The implementation challenge: deploy without taking critical care offline
Implementing RFID asset tracking in a large hospital is not a software project — it's a 16-week operational change touching every department. The temptation is to deploy fast, hospital-wide, in a single sprint. The result is usually disruption to clinical operations and rejection by ward staff.
This guide walks through a phased deployment plan that has been refined across 12 large hospital deployments. The principle: low-risk departments first, ICU and OT last, never simultaneously.
Phase 1 — Foundation (weeks 1-4)
The pre-deployment phase. Four parallel work streams:
- Asset register cleanup: a physical inventory walk-through. The existing register is reconciled to physical reality before tagging starts. Most hospitals discover 5-12% variance — the cleanup cycle takes 2-3 weeks.
- Hardware procurement: printers, RFID tags, readers, antennas, network switches. The procurement cycle in India typically takes 4-6 weeks; start ordering in Phase 1 even though installation isn't until later.
- Network design: dedicated PoE switch for asset tracking, antenna placement floor plan, RF interference survey.
- Biomedical training: the biomedical team must own the system. 8-12 hours of structured training in Phase 1 prevents the most common adoption failures later.

Phase 2 — Pilot (weeks 5-8)
100 assets across 2 departments. Recommended pilot departments: central stores (low risk, high asset count) and biomedical workshop (high control over the environment). Pilot objectives:
- Validate RFID scan accuracy (target: 98%+ across all reader-tag combinations).
- Confirm portal reader and ceiling antenna placement covers the actual asset paths.
- Test the asset management software integration with HIS / ERP.
- Establish daily / weekly operational rhythms — who does what, when.
Pilot success criteria are non-negotiable. If scan accuracy is below 98% at end of pilot, do not proceed to Phase 3 — fix the pilot environment first.
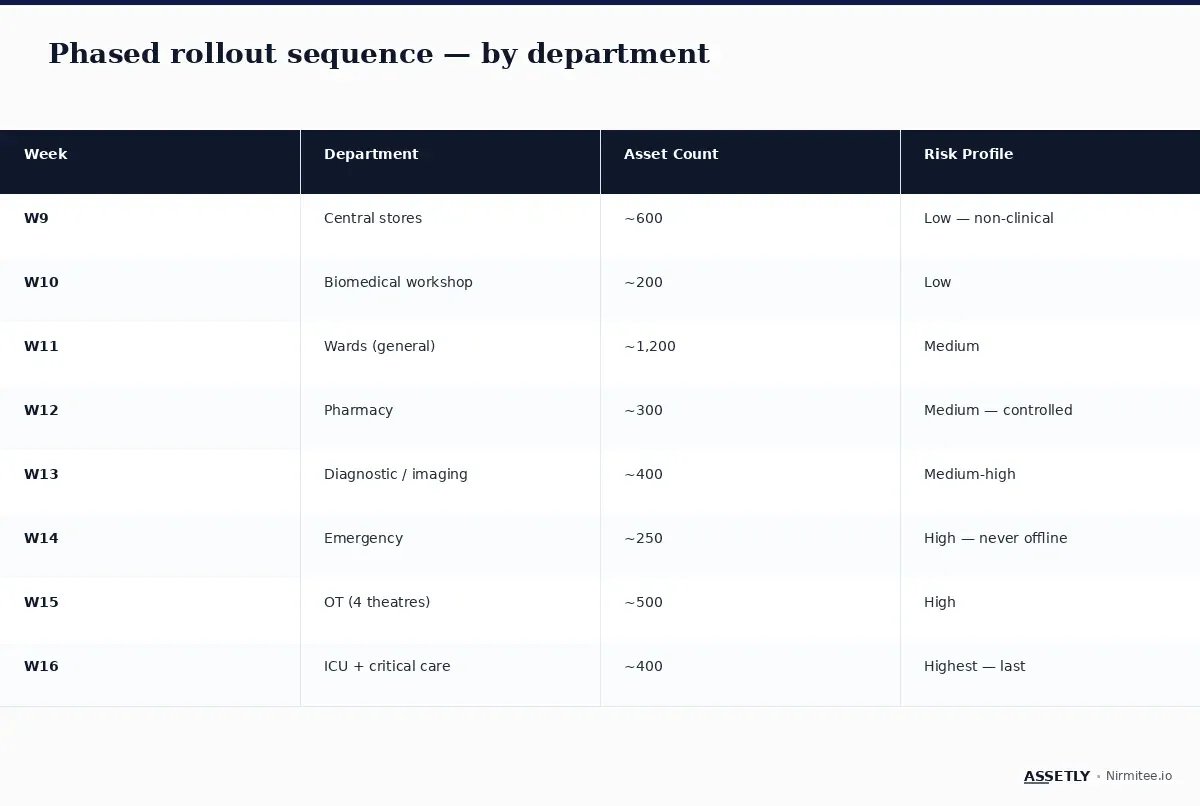
Phase 3 — Phased rollout (weeks 9-12)
Department-by-department, low-acuity first. The sequence is critical:
- Week 9: Central stores (~600 assets, low clinical risk).
