10-point increase in patient satisfaction scores
- 50% faster referral completion times
- MIMIT Health achieved 459% ROI and $1.5 million in savings with AI-powered coordination agents
By 2027 Prediction
By 2027, AI care coordination agents will be the connective tissue of integrated delivery networks. CMS value-based care models will increasingly require showed AI-assisted coordination capabilities as a condition of participation.
The most advanced systems will incorporate social determinants of health data, community resource matching, and patient-reported outcomes into their coordination logic, moving from reactive handoff management to proactive population health orchestration.
5. Patient Communication: Intelligent, Multilingual, Always-On Engagement
The Problem
Healthcare's communication infrastructure is stuck in the 1990s. Patients navigate voicemail trees, endure hold times averaging 8-12 minutes, and play phone tag for simple tasks like scheduling appointments or asking about test results.
For the 25 million US residents with limited English proficiency, accessing healthcare information in their preferred language adds another layer of friction.
The consequences are measurable: 23% of patients miss appointments due to scheduling friction, contributing to an estimated $150 billion in annual revenue loss from no-shows. Post-discharge communication gaps contribute to preventable readmissions. And patient satisfaction scores, increasingly tied to reimbursement through value-based care models, suffer when basic communication needs go unmet.
How Agentic AI Solves It
Agentic patient communication systems replace fragmented, reactive touchpoints with a continuous, personalized engagement layer that operates across channels and languages:
- Intelligent scheduling agent: Handles appointment requests via voice, text, web chat, or patient portal, accessing real-time provider availability, insurance verification, and scheduling rules to book appointments in a single interaction
- Pre-visit preparation agent: Sends personalized pre-visit instructions, intake forms, and medication lists for review, collects updated information, and flags clinical changes for provider attention before the appointment
- Results communication agent: Delivers lab results, imaging reports, and care plan updates through patient-preferred channels with appropriate context, automatically routing abnormal results to provider review workflows
- Post-discharge follow-up agent: Conducts structured post-discharge check-ins at guideline-recommended intervals, assessing symptom status, medication adherence, and care plan compliance, escalating concerns to clinical teams
- Multilingual engagement engine: Provides native-quality communication in 95+ languages, adapting not just vocabulary but cultural context, health literacy level, and communication preferences to each patient
Architecture Pattern
Patient communication agents use an omnichannel orchestration pattern with a unified conversation state that persists across voice, SMS, web chat, patient portal, and mobile app channels. The system integrates with scheduling engines, EHRs, lab information systems, and billing platforms to provide contextual responses without transferring patients between departments.
Natural language understanding models are fine-tuned on healthcare-specific intents and entities, with built-in HIPAA compliance for PHI handling. The multilingual capability uses specialized medical translation models that understand clinical terminology in context, avoiding the dangerous literal translations that general-purpose translation tools sometimes produce.
Expected ROI
Healthcare organizations deploying agentic patient communication report:
- 85% call deflection rate for routine inquiries (scheduling, billing, directions)
- 30-50% reduction in scheduling-related call volume
- 30-40% decrease in no-show rates with AI-powered reminders and easy rescheduling
- 20-25% improvement in appointment utilization rates
- 15-20 point increase in patient satisfaction scores
By 2027 Prediction
By 2027, AI-powered patient communication will be considered table stakes for competitive health systems. Forrester already designates conversational AI as a baseline requirement in their 2026 Healthcare CX Wave.
The next frontier will be anticipatory communication: AI agents that reach out to patients before they realize they need help. These agents proactively schedule preventive care, flag prescription refill needs, and connect patients with community resources based on social determinants of health data.
The ROI Picture: What C-Suite Leaders Need to Know
Across all five workflows, the financial case for agentic AI investment is compelling. Deloitte's 2026 survey found that 98% of healthcare executives expect a minimum 10% cost savings within two to three years, with 37% anticipating savings exceeding 20%. The specific ROI varies by workflow, but the pattern is consistent: agentic AI delivers returns through labor efficiency, error reduction, revenue recovery, and improved patient outcomes that reduce downstream costs.
