HIMSS 2025 in Las Vegas was the conference where healthcare AI stopped being a future promise and became a present-tense engineering problem. Over 40,000 attendees, 1,300+ exhibitors, and a theme that kept surfacing in every keynote, breakout, and vendor booth: agentic AI is here, but most health systems are not ready for it.
This is not a recap of who had the best booth or which keynote got the most applause. This is a technical analysis of what HIMSS25 revealed about the state of AI in healthcare — what is real, what is marketing, and what you need to build before any of it matters.
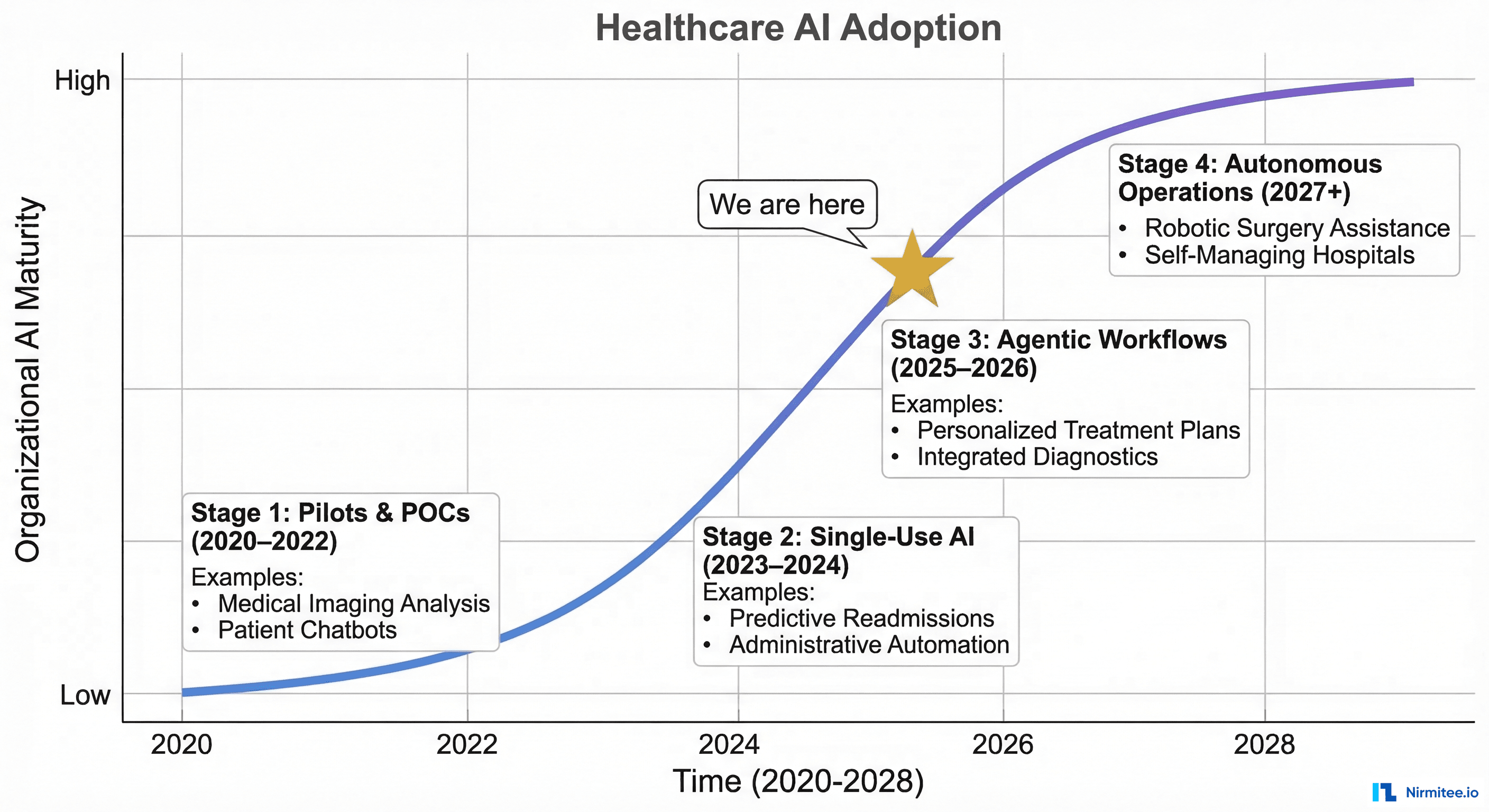
The Big Shift: From Assistive AI to Agentic AI
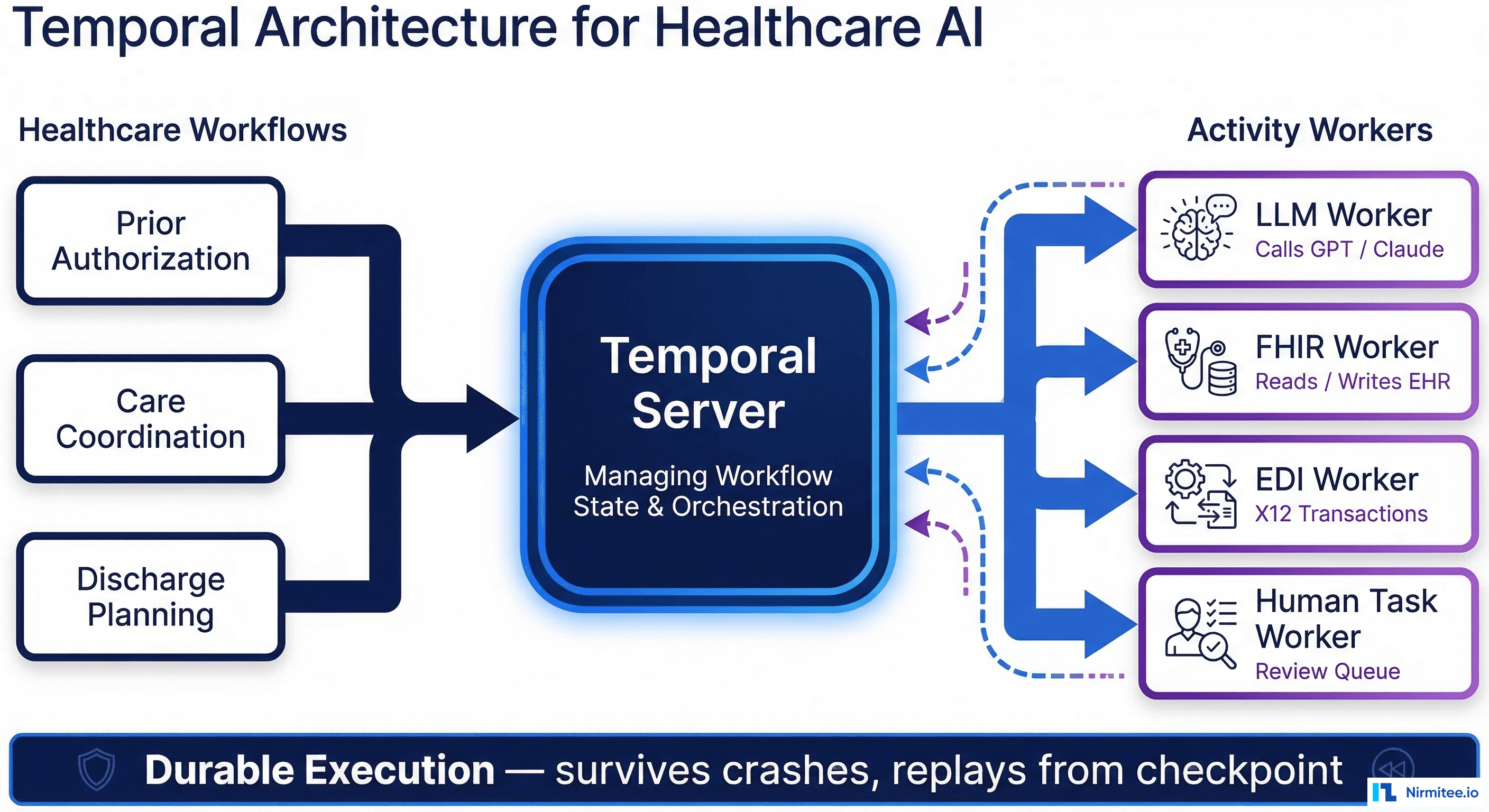
At HIMSS24, the dominant AI narrative was assistive: summarize this note, answer this question, suggest this code. At HIMSS25, the conversation shifted to agentic: AI systems that take multi-step actions, make decisions within defined boundaries, and complete entire workflows with minimal human intervention.
The difference is not semantic — it is architectural. An assistive AI tool calls one model, returns one response, and waits for the next human instruction. An agentic system orchestrates multiple models, calls external APIs, manages state across a workflow, and makes branching decisions based on intermediate results. The engineering complexity is an order of magnitude higher.
