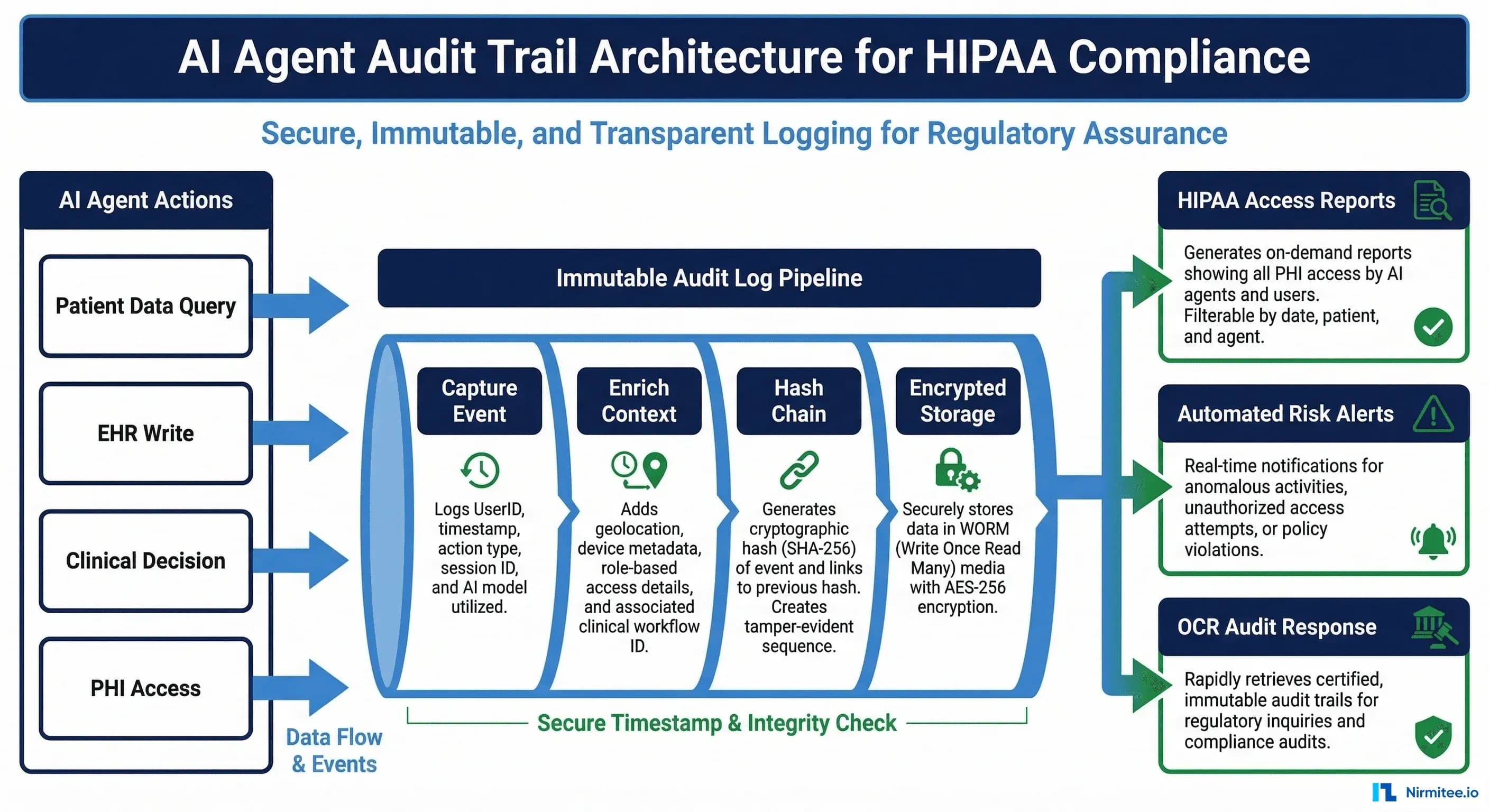
When healthcare organizations deploy AI agents that access patient data, a critical question emerges: how do you prove to auditors, regulators, and your own compliance team that every action was authorized, justified, and traceable? The answer is a purpose-built audit trail system designed specifically for AI agent operations.