What makes 2026-2027 the inflection point is the convergence of three factors:
- Regulatory mandates: CMS rules on prior authorization timelines, interoperability requirements, and quality reporting create compliance-driven urgency that makes AI adoption a regulatory necessity, not just a competitive advantage
- Technology maturity: LLM capabilities, FHIR API adoption, and cloud infrastructure have reached the point where agentic healthcare applications are production-ready, not experimental
- Workforce crisis: With a projected shortfall of over 3.2 million healthcare workers by 2026, automation is not optional but essential for maintaining service levels
Implementation Roadmap: Where to Start
For health system leaders evaluating agentic AI investments, the recommended approach is phased deployment aligned with organizational readiness:
Phase 1 (0-6 months): Quick wins with measurable ROI
- Deploy ambient AI documentation in the highest-volume departments
- Implement AI-powered patient scheduling and communication
- Begin pre-submission claim auditing for denial prevention
Phase 2 (6-12 months): Revenue cycle transformation
- Scale prior authorization automation across payers
- Deploy a full denial management suite with prevention, detection, and recovery
- Integrate care coordination agents for high-risk patient populations
Phase 3 (12-18 months): Enterprise-wide orchestration
- Connect all agentic workflows into a unified AI operations layer
- Implement cross-workflow intelligence sharing and optimization
- Establish observability and governance frameworks for production AI agents
The key is starting with workflows where the data is structured, the rules are well-defined, and the ROI is immediately measurable. Prior authorization and denial management typically offer the fastest financial returns, while clinical documentation delivers the most visible quality-of-life improvement for clinical staff.
The Risks: What Could Go Wrong
It would be irresponsible to discuss agentic AI in healthcare without acknowledging the risks. Gartner predicts that more than 40% of agentic AI projects will be cancelled by the end of 2027. The most common failure modes include:
- Integration complexity: Agentic systems that cannot reliably connect to EHRs, payer systems, and ancillary platforms deliver limited value
- Trust and transparency gaps: Clinicians will reject AI agents they do not understand or trust, regardless of accuracy
- Regulatory uncertainty: The FDA has acknowledged that most AI tools used in healthcare operations have never been reviewed by a federal regulator, creating compliance ambiguity
- Data quality dependencies: AI agents trained on inconsistent or incomplete data will produce inconsistent or incomplete outputs
The mitigation strategy is clear: invest in observability and governance infrastructure from day one, maintain human oversight for clinical decisions, and start with well-bounded workflows before expanding to more complex use cases.
Conclusion: The Agentic Healthcare System of 2027
By 2027, the most advanced health systems will operate with an agentic AI backbone that autonomously manages the administrative and operational workflows that currently consume 30-40% of healthcare spending.
Prior authorizations will be resolved in minutes, not weeks. Clinical notes will write themselves. Denials will be prevented before claims are submitted. Care transitions will be orchestrated seamlessly across providers. And patients will communicate with their health system as easily as they message a friend.
This is not science fiction. The technology exists today, the regulatory environment is aligning, and the workforce crisis makes it necessary. The question for healthcare leaders is not whether agentic AI will transform these workflows. But whether your organization will be leading the transformation or scrambling to catch up.
Organizations that deploy agentic AI across these five workflows in 2026-2027 will establish operational efficiencies and patient experience standards that late adopters will struggle to match.
Ready to deploy AI agents in your healthcare workflows? Explore our Agentic AI for Healthcare services to see what autonomous automation can do. We also offer specialized Healthcare Software Product Development services. Talk to our team to get started.
Related reading
For more insights, explore our guides on 5 healthcare AI agent failures and lessons and Agent prompt-engineering patterns for healthcare.
You may also find value in what AI agents do in healthcare and FHIR in Modern Healthcare.