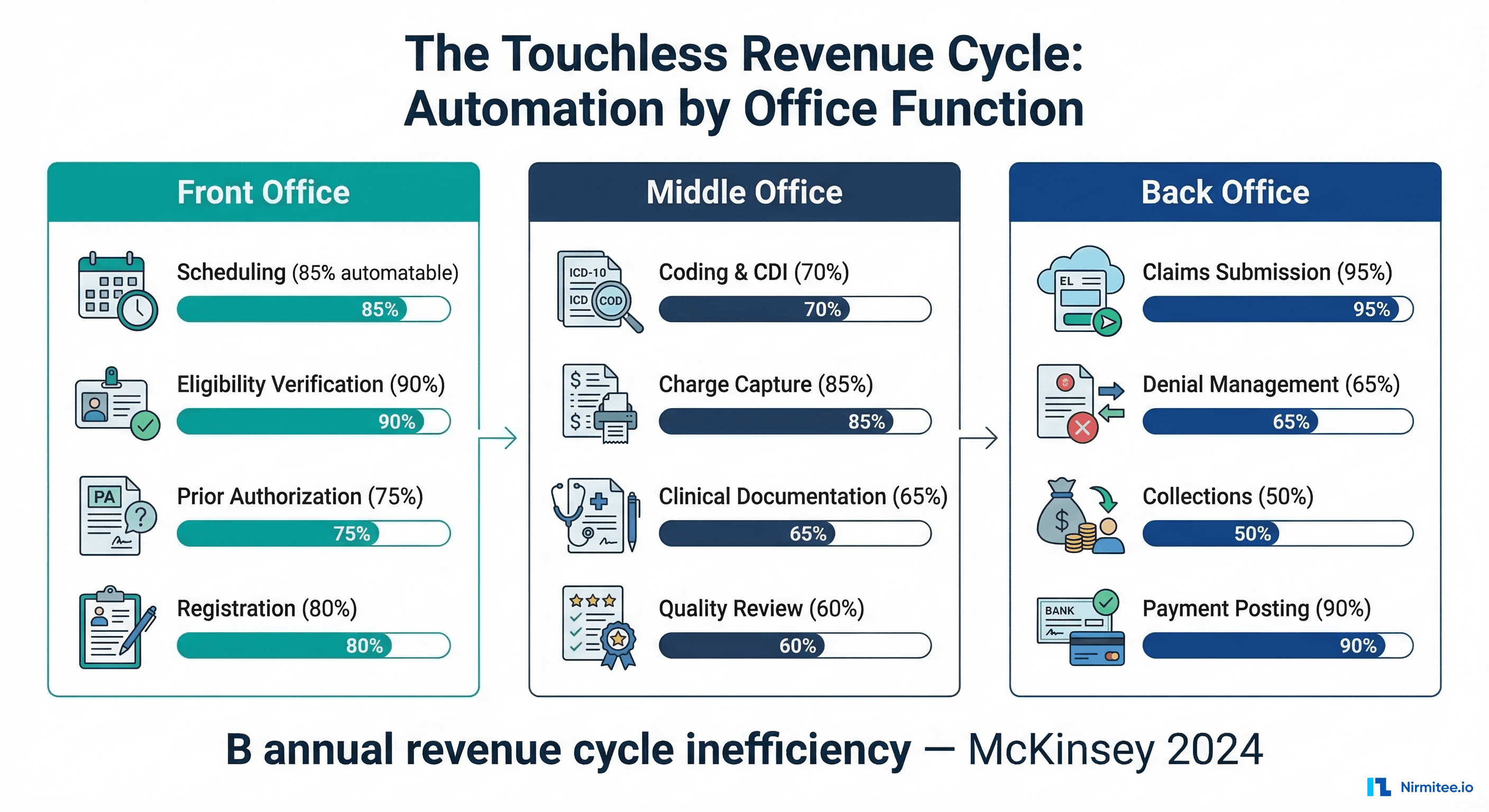
The US healthcare revenue cycle wastes $262 billion annually. That's not a projection — it's the measured cost of manual processes, denied claims, rework, and collections overhead that persists across nearly every health system in the country. McKinsey's landmark 2024 healthcare revenue cycle report quantified what operators have known for years: the revenue cycle is the largest operational cost center in healthcare, and the majority of it is automatable.
But "automatable" doesn't mean "automated." Most health systems still operate revenue cycles built on human labor, manual verification, and reactive workflows. The McKinsey framework breaks this down into three offices — front, middle, and back — each with distinct automation readiness profiles. This guide walks through each function, what's automatable now versus what requires a 2-3 year technology maturation, and the emerging vision of AI agent networks that could make the "touchless" revenue cycle a reality.
Over 30% of healthcare providers now rank AI investment in revenue cycle management as their top technology priority, according to Becker's Health IT 2025 survey. The question is no longer whether to automate — it's where to start and how fast to move.
Understanding McKinsey's Three-Office Framework
McKinsey's framework divides the revenue cycle into three functional offices, each with a distinct role in the patient financial journey:
- Front Office: Everything before the clinical encounter — scheduling, eligibility verification, prior authorization, patient registration, and financial counseling. This is where revenue cycle starts and where 30% of total RCM costs originate.
- Middle Office: Everything during and immediately after the encounter — medical coding, clinical documentation improvement (CDI), charge capture, and quality review. This is where clinical and financial data meet, and where 45% of denied claims originate.
- Back Office: Everything after coding — claims submission, remittance processing, denial management, appeals, patient collections, and bad debt recovery. This is where cash is collected and where days in accounts receivable (A/R) accumulate.
The insight from McKinsey's analysis is that automation maturity varies dramatically across these offices. Some functions are ready for near-complete automation today. Others require advances in clinical NLP, payer API standardization, or regulatory clarity before they can be reliably automated. Understanding this maturity gradient is essential for prioritizing investment.
Front Office Automation: The Fastest Wins
The front office offers the highest automation ROI with the lowest implementation complexity. Most front office functions are data-matching and verification tasks — exactly the kind of work that rules engines and API integrations handle well.