Traditional EHR access logs track human users clicking through screens. AI agents operate differently — they make hundreds of data access decisions per minute, chain multiple FHIR queries together, and generate clinical recommendations that influence care. Your audit infrastructure must keep pace.
Why Standard EHR Audit Logs Fall Short for AI Agents
HIPAA Security Rule §164.312(b) requires audit controls for any system containing or using PHI. Most EHR systems satisfy this with built-in access logs. But when AI agents enter the picture, standard logs miss critical context:
- No decision rationale: An EHR log shows "System accessed Patient/12345." An AI audit trail must show why — "Sepsis risk model queried vitals for real-time scoring, triggered by nurse opening chart."
- No chain of actions: AI agents execute multi-step workflows. A single clinical recommendation might involve 15 FHIR queries. Standard logs show 15 disconnected access events with no relationship.
- No confidence tracking: When an AI agent generates a clinical suggestion, regulators want to know the model version, confidence score, and whether alternatives were considered.
- No tamper evidence: If an AI agent makes a mistake, you need cryptographic proof that the audit log hasn't been modified after the fact.
The AI Agent Audit Event Schema
Every AI agent action should generate a structured audit event. Here's the schema we use in production:
from dataclasses import dataclass, field
from datetime import datetime
from enum import Enum
import hashlib, json, uuid
class ActionType(Enum):
READ = "READ"
WRITE = "WRITE"
DECISION = "DECISION"
ESCALATION = "ESCALATION"
class Outcome(Enum):
SUCCESS = "SUCCESS"
DENIED = "DENIED"
ESCALATED = "ESCALATED"
@dataclass
class AuditEvent:
event_id: str = field(default_factory=lambda: str(uuid.uuid4()))
timestamp: str = field(default_factory=lambda: datetime.utcnow().isoformat() + "Z")
agent_id: str = ""
agent_version: str = ""
action_type: ActionType = ActionType.READ
fhir_resource_type: str = "" # Patient, Observation, MedicationRequest
fhir_resource_id: str = ""
patient_id_token: str = "" # Tokenized, not raw MRN
justification: str = "" # Clinical context for the access
outcome: Outcome = Outcome.SUCCESS
model_version: str = "" # For DECISION events
confidence_score: float = 0.0 # For DECISION events
correlation_id: str = "" # Links related events in a workflow
previous_hash: str = "" # Hash chain link
event_hash: str = ""
def compute_hash(self):
payload = json.dumps({
"event_id": self.event_id,
"timestamp": self.timestamp,
"agent_id": self.agent_id,
"action_type": self.action_type.value,
"resource": self.fhir_resource_type,
"patient_token": self.patient_id_token,
"outcome": self.outcome.value,
"previous_hash": self.previous_hash
}, sort_keys=True)
self.event_hash = hashlib.sha256(payload.encode()).hexdigest()
return self.event_hashBuilding the Immutable Hash Chain
The hash chain is what makes your audit trail tamper-evident. Each event includes the hash of the previous event, creating a cryptographic chain that breaks if any record is modified:
class AuditChain:
def __init__(self):
self.last_hash = "GENESIS"
def append(self, event: AuditEvent) -> AuditEvent:
event.previous_hash = self.last_hash
event.compute_hash()
self.last_hash = event.event_hash
# Write to immutable storage (S3 Object Lock, Azure Immutable Blob)
self._persist(event)
return event
def verify_chain(self, events: list) -> bool:
"""Verify the entire chain is intact."""
expected_prev = "GENESIS"
for event in events:
if event.previous_hash != expected_prev:
return False # Chain broken - tampering detected
event_copy = AuditEvent(**vars(event))
event_copy.event_hash = ""
computed = event_copy.compute_hash()
if computed != event.event_hash:
return False # Event modified
expected_prev = event.event_hash
return TrueWhat to Log: The HIPAA Minimum + AI Extras
HIPAA §164.312(b) requires audit controls but doesn't prescribe exact fields. For AI agents, we recommend two tiers:
Tier 1: HIPAA Required (Every Action)
- Who: Agent ID + version + the human user who initiated the workflow
- What: FHIR resource type, resource ID, action type (READ/WRITE/DECISION)
- When: ISO 8601 timestamp with timezone
- Where: System identifier, network origin, deployment environment
- Outcome: Success, denied, or escalated to human review
Tier 2: AI-Specific (Clinical Decisions)
- Model version: Exact model ID that generated the recommendation
- Confidence score: The model's confidence in its output
- Alternatives considered: For drug recommendations, what alternatives were evaluated
- Evidence chain: Which data inputs drove the decision (lab values, vitals, history)
- Human review status: Was this reviewed by a clinician? Accepted/modified/rejected?