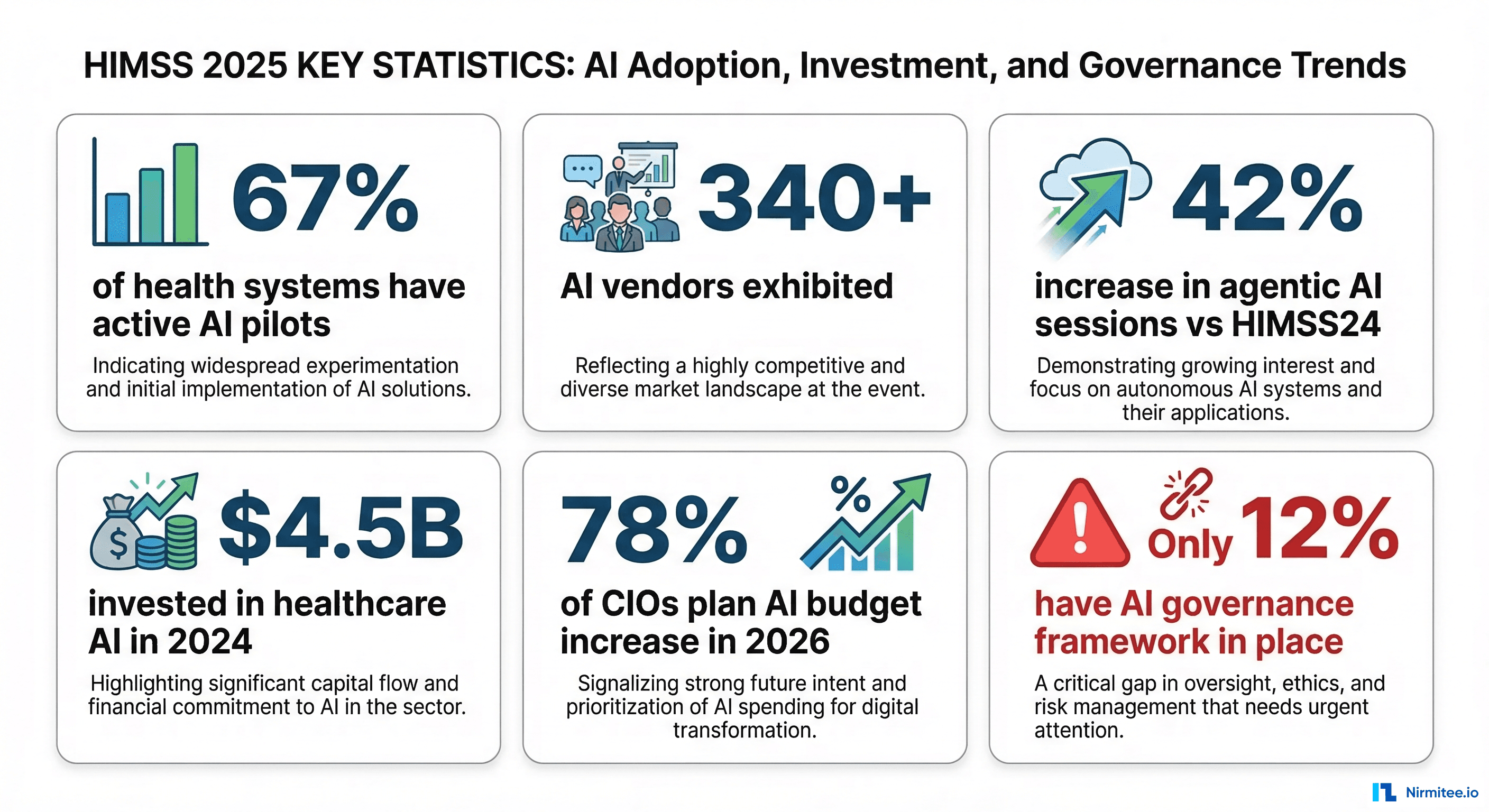
The data supports the shift. According to presentations at HIMSS25:
- 67% of health systems now have at least one active AI pilot program (up from 43% at HIMSS24)
- 42% increase in conference sessions explicitly focused on agentic AI compared to the previous year
- $4.5 billion was invested in healthcare AI companies in 2024, with CB Insights reporting that autonomous workflow tools received the largest share
- 78% of CIOs surveyed at the event plan to increase AI budgets in 2026
- But only 12% have a formal AI governance framework in place — the gap between adoption ambition and organizational readiness is enormous
Five Technologies That Dominated the Exhibition Floor
1. Ambient Clinical Documentation
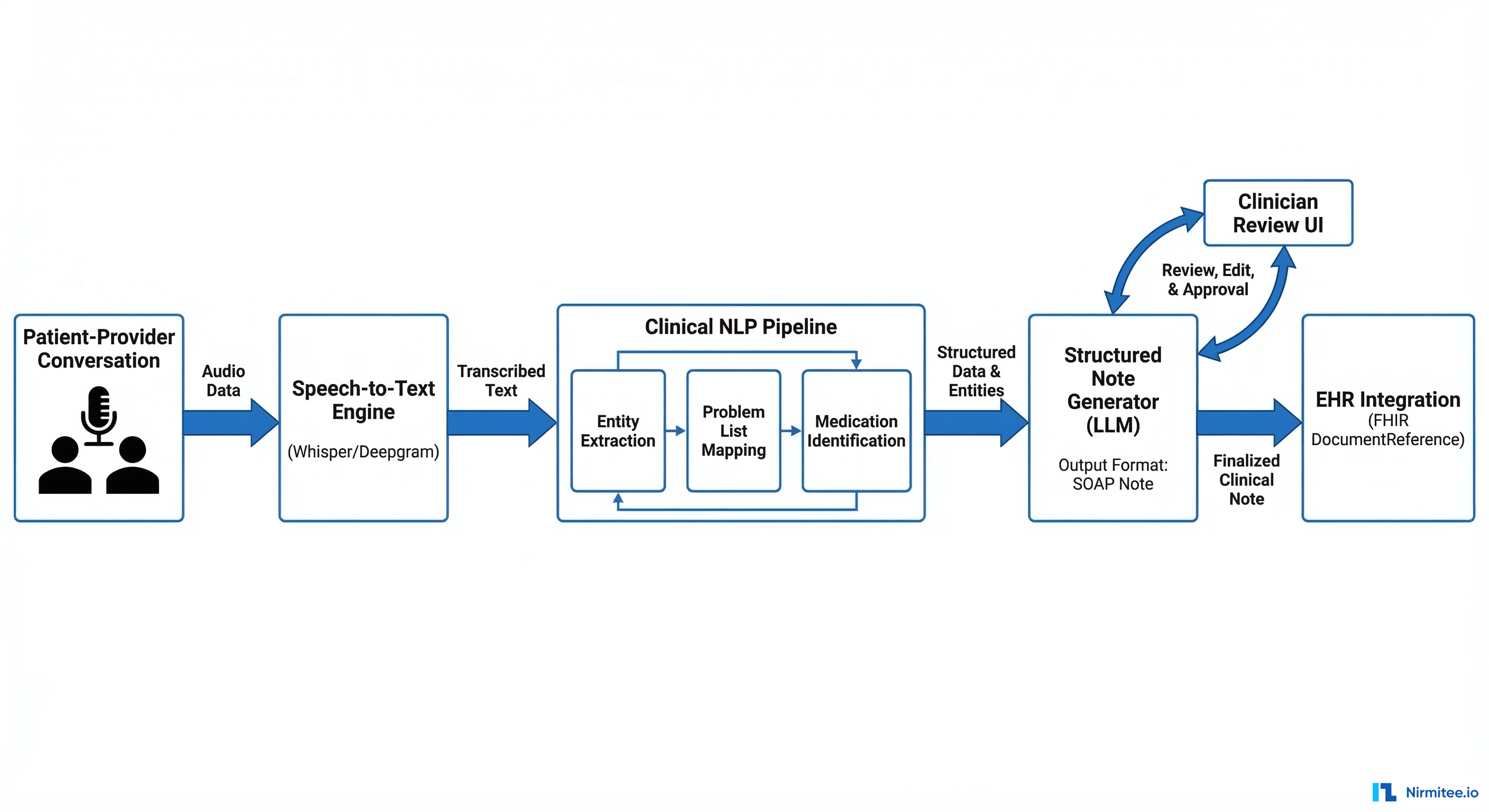
Every major EHR vendor and at least 30 startups were demonstrating ambient documentation — AI systems that listen to patient-provider conversations and automatically generate clinical notes. Microsoft's DAX Copilot (integrated into Epic and Oracle Health), Abridge, Suki, and DeepScribe were the most prominent players.
 EHR integration" width="1200" />
EHR integration" width="1200" /> The technology works. In demos, ambient scribes produced SOAP notes that were 85-90% accurate after a 10-minute patient encounter. The engineering challenge is not accuracy — it is integration. Getting a generated note into the EHR's documentation workflow, mapped to the correct patient and encounter, with the right SNOMED/ICD codes attached, and flagged for physician review before signing — that requires deep EHR integration that most startups are still building.
The impact data presented at HIMSS25 was compelling: organizations reporting 40-60% reduction in documentation time per encounter, with physician satisfaction scores improving by 25-30 points on post-implementation surveys. Documentation burden is the #1 driver of physician burnout — this technology directly addresses it.
2. Prior Authorization Automation
The CMS-0057-F rule mandating FHIR-based prior authorization APIs by January 2027 was a constant reference point. Vendors demonstrating PA automation fell into two camps: those building on the Da Vinci Prior Authorization Support (PAS) Implementation Guide, and those using LLM agents to extract clinical evidence from patient records and auto-populate PA forms.
The most technically impressive demonstrations showed multi-agent systems that could: read the payer's PA requirements, extract relevant clinical data from the patient's FHIR record, assemble the supporting documentation, submit the PA request via X12 278 or FHIR Claim, and track the response — all without human intervention for routine cases. For complex cases, the system flagged them for clinical review with the evidence already organized.
3. AI-Powered Revenue Cycle Management
Revenue cycle was the sleeper topic at HIMSS25. Multiple vendors demonstrated AI agents that could: predict claim denial probability before submission, automatically correct coding errors, generate appeal letters for denied claims with clinical evidence attached, and identify undercoded encounters where additional revenue was justified.
The ROI numbers presented were striking: 15-25% reduction in denial rates, 40% faster appeal processing, and $2-5M annual revenue recovery for mid-size health systems. The economics of healthcare AI agents are most compelling in revenue cycle because the value is directly measurable in dollars.
4. Clinical Decision Support 2.0
Traditional CDS (drug interaction alerts, dosage checks) has been in EHRs for years. HIMSS25 showcased the next generation: AI-driven CDS that combines rules engines with ML prediction models and LLM reasoning. The most discussed use cases were sepsis early warning (ML models achieving 0.89+ AUROC), AKI prediction, and diagnostic support for rare conditions.
The alert fatigue problem was explicitly acknowledged in multiple sessions. The consensus: effective CDS in 2026 means fewer, better alerts — not more alerts. Organizations that reduced low-value alerts by 50-60% saw 3x improvement in clinician action rates on remaining alerts.
5. Interoperability Infrastructure for AI
A recurring theme: AI is only as good as the data it can access. Multiple sessions focused on the data infrastructure prerequisites for healthcare AI — FHIR R4 APIs, real-time ADT/ORU feeds, clinical data warehouses, and de-identification pipelines for AI training data. Organizations that invested in interoperability infrastructure in 2023-2024 are now deploying AI agents. Organizations that skipped that investment are stuck in pilot purgatory.
The Governance Gap: The Elephant in Every Room
The most sobering finding from HIMSS25: the gap between AI adoption and AI governance. While 67% of health systems have active AI pilots, only 12% have a formal governance framework that covers model validation, bias testing, adverse event reporting, and regulatory compliance.
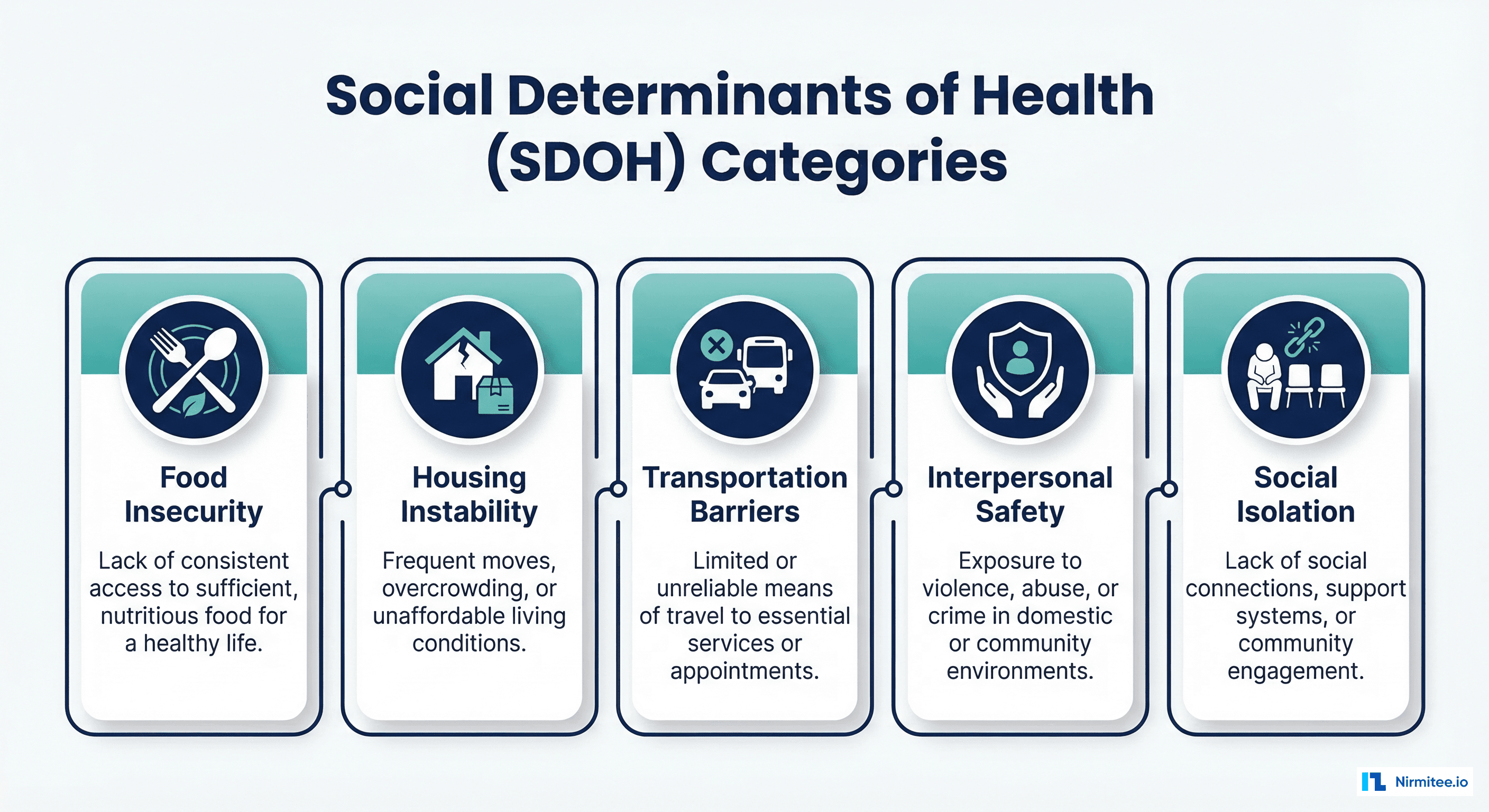
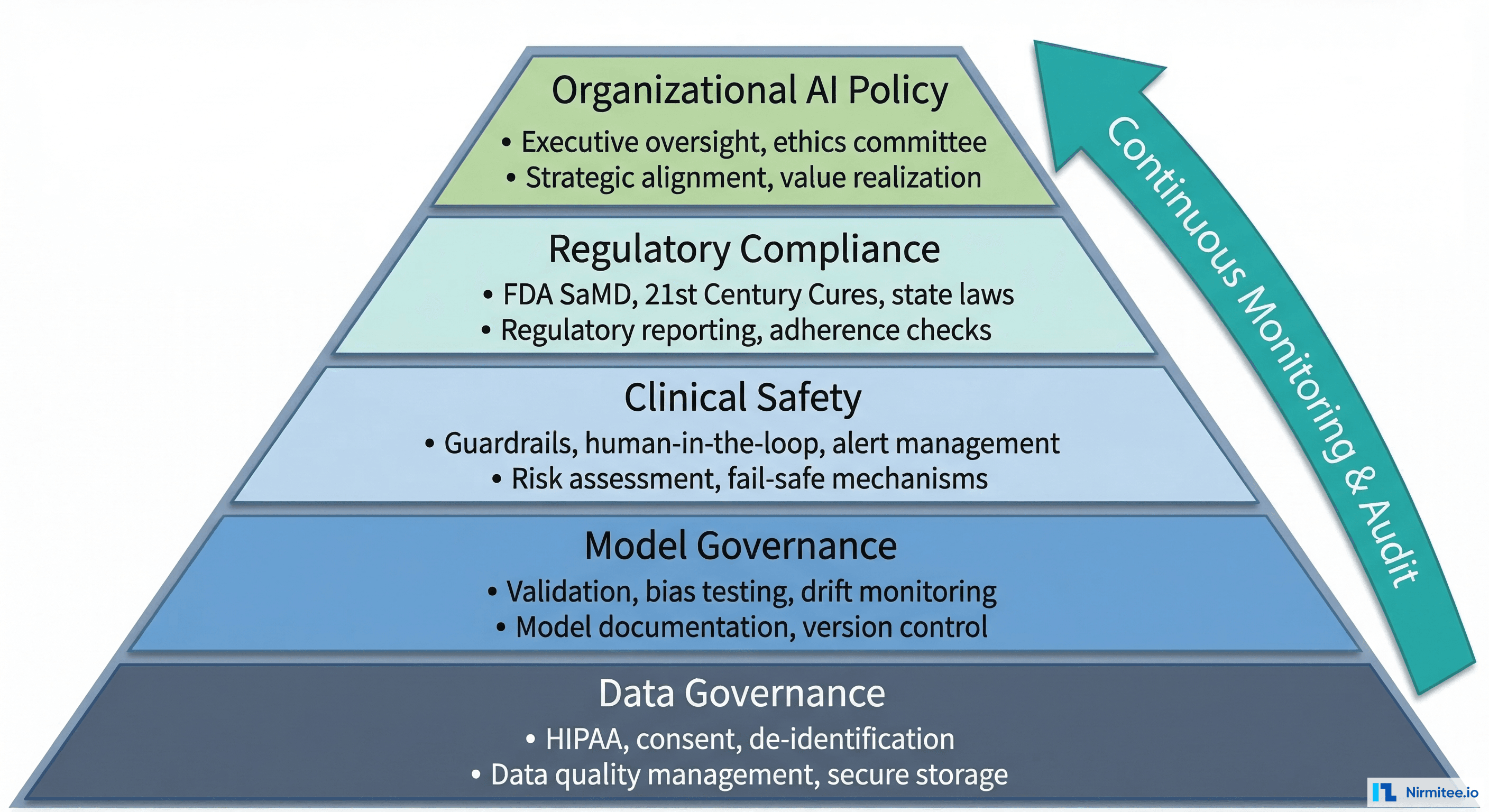
The governance sessions at HIMSS25 converged on a five-layer framework:
- Data Governance: HIPAA compliance, patient consent for AI use, de-identification standards, and data quality requirements
- Model Governance: Validation protocols before deployment, bias testing across patient demographics, ongoing evaluation suites, and drift monitoring
- Clinical Safety: Safety guardrails, human-in-the-loop policies, adverse event detection and reporting
- Regulatory Compliance: FDA SaMD classification, 21st Century Cures Act exemptions, state-level AI regulations (Colorado, California, and Connecticut are leading)
- Organizational Policy: Executive oversight committee, AI ethics guidelines, vendor evaluation criteria, and transparency requirements
Health systems that establish governance frameworks now will move faster on AI adoption in 2026-2027. Those that skip governance will face the same problem every technology adoption cycle produces: a proliferation of ungoverned AI tools that create compliance exposure and interoperability headaches.
What This Means for Healthcare Builders
If you are building healthcare applications in 2026, HIMSS25 surfaced three strategic imperatives:
1. Build the data foundation first. Every successful AI deployment at HIMSS25 was built on a solid data layer — FHIR R4 APIs, real-time clinical data feeds, and structured data pipelines. If your application cannot access patient data in real-time via FHIR, AI features will be limited to batch processing on stale data. FHIR-based AI/ML pipelines are the prerequisite, not the end goal.
2. Design for human-in-the-loop from day one. The most credible AI demonstrations at HIMSS25 explicitly showed where humans stayed in the loop. The most criticized ones claimed "fully autonomous" operation. In healthcare, human-in-the-loop is not a compromise — it is the architecture that earns clinical trust and regulatory approval.
3. Governance is a competitive advantage, not a burden. Health systems are beginning to require AI governance documentation from their vendors. If your product cannot demonstrate model validation protocols, bias testing results, and audit trail completeness, you will lose deals to competitors that can. Build governance into your product, not your pitch deck.
Ready to deploy AI agents in your healthcare workflows? Explore our Agentic AI for Healthcare services to see what autonomous automation can do. We also offer specialized Healthcare AI Solutions services. Talk to our team to get started.
Frequently Asked Questions
What was the biggest AI announcement at HIMSS 2025?
No single announcement dominated, but the most discussed development was the proliferation of agentic AI systems for revenue cycle and prior authorization workflows. The shift from "AI that assists" to "AI that acts" was the defining theme across vendors, sessions, and keynotes.
Is ambient clinical documentation ready for production?
Yes, for specific use cases. Ambient documentation for primary care encounters (straightforward SOAP notes) is production-ready from multiple vendors. Specialty-specific workflows (surgery, complex procedures, multi-disciplinary rounds) remain challenging due to medical terminology complexity and multi-speaker environments.
When will AI replace clinicians?
It will not. This question was directly addressed in multiple keynotes. AI in healthcare augments clinical decision-making — it does not replace it. The most effective implementations give clinicians better information faster, reduce administrative burden, and flag risks earlier. The clinician remains the decision-maker.
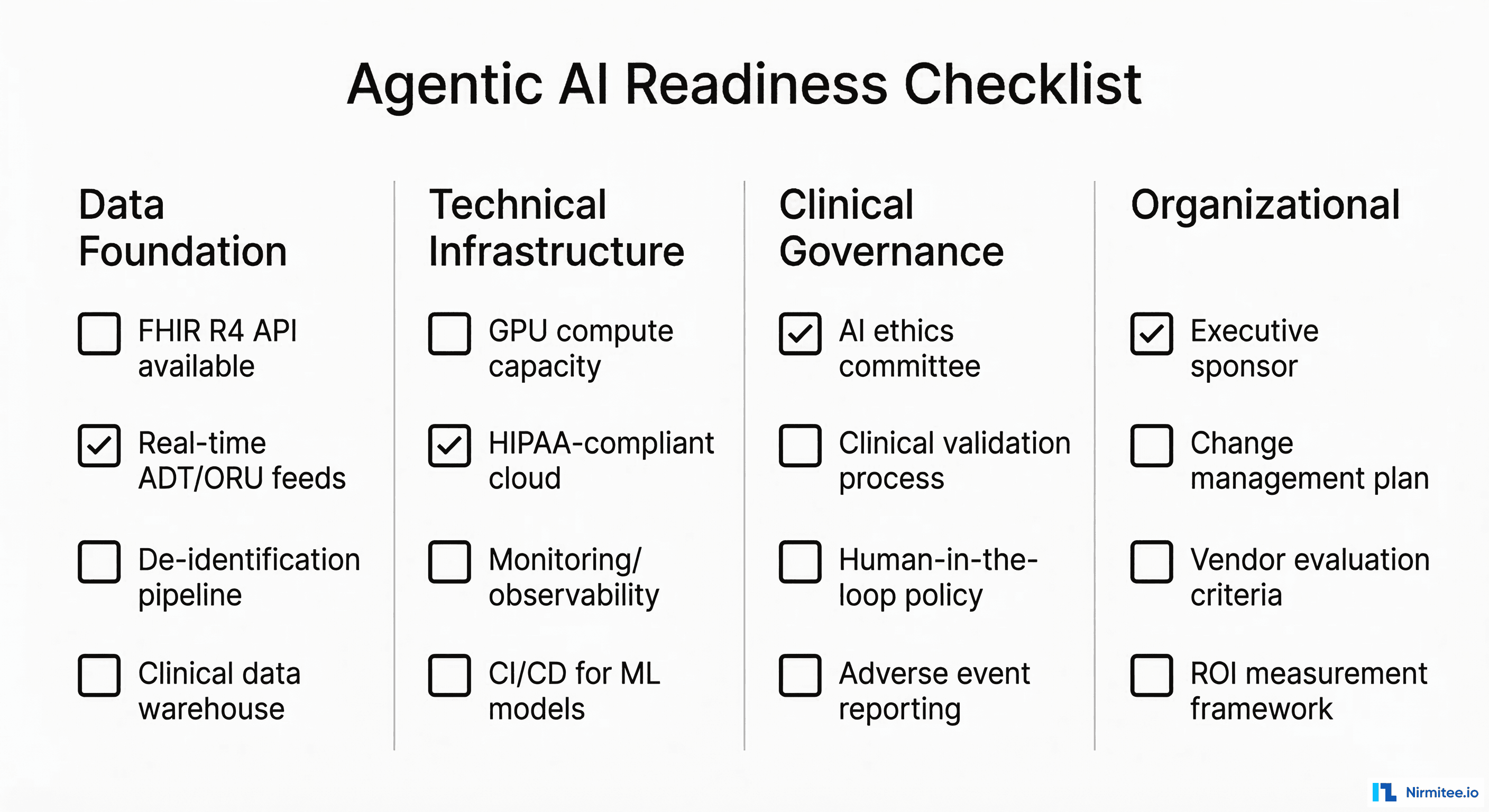
What should health systems prioritize for AI readiness in 2026?
In order: (1) FHIR R4 API availability and real-time data feeds, (2) AI governance framework, (3) single high-value AI use case (ambient documentation or prior auth automation), (4) monitoring and evaluation infrastructure. Do not attempt five AI initiatives simultaneously — pick one, prove value, then expand.
HIMSS25 made one thing clear: the healthcare organizations that will lead in AI are not the ones with the most pilots — they are the ones with the strongest data foundations, governance frameworks, and engineering discipline. At Nirmitee, we build the infrastructure layer that makes healthcare AI possible — FHIR integration, EHR connectivity, and HIPAA-compliant AI architecture. If you are building for 2026, let us talk.