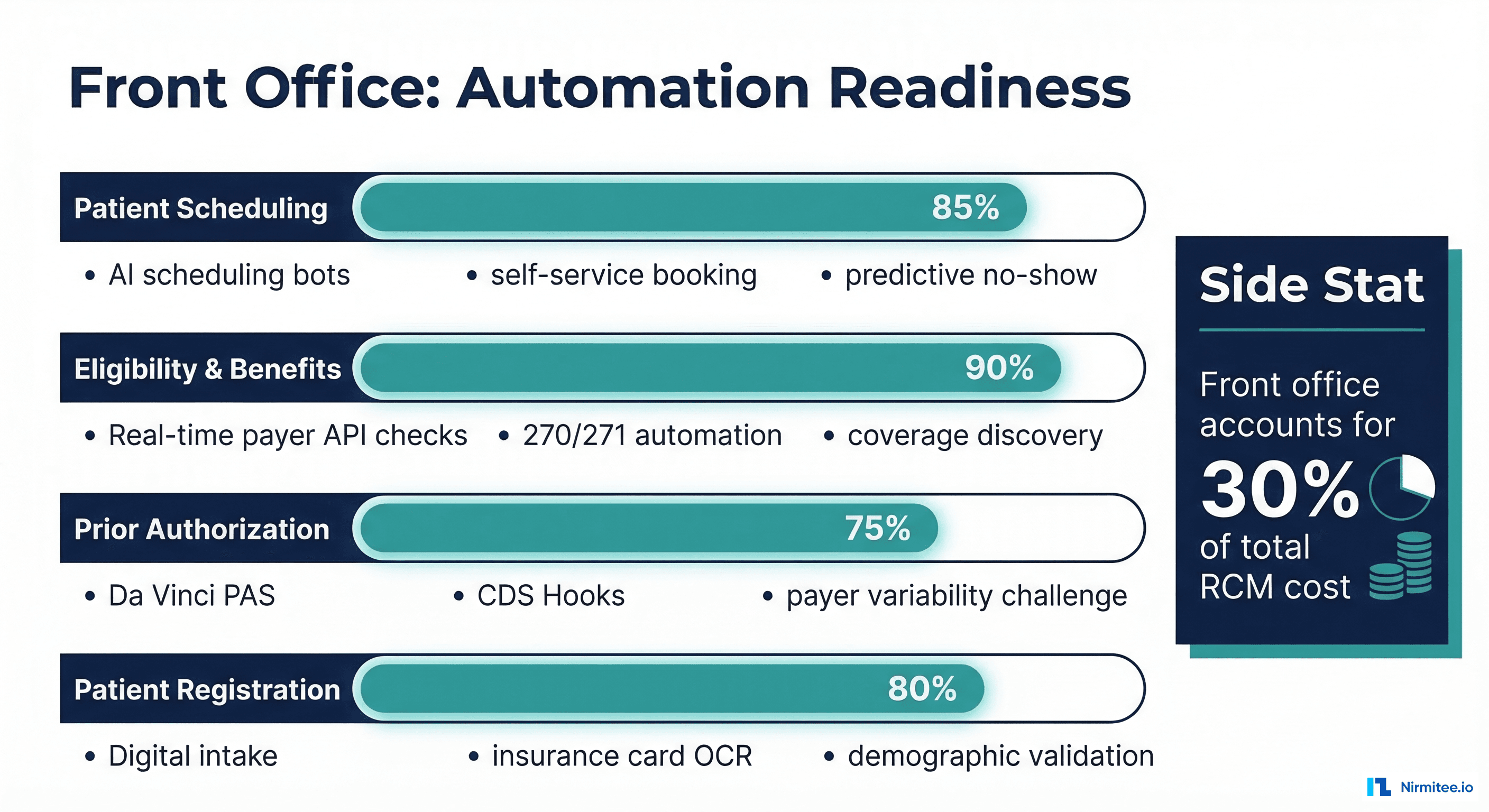
Patient Scheduling (85% Automatable)
Modern scheduling automation goes far beyond online booking. AI-powered scheduling systems analyze historical no-show patterns, provider preference data, and appointment type duration to optimize scheduling templates. Predictive models can identify patients likely to no-show and automatically overbooking slots or sending targeted outreach. Self-service booking portals integrated with insurance eligibility checks ensure patients are routed to in-network providers. The remaining 15% that resists automation: complex multi-visit scheduling for procedures requiring sequential appointments across departments, and accommodating patient preferences that don't fit templated slots.
Eligibility and Benefits Verification (90% Automatable)
This is the most automation-ready function in the entire revenue cycle. Real-time eligibility APIs (EDI 270/271) can verify coverage, copay amounts, deductible status, and out-of-pocket maximums in under 2 seconds. The technology is mature, payer APIs are standardized, and the ROI is immediate: eliminating eligibility-related denials (which account for 20-30% of all initial denials at most health systems) and reducing registration time by 60-70%. The remaining 10%: payer systems with API downtime, Medicaid programs with complex eligibility rules, and patients with multiple active coverage requiring coordination of benefits logic.
Prior Authorization (75% Automatable)
Prior authorization is the most painful front office function and the one most actively being targeted by regulation. The CMS Prior Authorization API mandate (effective January 2027) requires CMS-regulated payers to support FHIR-based electronic prior auth. For straightforward authorizations — standard imaging, common medications, routine procedures — automation can handle the complete submit-track-receive cycle. The challenge is the 25% of authorizations that require clinical justification, peer-to-peer reviews, or payer-specific documentation requirements that vary across thousands of health plans. This is where AI agents are making the most rapid progress.
Patient Registration (80% Automatable)
Digital patient intake has accelerated dramatically since COVID. Insurance card OCR extracts plan information from a phone photo. Demographic validation APIs verify addresses and identity. Pre-visit intake forms collect history and consent electronically. The automation gap: patients who arrive without ID, have complex insurance situations (Workers' Comp, auto accident liability, dual eligibility), or need interpreter services and accessibility accommodations that require human coordination.