- Correlation ID: Links all events in a multi-step agent workflow
Automated Compliance Reporting
The real value of structured audit data is automated compliance. Instead of spending weeks preparing for an OCR audit, your system generates reports on demand:
def generate_hipaa_access_report(patient_id_token: str, date_range: tuple) -> dict:
"""Generate HIPAA-compliant access report for a specific patient."""
events = query_audit_store(
patient_token=patient_id_token,
start_date=date_range[0],
end_date=date_range[1]
)
return {
"patient_token": patient_id_token,
"period": {"start": date_range[0], "end": date_range[1]},
"total_access_events": len(events),
"by_action_type": group_by(events, "action_type"),
"by_agent": group_by(events, "agent_id"),
"denied_events": [e for e in events if e.outcome == Outcome.DENIED],
"escalated_events": [e for e in events if e.outcome == Outcome.ESCALATED],
"chain_integrity": verify_chain(events),
"anomalies": detect_anomalies(events), # Unusual access patterns
}Real-Time Anomaly Detection
With structured audit events flowing in real-time, you can detect suspicious patterns before they become breaches:
- Volume anomalies: An agent accessing 10x more patient records than its baseline — possible misconfiguration or data exfiltration
- Scope violations: An agent designed for cardiology is accessing oncology records outside its authorized scope
- Time anomalies: Agent activity during maintenance windows or outside expected operational hours
- Escalation rate spikes: Sudden increase in denied or escalated actions may indicate model drift or adversarial inputs
Infrastructure: Where to Store AI Audit Logs
Audit logs for AI agents must be stored separately from the AI system itself — an agent should never be able to modify its own audit trail. Recommended approaches:
- AWS: S3 with Object Lock (WORM compliance) + Athena for querying + CloudTrail for meta-audit
- Azure: Immutable Blob Storage + Azure Data Explorer for analytics + Azure Monitor
- GCP: Cloud Storage with retention policies + BigQuery for analysis + Cloud Audit Logs
All options must be configured with: encryption at rest (AES-256), retention policies aligned with your state's medical record retention requirements (typically 7-10 years), and access controls that prevent the AI system from modifying or deleting logs.
Breach Response: How Audit Trails Save You
When (not if) a breach investigation occurs, comprehensive audit trails directly support HIPAA Breach Notification Rule (§164.404) compliance. Within 60 days, you must identify every affected individual. With proper audit data, this query takes minutes instead of weeks:
# Breach scope assessment - which patients were affected?
SELECT DISTINCT patient_id_token,
MIN(timestamp) as first_access,
MAX(timestamp) as last_access,
COUNT(*) as total_events,
COUNT(CASE WHEN action_type = 'WRITE' THEN 1 END) as write_events
FROM ai_audit_events
WHERE agent_id = 'compromised-agent-id'
AND timestamp BETWEEN '2026-03-01' AND '2026-03-21'
GROUP BY patient_id_token
ORDER BY total_events DESC;Getting Started
If you're deploying AI agents in healthcare, audit infrastructure should be built before the first patient data access, not retrofitted later. Start with the event schema, add the hash chain for integrity, connect to immutable storage, and build compliance reporting on top.
For a broader view of HIPAA-compliant AI agent architecture, see our complete architecture guide. For the autonomy patterns that govern when agents can act independently vs. requiring human review, read about bounded autonomy architecture.
At Nirmitee, we build production audit infrastructure for healthcare AI systems. If you're planning an AI agent deployment and need help getting the compliance architecture right, let's talk.
Related reading
For more insights, explore our guides on AI agents in healthcare and FHIR in Modern Healthcare.
You may also find value in EHR Software Development Guide and Building a Healthtech App.


