The list every hospital manager wants
"What can an AI agent actually do in my hospital today?" — the question we get most often. The answer is concrete, ranked, and shippable. Each of the workflows below has a published reference architecture, an established baseline metric, and a documented playbook for getting to production in under six months. None of them require FDA clearance for the typical scope. None of them displace clinical judgment.
This is the actionable companion to our pillar guide on AI agents in healthcare. For the strategic context, see top use cases of AI agents in healthcare; for the dollar-level math, see where AI agents deliver ROI in healthcare.
The 10 workflows
01 — Patient intake (Operations)
Conversational intake across web, SMS, or voice. Demographics, visit reason, insurance, consent — captured and validated before the patient arrives. Front-desk time per patient drops from 12 minutes to 3 minutes of staff review. Build path: how to build an AI agent for patient intake automation.
02 — Eligibility verification (RCM)
Real-time 270/271 transactions with carrier mapping. Coverage gaps surface at scheduling, not after the visit. Average response under 30 seconds. Reference: eligibility verification AI agent in 30 seconds.
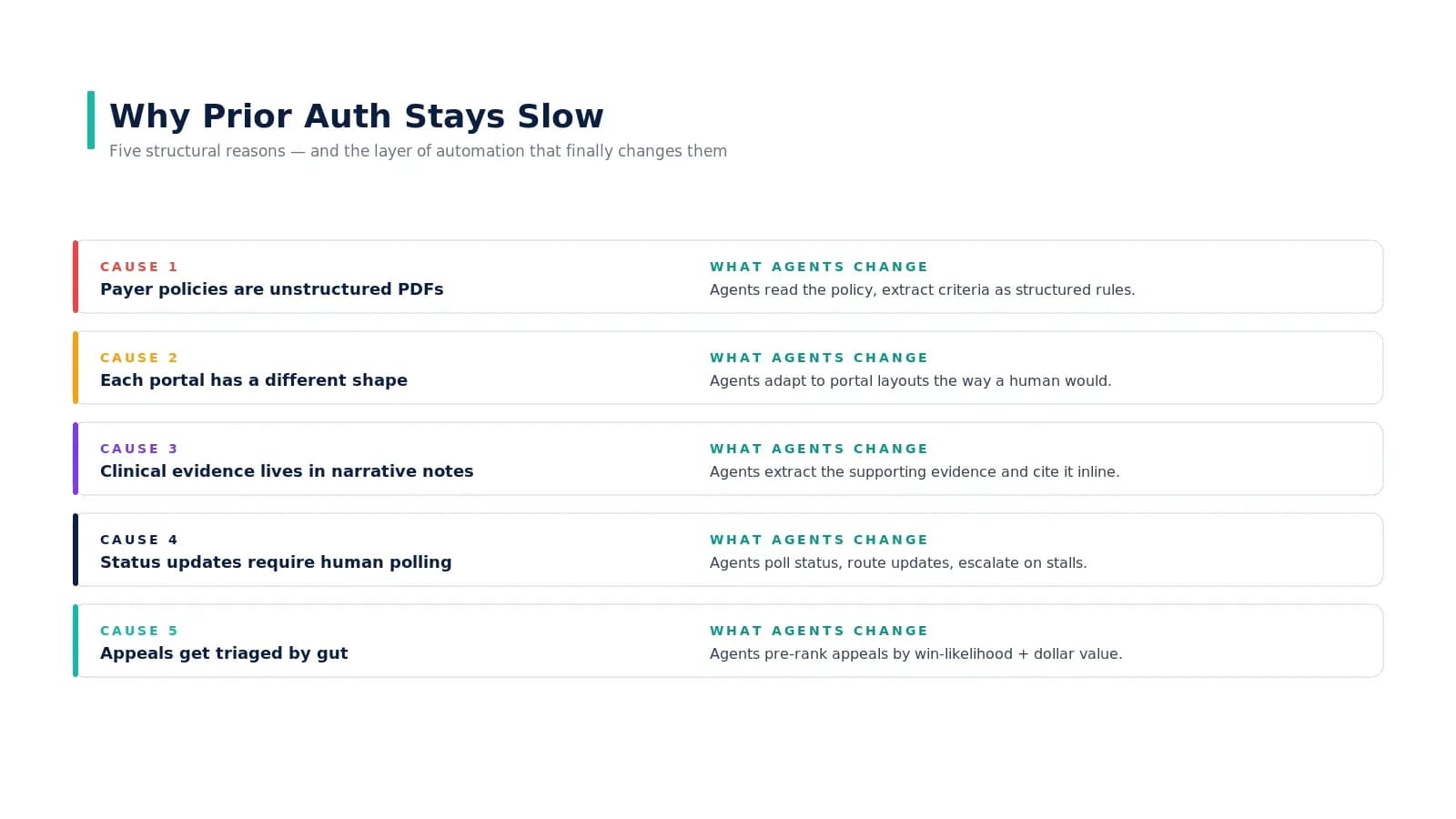
03 — Prior authorization submission (RCM)
End-to-end PA: chart read, payer policy mapping, justification draft, portal submission, status tracking, appeal drafting. Cycle time from 5 days to single-digit hours. See why prior authorization is broken for the full pattern.