Middle Office Automation: The Clinical-Financial Bridge
The middle office is where automation gets hard. These functions sit at the intersection of clinical medicine and financial operations — requiring understanding of both clinical documentation and payer billing rules. This is also where the highest-value automation opportunities exist, because middle office errors cascade into denials that cost 10-20x more to fix downstream.
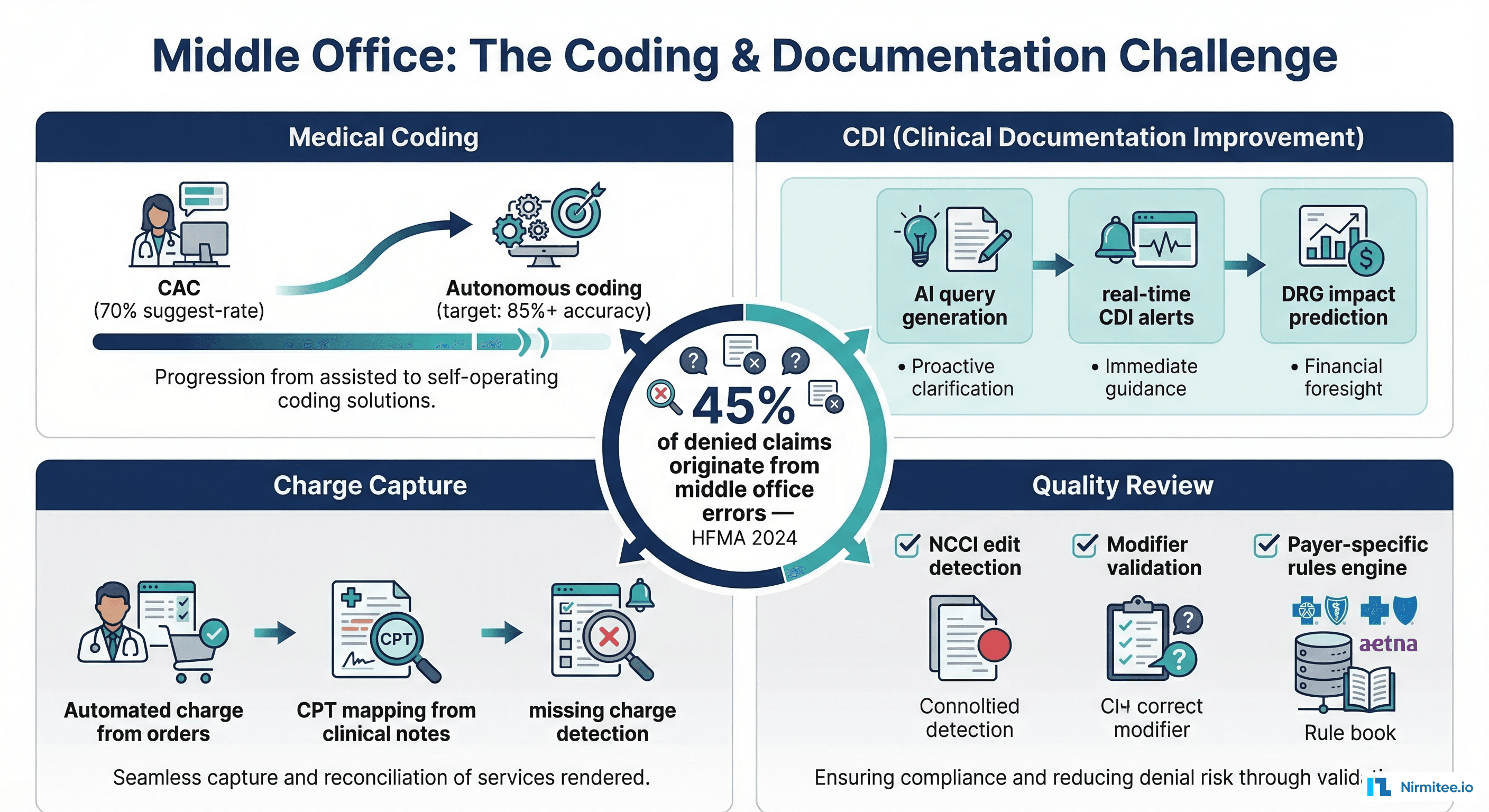
Medical Coding (70% Automatable)
Computer-Assisted Coding (CAC) has been in use for a decade, but accuracy rates have plateaued at 60-70% for automated code suggestion. The next generation of coding automation uses large language models trained on clinical documentation to suggest ICD-10-CM, CPT, and HCPCS codes with increasing accuracy. Current state-of-the-art systems achieve 85-90% accuracy on high-volume, straightforward encounters (office visits, routine labs). But complex inpatient stays, multi-system diagnoses, and procedures requiring modifier selection still need human coders for validation. The 2-3 year horizon: autonomous coding for 85%+ of outpatient encounters, with human review reserved for inpatient, surgical, and complex specialty coding. The bottleneck isn't AI capability — it's regulatory acceptance and payer audit risk tolerance.
Clinical Documentation Improvement (65% Automatable)
CDI programs ensure that clinical documentation supports the acuity, severity, and complexity of the patient's condition for accurate coding and reimbursement. Traditional CDI requires specialist nurses to review charts and query physicians for clarification. AI-powered CDI tools can: (1) identify documentation gaps in real-time during the encounter, (2) generate physician queries automatically when a diagnosis appears unsupported, (3) predict DRG (Diagnosis Related Group) impact based on documentation completeness, and (4) flag cases where documentation improvements could change reimbursement by $5,000+. The challenge: physician engagement. Even the best AI-generated CDI query is useless if the physician ignores it. The human element — CDI specialists building relationships with clinical teams — remains essential for the 35% of cases requiring physician behavior change.
Charge Capture (85% Automatable)
Charge capture — ensuring that every billable service rendered generates a corresponding charge — is highly automatable because it's fundamentally a matching problem. Automated charge capture systems monitor clinical orders, procedure completions, and supply usage, then generate charges based on rules. Missing charge detection algorithms compare expected charges (based on diagnosis, visit type, and procedure history) against actual charges and flag discrepancies. The remaining 15%: non-standard procedures, research protocol charges, and multi-department encounters where charge responsibility is ambiguous.
Quality Review and Compliance (60% Automatable)
Pre-bill quality review — checking coded claims against NCCI (National Correct Coding Initiative) edits, LCD/NCD medical necessity rules, and payer-specific billing rules — is largely rules-based and automatable. Claims scrubbing software has been doing this for 20 years. What's new: AI-powered tools that learn from denial patterns to predict which claims are likely to be denied before submission, allowing proactive correction. The gap: complex compliance scenarios involving anti-kickback, Stark Law, and medical necessity determinations that require clinical judgment.
Back Office Automation: Following the Cash
The back office handles the largest volume of transactions and has the most mature automation tooling. Electronic claims submission and remittance processing have been partially automated for decades via EDI. The new frontier is intelligent automation of denial management and patient collections.
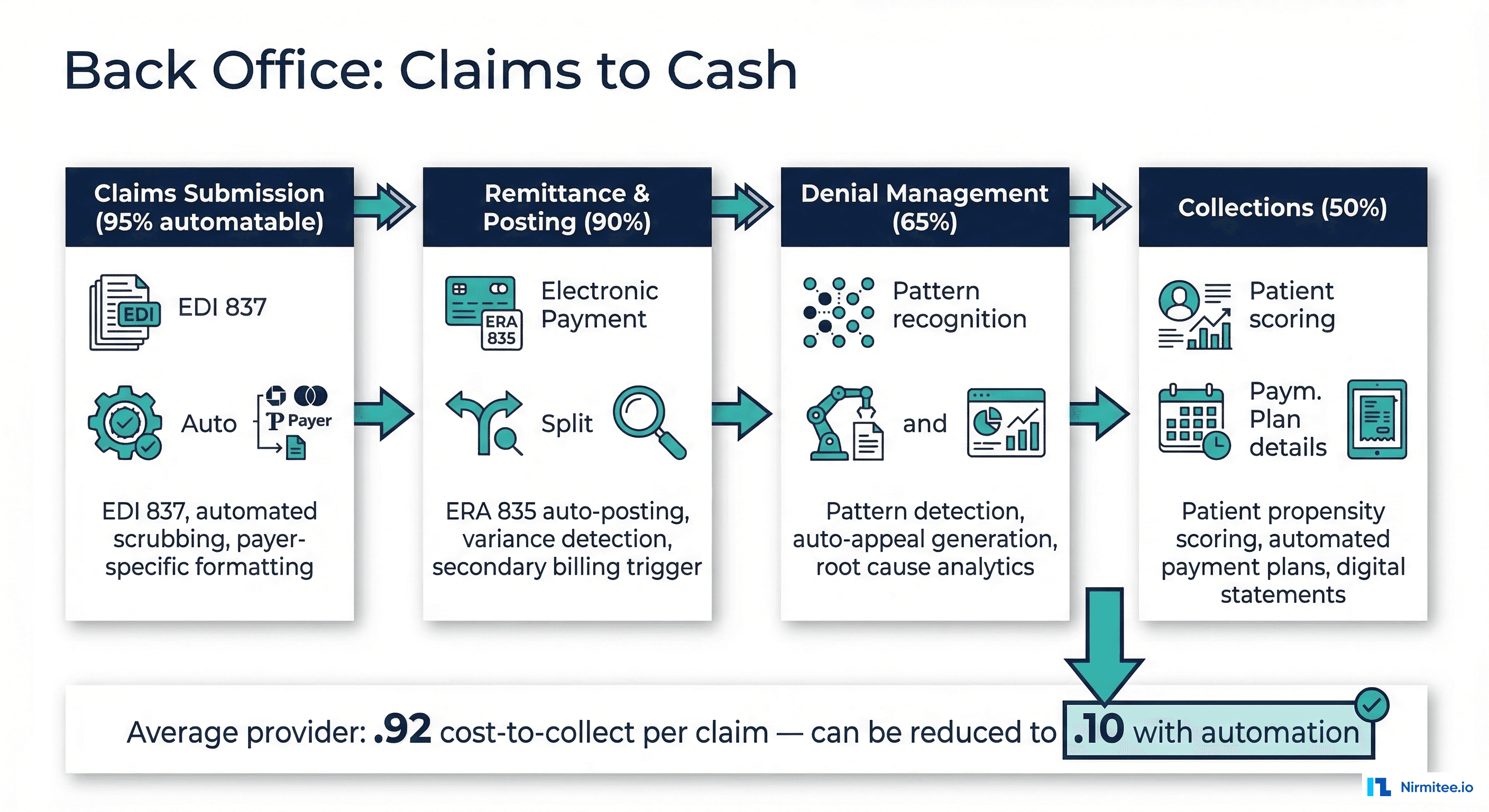
Claims Submission (95% Automatable)
Electronic claims submission via EDI 837 is already near-fully automated at most health systems. The remaining 5% are paper claims (still required by some Workers' Comp and auto liability payers) and complex claims requiring manual attachment assembly. The real automation opportunity in claims submission isn't the submission itself — it's pre-submission intelligence: routing claims to the optimal clearinghouse based on payer acceptance rates, timing submission to avoid known payer processing delays, and batching related claims for coordination of benefits efficiency.
Remittance and Payment Posting (90% Automatable)
Electronic Remittance Advice (ERA, EDI 835) parsing and auto-posting is well-established technology. Payments are matched to claims, adjustments are categorized by reason code, and balances are updated automatically. The remaining 10%: manual remittances from small payers, complex adjustment scenarios requiring human interpretation, and coordination of benefits postings where primary and secondary payer logic creates ambiguity. Automation enhancement: variance detection algorithms that flag postings where the payment differs from expected reimbursement by more than a threshold, triggering investigation before the claim ages.
Denial Management (65% Automatable)
Denial management is the highest-value back office automation target. The average health system has a 5-10% initial denial rate, and each denied claim costs $25-118 to rework (HFMA data). AI-powered denial management systems can: (1) classify denials by root cause automatically from CARC/RARC codes, (2) route denials to the appropriate resolution workflow (rebill, clinical appeal, technical correction), (3) generate appeal letters using templates populated with claim-specific clinical data, and (4) predict appeal success probability to prioritize high-value opportunities. The remaining 35%: complex clinical appeals requiring physician narratives, peer-to-peer reviews with payer medical directors, and denials involving regulatory disputes that require legal review.
Patient Collections (50% Automatable)
Patient financial responsibility continues to grow as high-deductible plans proliferate. Automation opportunities include: propensity-to-pay scoring (predicting which patients are likely to pay and how much), automated payment plan enrollment based on balance and income data, digital statement delivery with embedded payment links, and chatbot-assisted billing inquiries. The reason this function is only 50% automatable: collections is inherently a human-relationship activity. Patients in financial distress need empathetic conversations. Patients confused by their bills need explanations that account for their specific situation. No-surprise billing regulations (the No Surprises Act) add complexity that requires case-by-case evaluation.
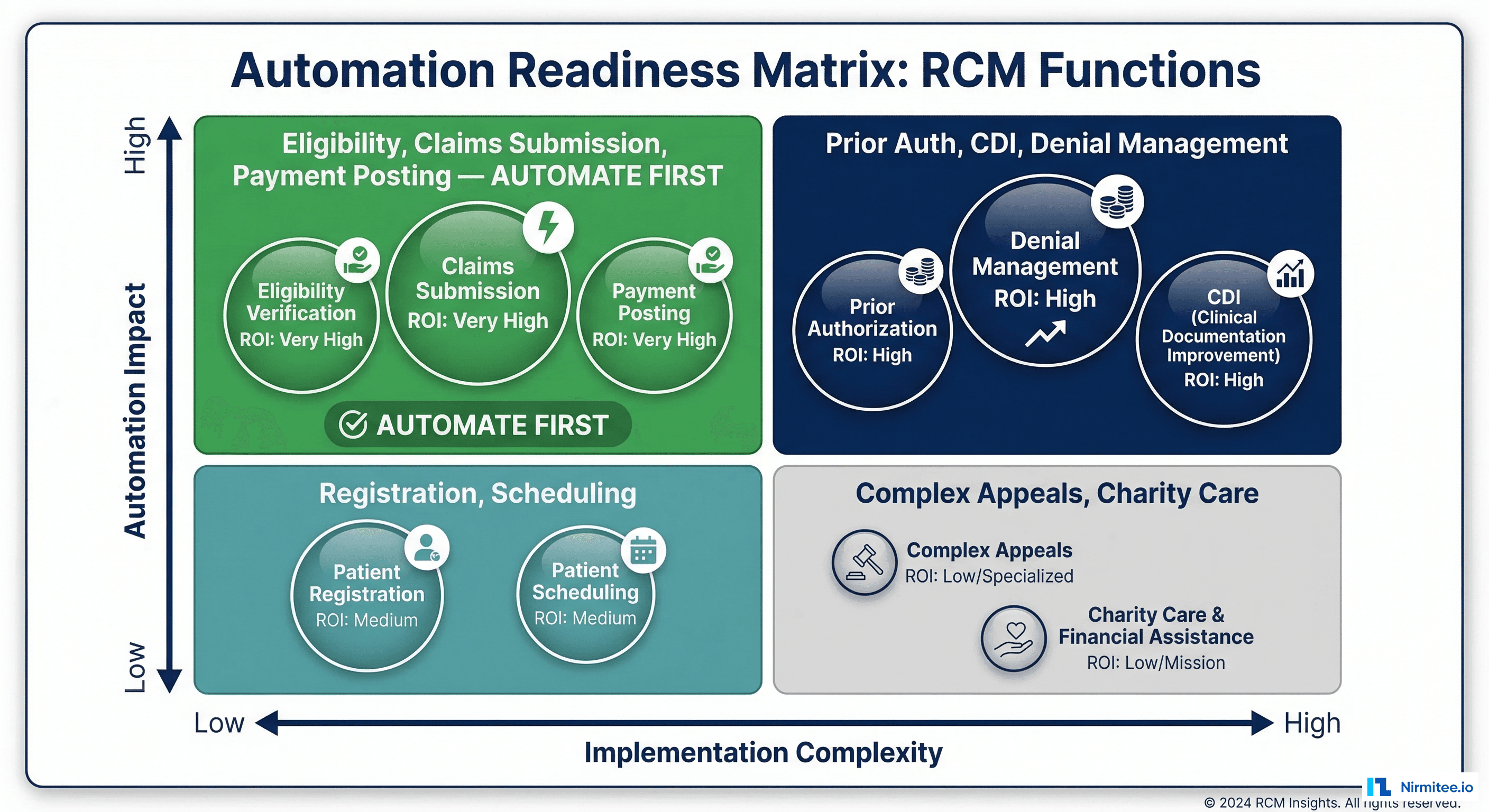
The Automation Readiness Matrix
Not all functions should be automated in the same sequence. Use this prioritization matrix to identify where to invest first based on automation impact and implementation complexity:
| Function | Automation % | Complexity | Annual Savings Potential (500-bed) | Priority |
|---|---|---|---|---|
| Eligibility Verification | 90% | Low | $1.2M-1.8M | Immediate |
| Claims Submission | 95% | Low | $800K-1.2M | Immediate |
| Payment Posting | 90% | Low | $600K-900K | Immediate |
| Charge Capture | 85% | Medium | $1.5M-2.5M | 90 days |
| Prior Authorization | 75% | High | $2M-4M | 90 days |
| Medical Coding | 70% | High | $3M-5M | 6 months |
| Denial Management | 65% | High | $2M-3.5M | 6 months |
| CDI | 65% | High | $2.5M-4M | 6 months |
| Patient Collections | 50% | Medium | $1M-2M | 12 months |
What's Automatable Now vs. the 2-3 Year Horizon
The distinction between "automatable now" and "needs maturation" is critical for investment planning. Automating functions prematurely leads to quality issues and clinical risk. Waiting too long means competitors capture the operational advantage first.
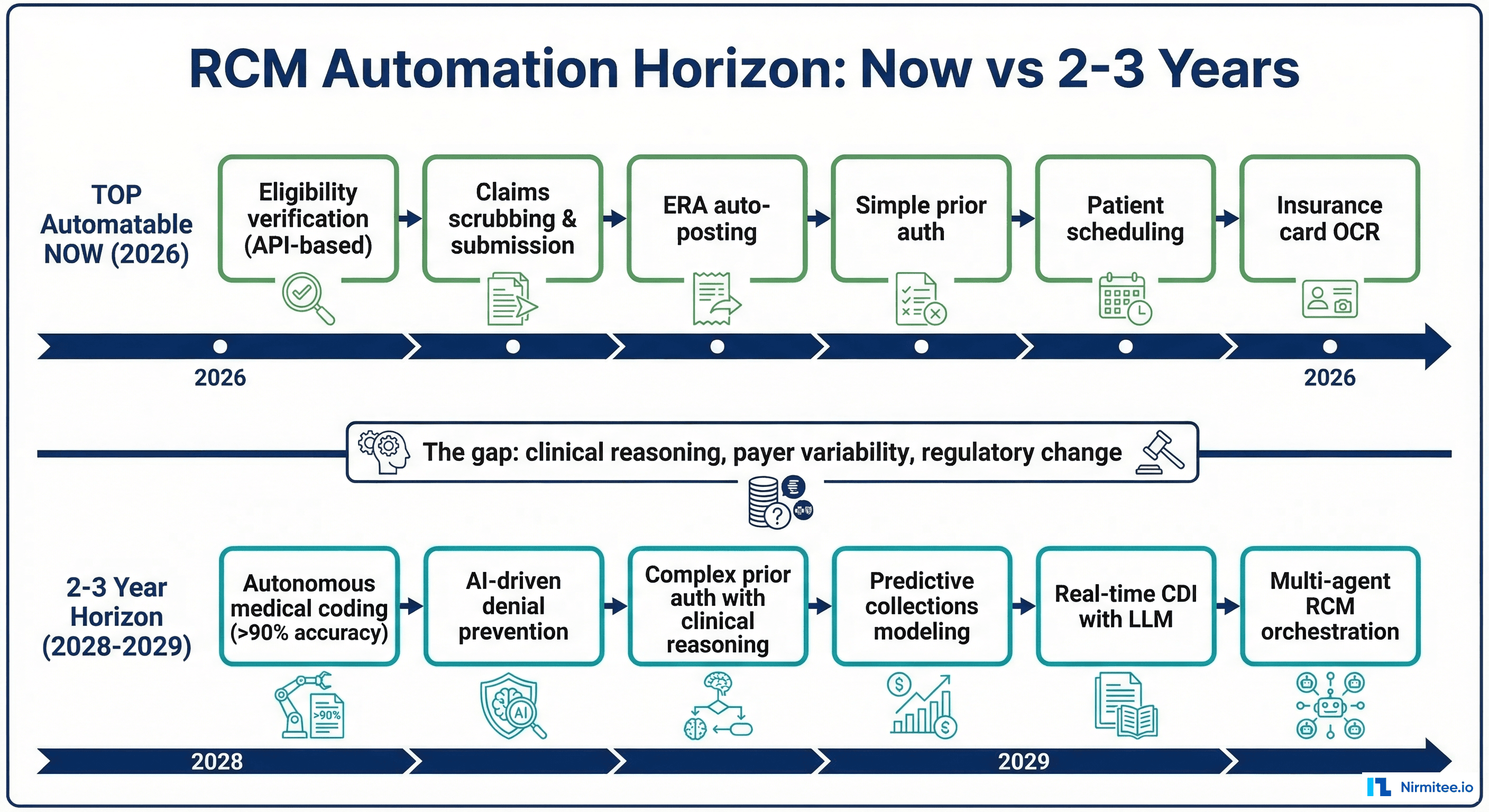
Automatable Now (2026)
- Eligibility verification via real-time payer APIs (270/271, FHIR Coverage)
- Claims scrubbing and submission with rules-based edits and EDI automation
- ERA auto-posting with variance detection and exception routing
- Simple prior authorization for standardized procedures via payer portals and APIs
- Patient scheduling with self-service booking and no-show prediction
- Insurance card OCR and demographic validation for registration
- Charge capture from structured order data with missing charge detection
2-3 Year Horizon (2028-2029)
- Autonomous medical coding achieving 90%+ accuracy across outpatient encounters using clinical LLMs
- AI-driven denial prevention that predicts and corrects likely-to-deny claims before submission
- Complex prior authorization with clinical reasoning agents that assemble supporting documentation
- Predictive collections modeling that optimizes outreach timing, channel, and messaging per patient
- Real-time CDI with LLMs that generate physician queries during the encounter, not days later
- Multi-agent RCM orchestration where specialized AI agents coordinate across the revenue cycle
The gap between "now" and "2-3 years" is primarily about: (1) clinical reasoning capability of AI models, (2) payer API standardization (particularly for prior auth and benefits), and (3) regulatory clarity around AI-assisted coding and clinical decision-making.
The Agent Network Vision
The most ambitious vision for revenue cycle automation isn't automating individual functions — it's creating a network of specialized AI agents that orchestrate the entire revenue cycle end-to-end.
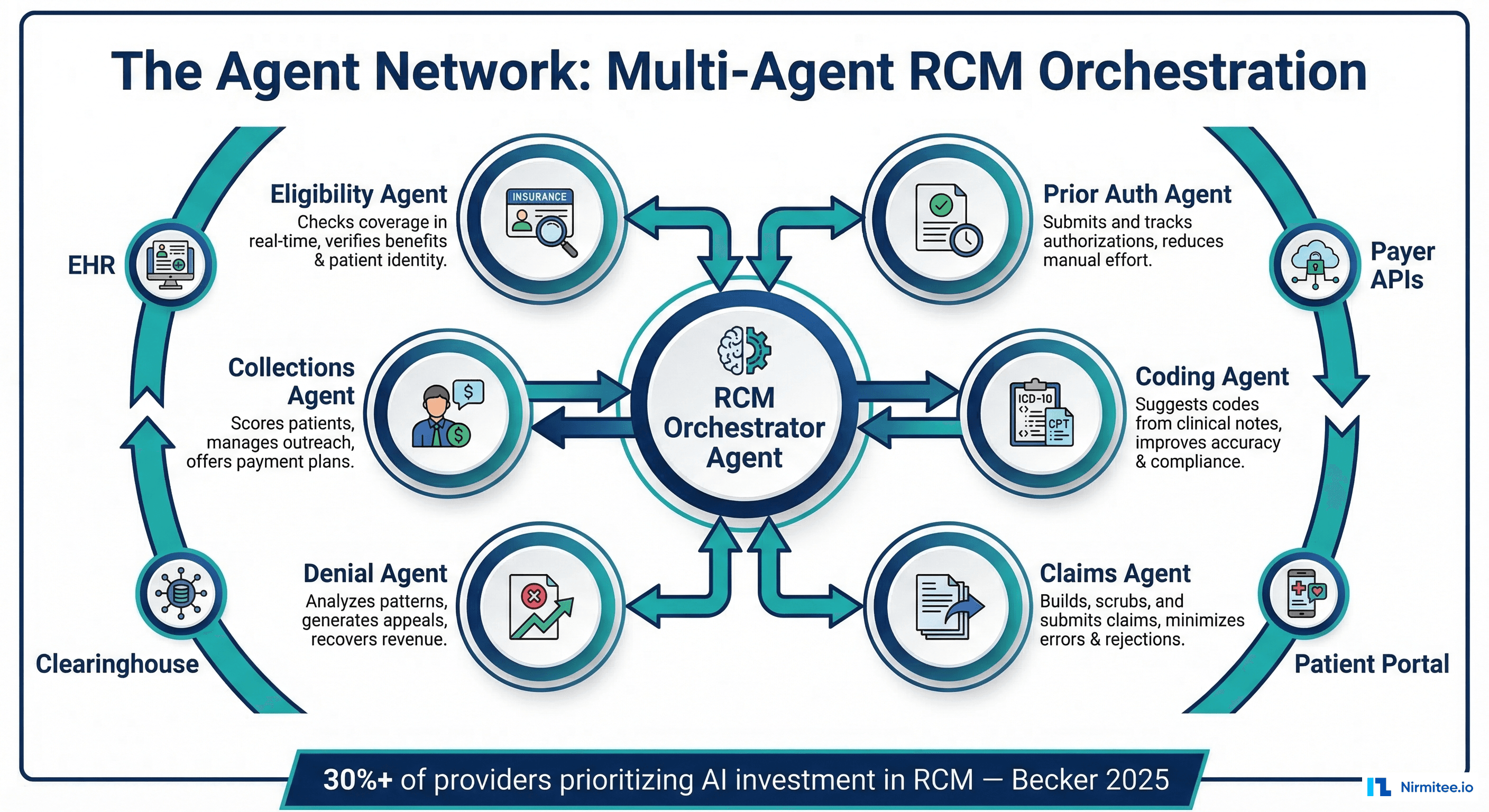
In this model, each revenue cycle function is handled by a specialized agent:
- Eligibility Agent: Monitors patient coverage in real-time, alerts scheduling when coverage changes, and pre-verifies benefits before every encounter
- Prior Auth Agent: Submits authorization requests, tracks status, escalates delays, and assembles clinical documentation for complex cases
- Coding Agent: Reviews clinical documentation, suggests codes, and learns from denial patterns to improve accuracy
- Claims Agent: Builds claims from coded encounters, runs pre-submission edits, routes to the optimal clearinghouse, and monitors submission status
- Denial Agent: Analyzes denial patterns, identifies root causes, generates appeals, and tracks appeal outcomes for continuous improvement
- Collections Agent: Scores patient propensity to pay, generates payment plans, manages outreach cadences, handles billing inquiries
An orchestrator agent coordinates between these specialists, managing handoffs, resolving conflicts (e.g., when the coding agent and denial agent disagree on code selection), and escalating to human operators when confidence is low.
This isn't science fiction — early versions of multi-agent RCM systems are in pilot at several large health systems. The technology stack exists: agentic AI frameworks, FHIR APIs for EHR data access, payer APIs for eligibility and claims, and LLMs for clinical reasoning. The gap is integration, validation, and regulatory acceptance.
Measuring Touchless Rate: The Key Metric
The defining metric for revenue cycle automation is the touchless rate — the percentage of claims that go from charge to cash without any human intervention. Industry benchmarks:
- Current average: 30-40% touchless rate (most health systems)
- Best-in-class today: 60-70% touchless rate (health systems with mature automation)
- McKinsey target: 80-85% touchless rate (achievable with current technology for straightforward encounters)
- Theoretical maximum: 90-92% (some claims will always require human review due to complexity, edge cases, and regulatory requirements)
Track touchless rate by encounter type, payer, and department. You'll find that straightforward office visits with commercial insurance may already be 70-80% touchless, while complex inpatient stays with Medicare Advantage are 20-30%. Target your automation investment at the encounter types with the largest gap between current and achievable touchless rates.
Frequently Asked Questions
What's the realistic ROI timeline for RCM automation?
Front office automation (eligibility, scheduling, registration) typically shows ROI within 6 months. Middle office automation (coding, CDI) takes 12-18 months due to model training and validation requirements. Back office automation (denial management, collections) shows ROI in 9-12 months. Total program ROI for a 500-bed health system investing $3-5M in comprehensive RCM automation: 18-24 months to breakeven, with $8-15M annual savings at steady state.
Does automation mean eliminating RCM staff?
Not in the short term. Automation shifts staff from repetitive tasks (manual eligibility calls, simple coding, claims resubmission) to exception handling, complex case management, and quality oversight. The most successful health systems use automation to handle volume growth without proportional staff increases — not to reduce headcount. McKinsey estimates that automation allows 25-35% productivity improvement per FTE, meaning you need fewer new hires as volume grows rather than laying off existing staff.
How do we avoid vendor lock-in with RCM automation platforms?
Build on standards. Use FHIR APIs for EHR data access, EDI standards for payer communication, and open model APIs for AI components. Avoid monolithic RCM automation platforms that bundle everything — they create the same vendor dependency that legacy EHR systems created. Instead, use a composable architecture: best-of-breed tools for each function (eligibility, coding, denial management) integrated through a common data platform and integration layer.
What role does the CMS prior auth mandate play in this?
The CMS mandate (effective January 2027) is a forcing function for front office automation. It requires CMS-regulated payers to support FHIR-based prior authorization APIs, enabling electronic submission and status tracking. This makes prior auth automation feasible at scale for the first time. Health systems that build prior auth automation now will be ready when payer APIs go live — and will capture the savings immediately while competitors are still implementing.
Conclusion
The touchless revenue cycle isn't a distant aspiration — parts of it are achievable today. Eligibility verification, claims submission, and payment posting are ready for near-complete automation. Medical coding and denial management are on a 2-3 year trajectory toward high-confidence automation. The multi-agent orchestration vision represents the 5-year horizon where specialized AI agents coordinate the entire revenue cycle with minimal human intervention.
The health systems that move first will capture compounding advantages: lower cost-to-collect, faster cash cycles, fewer denials, and the ability to scale revenue operations without proportional staff growth. The McKinsey framework provides the roadmap. The technology is mature enough to start. The only question is organizational will.
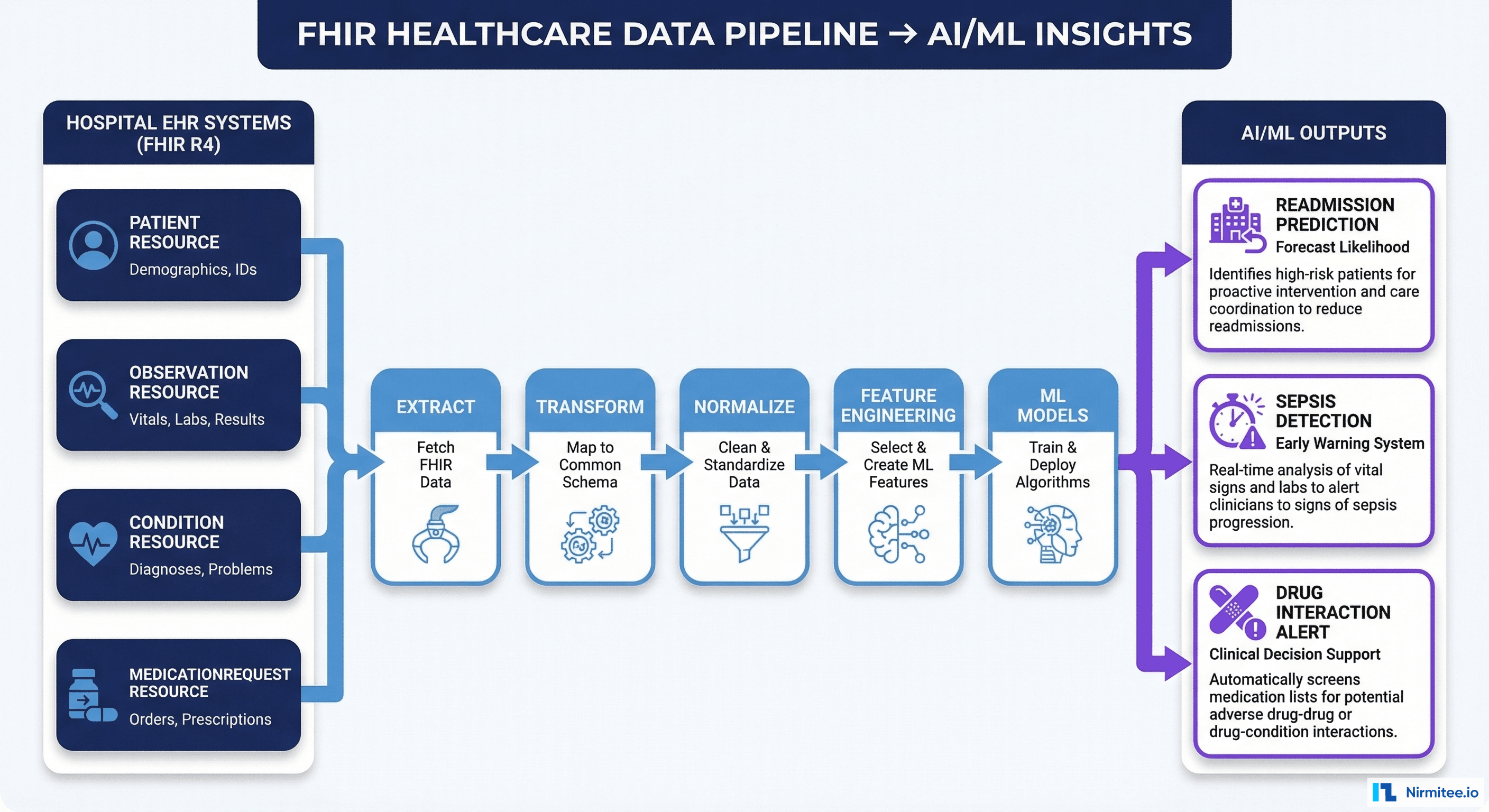
Ready to assess your revenue cycle automation readiness? At Nirmitee, we help health systems build the technology infrastructure for touchless revenue cycles — from FHIR API integrations to AI agent orchestration. We can map your current touchless rate by function and deliver a prioritized automation roadmap in 3 weeks. Start the conversation.