- Week 10: Biomedical workshop (~200 assets, full team control).
- Week 11: General wards (~1,200 assets, medium risk).
- Week 12: Pharmacy + diagnostic / imaging (~700 assets combined).
Each department gets 1-2 days of on-site biomedical support during go-live, then daily check-ins for the first week. By end of Phase 3, roughly 60-70% of the asset base is on the system.
Phase 4 — Stabilisation + optimisation (weeks 13-16)
The high-risk departments — emergency, OT, and ICU — go last. Why: these departments cannot tolerate deployment disruption. By Phase 4, the deployment team has already learned every operational quirk on lower-risk departments. Phase 4 deployment goes faster and cleaner.
- Week 13: Diagnostic and imaging (~400 assets).
- Week 14: Emergency (~250 assets — never goes offline; tag during shift handovers).
- Week 15: OT (4 theatres, ~500 assets — tag between scheduled cases).
- Week 16: ICU and critical care (~400 assets — tag bed-by-bed during patient transfers).
By end of Phase 4, the entire hospital is on the system. The first quarterly audit cycle runs in week 17-18 and validates the deployment.
Common pitfalls to avoid
- Deploying ICU first — guaranteed to fail. ICU staff are stretched, intolerant of disruption, and need the deployment to be already-proven before they engage.
- Skipping the asset register cleanup — tagging on a dirty register propagates the existing data quality issues.
- Insufficient biomedical training — the team must be the SMEs by Phase 2, not Phase 4.
- Sharing the network with patient monitoring — RFID packet bursts affect QoS. Use a dedicated PoE switch.
- Not running the walk test — every reader must be validated with a 50-tag walk through every angle before sign-off.
Real-world: a 1,000-bed hospital's clean deployment
A 1,000-bed multispecialty hospital in Bangalore deployed Assetly RFID on 6,200 assets in 18 weeks (slightly over plan due to one antenna repositioning). Pilot scan accuracy was 99.1%. Departmental rollout completed without operational disruption to any clinical service. First audit cycle (week 19) reconciled at 99.6% — the highest rate in the hospital's history.
Resource requirements for a 500-1,000 bed deployment
- Internal team: 1 biomedical lead (dedicated), 2 biomedical engineers (50% time), 1 IT lead, 1 procurement lead.
- External team: deployment partner (Assetly + integrator) for the full 16 weeks.
- Time investment: roughly 320-480 internal hours over 16 weeks.
Key takeaways
- 16-week phased deployment is the operational standard for large hospitals.
- Asset register cleanup must precede tagging — don't tag a dirty register.
- Pilot 100 assets in 2 low-risk departments before any wider rollout.
- ICU and OT go last, not first. Deploy after all the operational quirks are learned.
- RFID network must be dedicated, not shared with patient monitoring.
- Validate every reader with a 50-tag walk test.
Planning a hospital RFID deployment?
Get the sequencing right and the program runs smoothly for years. Read our pillar guide, or talk to the Assetly team about a 16-week deployment plan tailored to your hospital.