04 — Claim scrubbing (RCM)
Pre-bill validation: codes against clinical notes, payer-specific edits, documentation gap detection. First-pass denial rate drops 25–40% in the first six months.
05 — Denial appeal drafting (RCM)
The agent reads the EOB, ranks denials by win-likelihood and dollar value, retrieves chart evidence, and drafts the appeal letter. Biller reviews and submits. Appeal win rate climbs because effort concentrates on winnable cases.
06 — Ambient SOAP documentation (Clinical)
Encounter audio captured by an ambient device → structured SOAP note draft → physician sign-off. After-hours documentation drops 40%. Note quality improves because the agent captures the full encounter.
07 — Care-gap outreach (Population Health)
Risk-rank attributed patients, identify care gaps (overdue screenings, lapsed refills), trigger appropriate outreach (SMS for routine, coordinator escalation for complex). Coordinator capacity 3x what it was.
08 — Refill coordination (Clinical)
Detect lapses in chronic medication refills, contact the patient to confirm, route to the pharmacy. Lapse rate drops ~18%. Particularly valuable in chronic care and post-discharge.
09 — Wait-list backfill (Access)
Match cancellations to a ranked wait-list — clinical urgency, provider preference, patient availability — without a scheduler making manual calls. Schedule utilization climbs ~22%.
10 — Discharge instructions (Clinical)
Generate personalized discharge instructions from the chart, in the patient's language and reading level, for clinician review and sign-off. Average 12 minutes saved per discharge; readmission rates trend favorably (the causal claim requires more rigorous study).
How to sequence the first three
Most hospitals win by stacking adjacent RCM agents in this order:
- Months 1–3 — Eligibility. The cleanest possible first agent. Bounded data, large dollar impact, low clinical risk. Output: real-time 270/271 with carrier mapping and proactive alerts.
- Months 3–5 — Prior authorization. Builds on cleaner eligibility data. The PA workflow now starts with confirmed coverage rather than uncertain coverage.
- Months 5–7 — Claim scrubbing. Builds on both upstream agents. By the time the claim is scrubbed, eligibility is confirmed and PA is in place — the scrubber surfaces only the genuinely fixable issues.
The 30 / 60 / 90-day starter plan
For the first workflow:
Days 0–30: Design
Pick ONE workflow. Set baseline metric. Confirm BAA and EHR access. Conduct 5 stakeholder interviews. Establish a 30-day baseline log. Brief CFO and CMIO. Exit gate: approved use case + baseline.
Days 31–60: Build
Shadow the agent on production data. Compare against humans. Draft governance. Run accuracy check on 200 cases. Conduct bias audit. Update risk register. Exit gate: >95% accuracy or rollback.
Days 61–90: Deploy
Supervised go-live. Define rollback trigger. Track KPI vs baseline. Run 30-day production review. Clinical safety committee review. Exit gate: sustained KPI improvement.
The exit gate after each block is the operating discipline that distinguishes scaled deployments from stalled pilots. Skip a gate, you accumulate technical and operational debt that surfaces six months later as "why isn't this working at scale?"
What about the workflows not on this list?
Diagnosis from imaging, autonomous medication titration, unsupervised triage to high-acuity beds, open-ended patient counseling — see where AI agents deliver ROI in healthcare for the honest counter-cases. The math and the risk profile do not yet support them; revisit as FDA pathways and payer codes evolve.
Real-world examples behind these workflows
Each workflow on this list has at least one publicly documented production deployment grounding the impact estimates: Mayo Clinic on patient access and revenue cycle automation, Geisinger on eligibility verification, Mass General Brigham on ambient SOAP documentation, Kaiser Permanente on the early-warning system that saves an estimated 500 lives per year, and Banner Health on denial management. The metric ranges associated with each workflow above are calibrated against those public outcomes plus patterns observed across Nirmitee deployments — they are achievable, not aspirational.
Key takeaways
- Start with eligibility verification. Bounded data, large dollar impact, low clinical risk, fast payback.
- Stack adjacent RCM agents. Eligibility → PA → claim scrubbing — each agent makes the next one easier.
- Run the 30/60/90 plan. Design → build → deploy with explicit exit gates between each block.
- Build a platform, deploy specialized agents on top. Identity, FHIR client, audit, and observability are shared; prompts and validation are workflow-specific.
- The first workflow takes 90 days; the third takes 45. The platform compounds; budget the ROI accordingly.
Want to deploy an AI Agent inside your hospital or healthcare product? Get in touch with our team — we will scope the workflow, governance, and 90-day rollout plan against your own baseline metrics.
Learn more about AI Agents in Healthcare → read the full pillar guide.
Related reading: