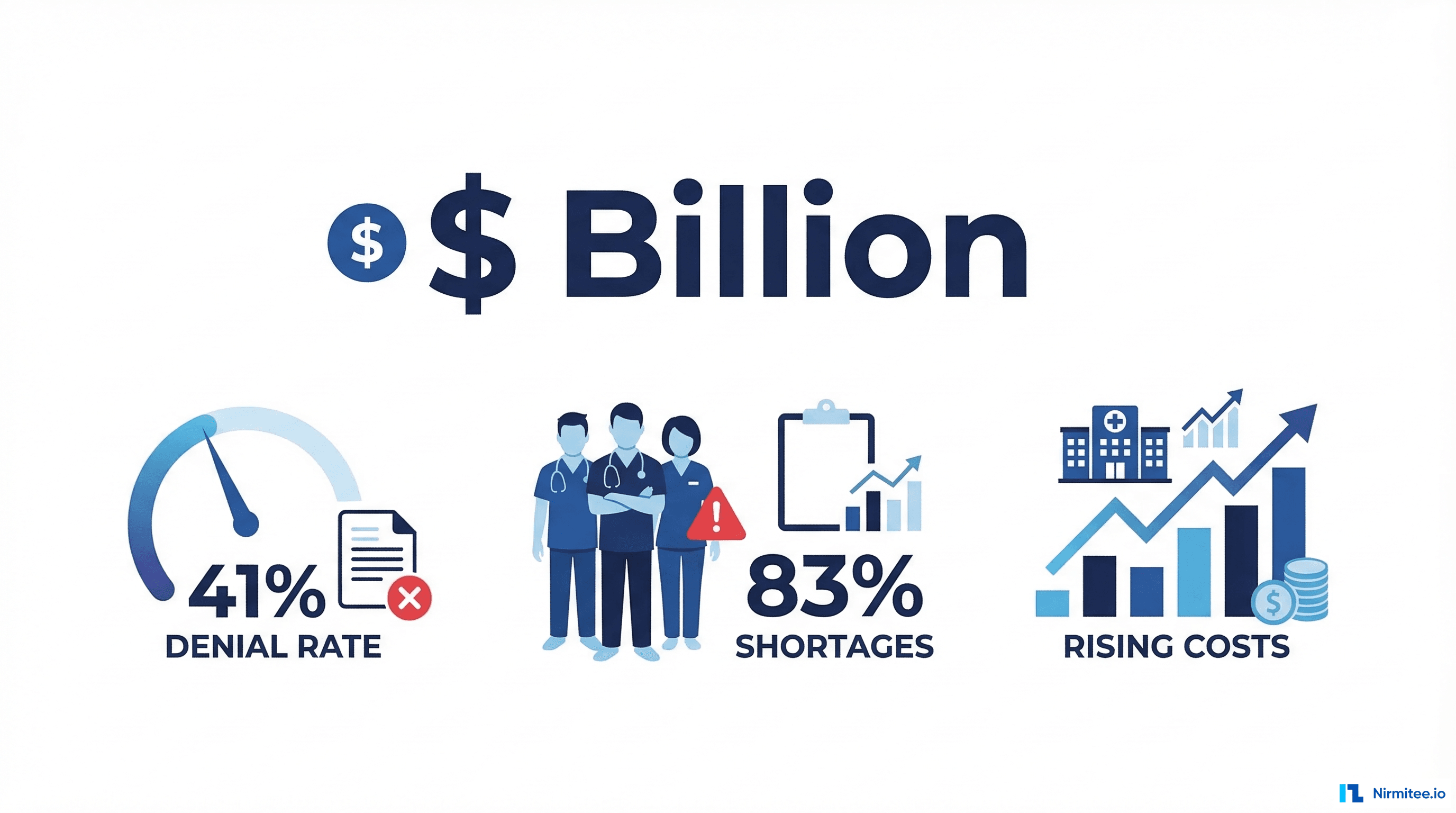
The American healthcare revenue cycle is broken. Not bending, not strained — structurally broken. The United States loses $262 billion annually to revenue cycle inefficiency, a figure that has grown every year for the past decade. Claim denial rates have surged from 30% in 2022 to 41% in 2025, according to Experian Health's State of Claims report. And 83% of healthcare leaders now report labor shortages across their revenue cycle operations, per the HFMA 2025 workforce survey.
These are not abstract numbers. They represent hospitals closing departments, physician groups leaving communities, and health systems operating on margins so thin that a single bad quarter triggers layoffs. The revenue cycle — the sequence of administrative processes from patient scheduling through final payment — has become the single largest operational liability in American healthcare.
But something is shifting. A new class of artificial intelligence, known as agentic AI, is moving beyond the chatbots and predictive models that dominated healthcare AI conversations in 2023 and 2024. Agentic AI systems do not wait to be asked. They observe, reason, plan, and execute multi-step workflows autonomously — verifying insurance eligibility, coding clinical encounters, scrubbing claims for errors, appealing denials, and collecting patient balances without human intervention at every step.
This is not incremental automation. This is the beginning of the touchless revenue cycle — a future where the majority of revenue cycle transactions flow from charge capture through payment without a human touching them. And the race to get there is already underway.
In this article, we examine the data behind the crisis, the technology making autonomous RCM possible, the vendors leading the charge, the regulatory landscape shaping deployment, and a practical roadmap for health systems ready to move.

The Revenue Cycle Crisis: By the Numbers
Before diving into solutions, it is worth understanding the depth of the problem. Revenue cycle management has always been complex, but the post-pandemic era has pushed it past a tipping point.
The Denial Rate Explosion
Claim denials are the single most expensive failure mode in healthcare revenue cycle. When a claim is denied, the average cost to rework and resubmit it is $25 to $118 per claim, depending on complexity. Multiply that by millions of denied claims per year, and the math is staggering.
The trend line is alarming. Denial rates have escalated consistently:
- 2022: 30% initial denial rate (MGMA benchmark)
- 2023: 34% (Change Healthcare/Optum data)
- 2024: 38% (Experian Health mid-year report)
- 2025: 41% (Experian Health State of Claims 2025)
The drivers behind this increase are well-documented: payer policy changes, increased use of AI by payers for automated denials, coding complexity from ICD-10 updates, and prior authorization requirements that have expanded dramatically.
The Labor Crisis
Revenue cycle departments cannot hire fast enough. The HFMA 2025 Workforce Survey found that 83% of healthcare leaders report labor shortages across revenue cycle functions. The positions hardest to fill are medical coders (45% vacancy rate at community hospitals), prior authorization specialists, and denial management analysts.
This creates a vicious cycle: fewer staff means more errors, more errors mean more denials, more denials mean more rework, and more rework means staff burnout and further attrition. The average tenure of a revenue cycle specialist has dropped to 18 months, down from 3 years in 2019.
The Financial Pressure
Hospital operating margins averaged -1.3% in 2024, according to Kaufman Hall's National Hospital Flash Report. Rural and community hospitals are disproportionately affected, with over 600 facilities at risk of closure. Revenue cycle inefficiency is not the only cause, but it is the one most amenable to technological intervention.
The bottom line: health systems are spending $12 to $15 per claim on administrative processing, and roughly 30% of that spend is pure waste — rework, manual data entry, phone calls to payers, and chasing denials that should never have occurred.
What Agentic AI Actually Means for RCM
The term "AI" in healthcare has been diluted by years of vendor marketing. Rule-based engines were called AI. Simple chatbots were called AI. Predictive models that scored claims for denial risk were called AI. Each of these has value, but none of them are what the industry now means by agentic AI.
Agentic AI refers to systems that exhibit four capabilities simultaneously:
- Perception: The agent reads and understands unstructured clinical documentation, payer policy documents, EOBs, remittance advice, and patient communications.
- Reasoning: The agent applies clinical and financial logic to determine the correct course of action — not just pattern matching, but multi-step causal reasoning about why a claim was denied and what evidence would overturn it.
- Planning: The agent constructs a sequence of actions — querying an eligibility API, pulling a clinical note, mapping to ICD-10 codes, generating an appeal letter, submitting it through the correct payer portal — without being explicitly programmed for every scenario.
- Action: The agent executes those steps, interacting with real systems through APIs, RPA, or direct integration, and monitors the outcome to decide what to do next.
This is fundamentally different from a predictive model that flags high-risk claims for human review. An agentic system resolves the claim. It does not create a worklist — it works the worklist.
The distinction matters enormously for ROI calculation. A predictive denial model might reduce denial write-offs by 15-20%. An agentic system that autonomously resolves denials can reduce them by 40-60%, because it eliminates the bottleneck: human bandwidth.
As we explored in our analysis of how agentic AI is streamlining data management in healthcare, the shift from passive to active AI is the defining transition of this decade in health IT.
McKinsey's 4 Levels of RCM Automation
McKinsey & Company's healthcare practice has proposed a useful framework for understanding where organizations sit on the automation maturity curve. Their four levels of RCM automation provide a roadmap from today's assisted tools to tomorrow's touchless revenue cycle.
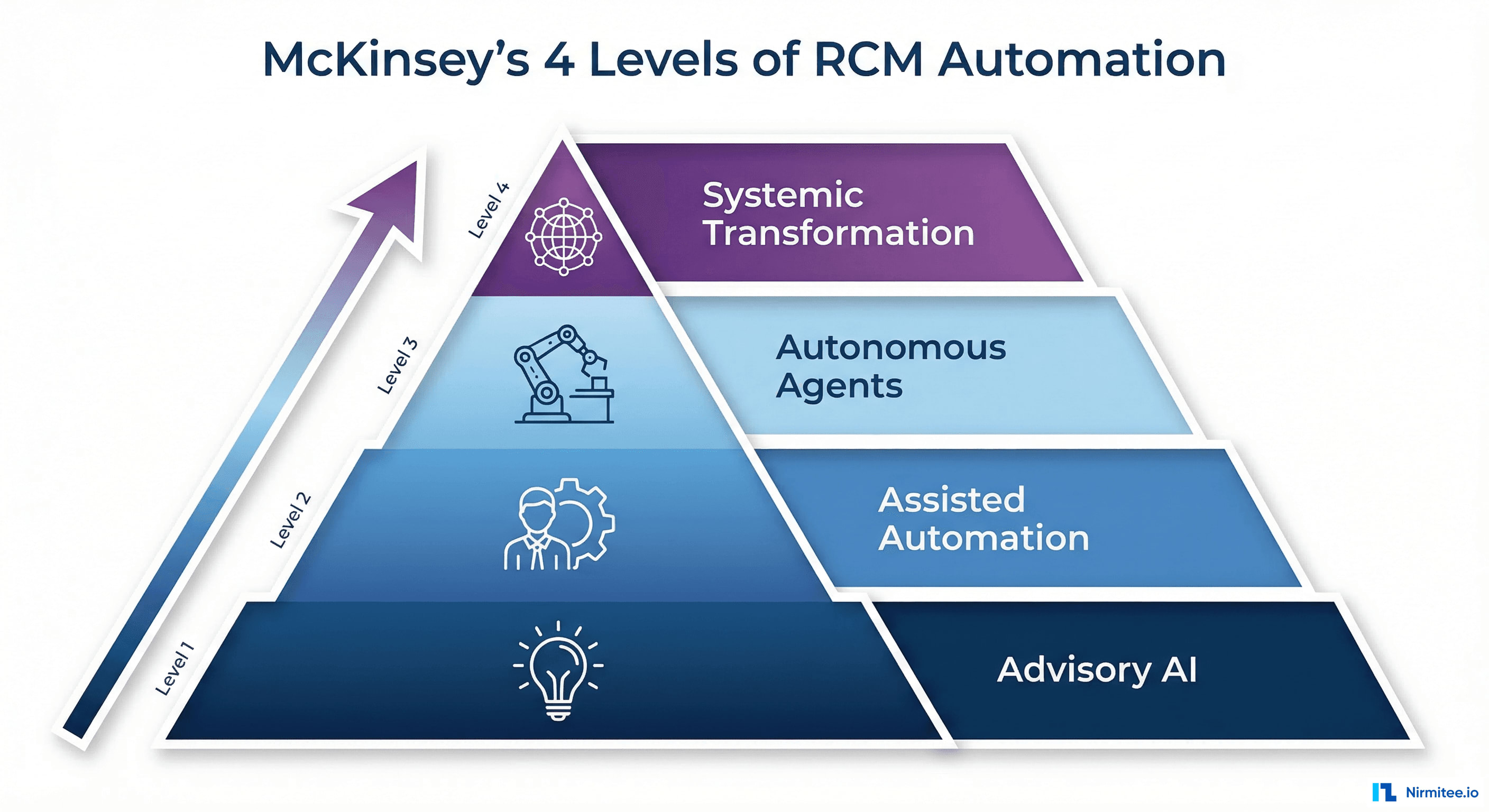
Level 1: Advisory AI
At this level, AI systems provide recommendations to human operators. Think of a denial prediction model that highlights claims likely to be denied before submission, or a coding assistant that suggests ICD-10 codes for a coder to review and accept. The human remains the decision-maker and executor.
Where most health systems are today: Level 1 represents the current state for approximately 60% of US hospitals with some form of RCM technology. Common tools include denial prediction dashboards, charge capture validation alerts, and eligibility verification queue prioritization.
Typical ROI: 5-15% reduction in denial rates, 10-20% improvement in coder productivity.
Level 2: Assisted Automation
Here, AI handles routine tasks end-to-end but escalates edge cases to humans. A Level 2 system might automatically verify eligibility for 80% of patients, only flagging the remaining 20% with coverage complexities for manual review. The human-in-the-loop is still essential, but their role shifts from processing to exception handling.
Where early adopters are: Roughly 25% of large health systems have implemented Level 2 automation for at least one RCM function, typically eligibility verification or charge capture. The technology has proven reliable for high-volume, rules-based tasks.
Typical ROI: 20-35% reduction in labor costs for automated functions, 25-40% faster processing times.
Level 3: Autonomous Agents (Agentic AI)
This is where agentic AI enters the picture. Level 3 systems independently handle complex, multi-step workflows including exception cases. A denial management agent, for example, reads the denial reason, retrieves the relevant clinical documentation, identifies the coding or authorization gap, generates an appeal with supporting evidence, and submits it — all without human intervention.
The critical differentiator at Level 3 is adaptive reasoning. The agent does not follow a fixed decision tree. It evaluates the specific circumstances of each case and constructs a response accordingly. When it encounters a scenario it cannot resolve with high confidence, it escalates — but the escalation threshold is much higher than Level 2.
Where the leaders are moving: Fewer than 10% of health systems have deployed Level 3 automation for any RCM function. However, this is the fastest-growing segment, with AI prior authorization spending alone growing 10x from $10 million in 2024 to $100 million in 2025, according to Rock Health's digital health funding analysis.
Typical ROI: 40-60% reduction in denial write-offs, 50-70% reduction in manual touches per claim, 3-6 month payback period.
Level 4: Systemic Transformation
The ultimate vision: a touchless revenue cycle where AI agents manage the entire financial workflow from patient access through final payment. At Level 4, individual agents are orchestrated into a connected system where the eligibility agent's output feeds the coding agent, which feeds the claims agent, which feeds the denial agent, which feeds the collections agent — all operating as a unified autonomous system.
No health system has achieved Level 4 today. But the building blocks are being assembled. The organizations that reach Level 3 across multiple functions will be positioned to orchestrate those agents into Level 4 within 24-36 months.
6 Use Cases Where Agentic AI Is Working Today
The theory is compelling. But CFOs and RCM directors need to see where agentic AI is delivering measurable results right now. Here are six use cases where autonomous agents are operational in US health systems today.
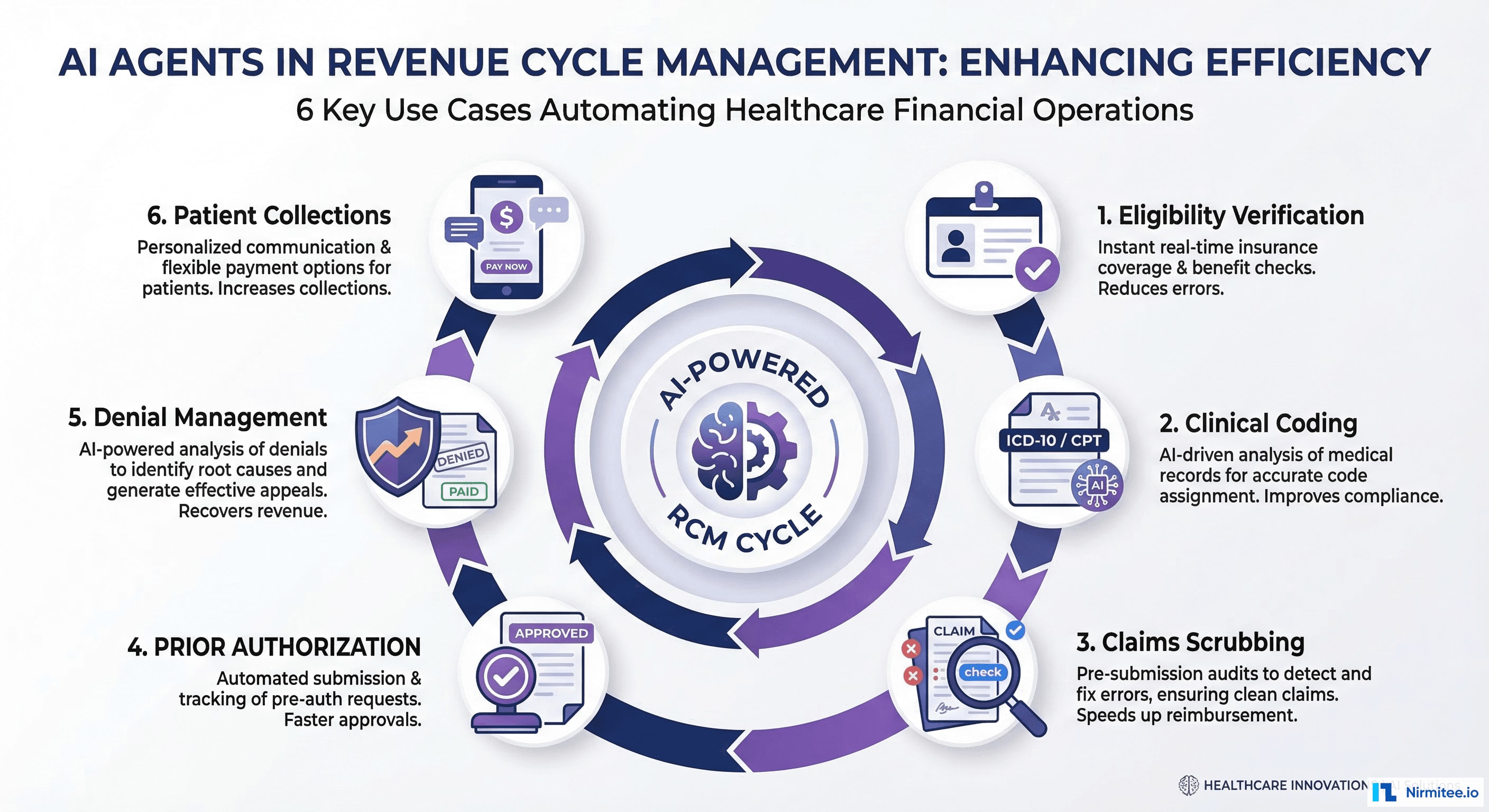
1. Eligibility Verification Agent
The eligibility verification agent operates before the patient arrives. It monitors the schedule, queries payer eligibility APIs (270/271 transactions), interprets coverage details, identifies potential issues (expired coverage, benefit maximums, out-of-network status), and proactively resolves them or alerts the appropriate staff.
How it works architecturally:
- Trigger: New appointment scheduled in EHR or practice management system
- Step 1: Agent queries the patient's insurance through the X12 270/271 real-time eligibility API
- Step 2: Agent parses the 271 response, extracting copay, deductible, coinsurance, and benefit details
- Step 3: Agent cross-references with the scheduled procedure to calculate estimated patient responsibility
- Step 4: If coverage gaps detected, agent initiates secondary insurance verification or flags for patient communication
- Step 5: Agent populates the registration system with verified coverage details
Results in production: Health systems report 95-98% auto-verification rates (up from 60-70% with manual processes), a 75% reduction in registration errors, and a 40% decrease in claim denials due to eligibility issues.
2. Clinical Coding Agent
The clinical coding agent reads physician documentation — progress notes, operative reports, discharge summaries — and generates ICD-10, CPT, and HCPCS codes. Unlike simple NLP-based coding suggestions, an agentic coding system understands clinical context, applies coding guidelines (including laterality, severity, and sequencing rules), and handles multi-code scenarios.
How it works architecturally:
- Trigger: Clinical encounter closed in EHR
- Step 1: Agent retrieves the complete clinical note via FHIR DocumentReference API
- Step 2: LLM-based clinical NLU extracts diagnoses, procedures, medications, and relevant clinical indicators
- Step 3: Agent maps extracted entities to ICD-10-CM/PCS and CPT codes, applying official coding guidelines
- Step 4: Agent validates code combinations against CCI edits, LCD/NCD requirements, and modifier logic
- Step 5: Agent assigns DRG (for inpatient) or APC (for outpatient) and calculates expected reimbursement
- Step 6: Codes with confidence scores below threshold are routed to human coders; high-confidence codes are auto-posted
Results in production: Auto-coding rates of 60-75% for outpatient encounters and 35-50% for inpatient, with accuracy rates of 95-97% on auto-coded encounters. Average coding turnaround time reduced from 3-5 days to under 4 hours.
3. Claims Scrubbing Agent
Before a claim is submitted, the claims scrubbing agent performs a comprehensive review that goes beyond rule-based edits. It evaluates the claim against payer-specific requirements, historical denial patterns, and current medical policies to predict and prevent denials before they occur.
How it works architecturally:
- Trigger: Claim generated in billing system
- Step 1: Agent validates all required fields (demographics, provider NPI, taxonomy, place of service, referring provider)
- Step 2: Agent checks code combinations against CCI edits, NCCI, and payer-specific bundling rules
- Step 3: Agent evaluates medical necessity by cross-referencing diagnoses against LCD/NCD policies for the specific payer
- Step 4: Agent reviews historical denial data for this payer/procedure combination and applies learned corrections
- Step 5: If issues detected, agent auto-corrects (e.g., adding modifiers, resequencing codes) or holds the claim with a specific correction recommendation
Results in production: First-pass clean claim rates improved from 82% to 96%, a 50-60% reduction in preventable denials, and an estimated $3-5 saved per claim in avoided rework costs.
4. Prior Authorization Agent
Prior authorization is the single most hated administrative burden in US healthcare. The AMA reports that physicians spend an average of 14 hours per week on prior auth activities. An agentic prior auth system handles the entire workflow: determining if authorization is required, gathering clinical documentation, submitting the request, monitoring status, and appealing denials.
How it works architecturally:
- Trigger: Order placed in EHR for procedure, medication, or referral
- Step 1: Agent queries payer-specific prior auth requirements database to determine if authorization is needed
- Step 2: Agent extracts relevant clinical data from EHR via FHIR APIs — diagnosis history, lab results, imaging, failed conservative treatments
- Step 3: Agent generates the prior auth request with supporting clinical evidence mapped to the payer's medical policy criteria
- Step 4: Agent submits via payer portal API, X12 278, or fax (with automated fax-to-digital for legacy payers)
- Step 5: Agent monitors for response, handles peer-to-peer scheduling if required, and manages appeals for denials
Results in production: Authorization turnaround reduced from 5-7 days to 24-48 hours, 70% reduction in staff time spent on prior auth, and 30% improvement in initial approval rates due to better clinical evidence packaging.
This is one of the highest-impact use cases and directly connects to the broader question of choosing the right agent framework for healthcare — the orchestration complexity of prior auth requires sophisticated multi-step reasoning that simple RPA cannot achieve.
5. Denial Management Agent
When claims are denied, the denial management agent acts as an autonomous appeal specialist. It reads the EOB/ERA (835), identifies the denial reason (CARC/RARC codes), determines the root cause, assembles the appeal package, and submits it through the appropriate channel — all within hours, not days or weeks.
How it works architecturally:
- Trigger: Denied claim received via 835/ERA or payer portal
- Step 1: Agent parses denial reason codes (CARC/RARC) and maps to root cause categories (clinical, administrative, coding, authorization)
- Step 2: Agent retrieves original claim, clinical documentation, and any relevant payer correspondence
- Step 3: For clinical denials: Agent reviews medical policy, identifies gaps in submitted documentation, pulls additional supporting evidence from EHR
- Step 4: Agent generates the appeal letter using LLM, specifically addressing the denial reason with clinical evidence and regulatory citations
- Step 5: Agent submits the appeal through the payer's required channel (portal, mail, fax) with tracking
- Step 6: Agent monitors appeal status and escalates to Level 2 (external review) if initial appeal is denied
Results in production: Appeal submission time reduced from 15-30 days to 24-72 hours, appeal success rates improved from 45% to 68% (due to faster turnaround and more comprehensive evidence), and a 55% reduction in denial write-offs.
6. Patient Collections Agent
With patient financial responsibility now averaging $1,650 per inpatient stay, patient collections have become a critical revenue cycle function. The collections agent manages the entire patient financial engagement — from pre-service estimates through post-service billing and payment plan management.
How it works architecturally:
- Trigger: Patient balance posted or payment plan milestone reached
- Step 1: Agent calculates patient responsibility based on verified benefits, adjustments, and payer payments
- Step 2: Agent evaluates patient's propensity to pay using financial, demographic, and behavioral data to determine optimal communication strategy
- Step 3: Agent generates personalized outreach via the patient's preferred channel (text, email, patient portal, mail)
- Step 4: Agent offers appropriate payment plan options, financial assistance screening, or charity care qualification based on patient profile
- Step 5: Agent processes payments, manages plan modifications, and escalates to collections only after exhausting patient-friendly options
Results in production: 25-35% improvement in patient collection rates, 40% reduction in bad debt write-offs, 60% decrease in patient billing complaints, and significant improvement in patient satisfaction scores.
The Technology Stack Powering Agentic RCM
Understanding the technology stack behind agentic RCM systems is essential for CIOs and technical leaders evaluating build-versus-buy decisions. The modern agentic RCM stack has four distinct layers.
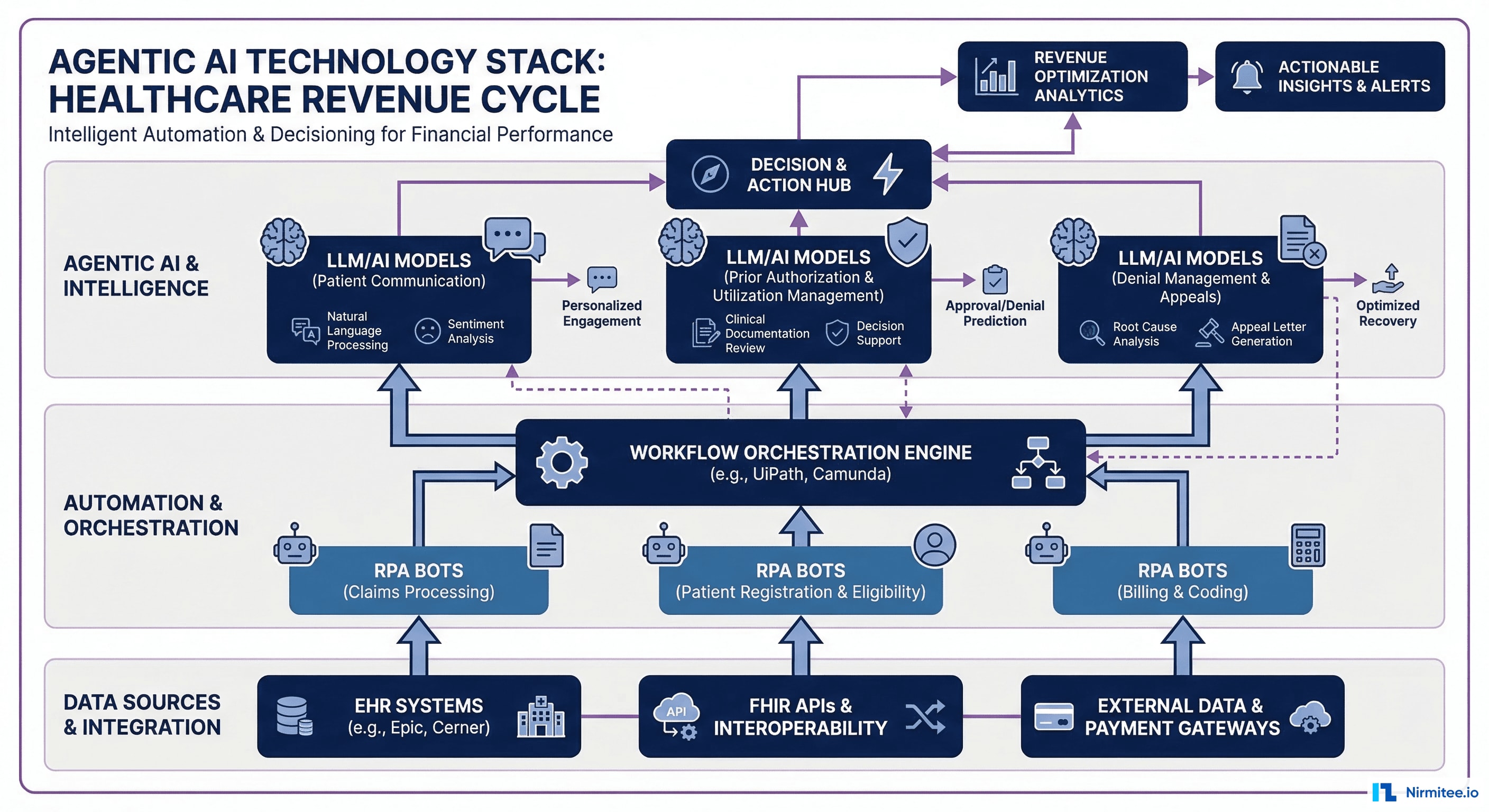
Layer 1: Data Integration and Interoperability
The foundation of any agentic system is access to data. In healthcare RCM, this means:
- HL7 FHIR R4 APIs for clinical data access (Patient, Encounter, Condition, Procedure, DocumentReference resources)
- X12 EDI for payer transactions (270/271 eligibility, 276/277 claim status, 278 prior auth, 835/837 claims)
- Payer portal APIs where available (Availity, Change Healthcare/Optum, individual payer portals)
- RPA connectors for systems without APIs (legacy payer portals, state Medicaid systems)
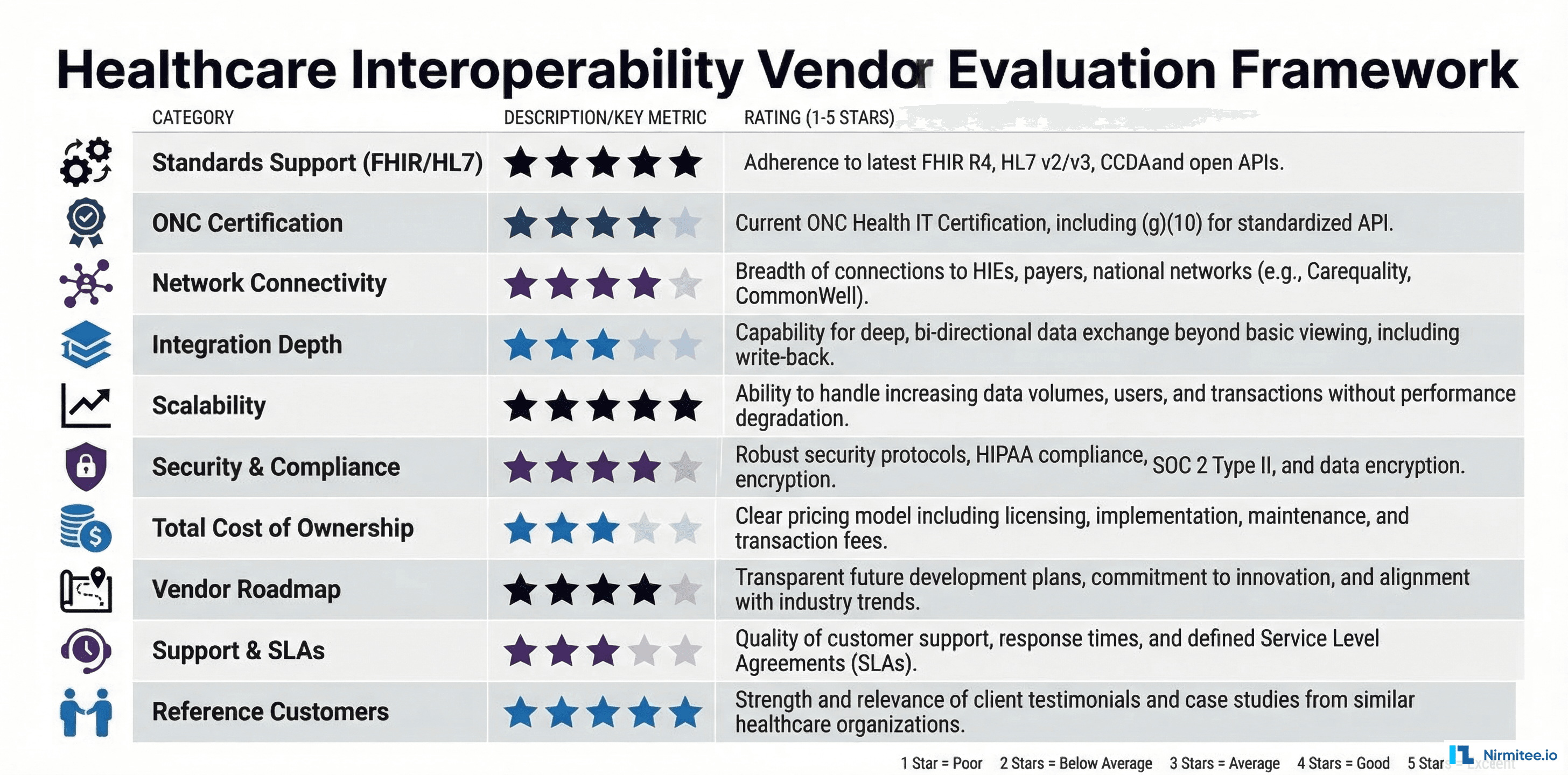
The interoperability layer must handle the reality that US healthcare still runs on a mix of modern FHIR APIs and 1990s-era EDI transactions. Successful agentic systems bridge both worlds. For a deeper dive into this integration challenge, see our guide on healthcare interoperability solutions.
Layer 2: AI/ML Models
The intelligence layer combines multiple model types:
- Large Language Models (LLMs) — GPT-4-class models for clinical documentation understanding, appeal letter generation, and conversational patient engagement. Most production systems use a combination of commercial APIs (OpenAI, Anthropic, Google) and fine-tuned open-source models (Llama, Mistral) for cost optimization.
- Clinical NLU Models — Domain-specific models trained on medical terminology, ICD-10 codebooks, CPT definitions, and payer medical policies. These are typically smaller, faster models optimized for entity extraction and classification.
- Predictive Models — XGBoost/LightGBM models for denial prediction, propensity-to-pay scoring, and workload prioritization. These traditional ML models remain superior to LLMs for structured prediction tasks.
- Embedding Models — For semantic search across medical policy databases, enabling agents to find relevant coverage criteria without exact keyword matches.
Layer 3: Agent Orchestration
The orchestration layer is what makes individual AI capabilities into a coherent agentic system:
- Workflow Engine — Manages the state machine for each revenue cycle transaction, tracking where each claim, authorization, or appeal is in its lifecycle. Tools like Temporal, Apache Airflow, or custom state machines provide durable execution.
- Agent Framework — LangChain, CrewAI, AutoGen, or custom frameworks that provide the agent loop: observe → reason → plan → act → evaluate. The choice of framework significantly impacts the system's ability to handle complex multi-step scenarios.
- Tool Registry — A catalog of actions the agent can take: query eligibility, submit claim, check status, generate letter, send fax. Each tool has defined inputs, outputs, and error handling.
- Memory System — Both short-term (within a single workflow) and long-term (across encounters and patients) memory that enables agents to learn from patterns and improve over time.
Layer 4: Governance and Observability
In a regulated industry like healthcare, the governance layer is not optional — it is a first-class requirement:
- Audit Trail — Every agent decision must be logged with full provenance: what data was accessed, what reasoning was applied, what action was taken, and what outcome resulted.
- Human Override — The ability for authorized users to intervene, correct, or override agent decisions at any point in the workflow.
- Compliance Monitoring — Continuous monitoring for regulatory compliance, including HIPAA (data access patterns), FWA (fraud, waste, and abuse detection), and payer-specific requirements.
- Performance Metrics — Real-time dashboards tracking agent accuracy, throughput, error rates, and financial impact.
For organizations deploying these systems, robust observability is non-negotiable. We have written extensively about observability for agentic AI in healthcare — the monitoring patterns that keep autonomous systems safe and effective.
Vendor Landscape 2026: Who Is Leading the Race
The agentic AI race in healthcare RCM has attracted significant investment and competition. Here is an objective assessment of the leading vendors as of March 2026.

Waystar
Waystar has emerged as the most aggressive mover in agentic RCM, fueled by its strategic partnership with Google Cloud announced in late 2025. The partnership gives Waystar access to Google's Gemini models and healthcare-specific AI infrastructure. Their platform processes over 5 billion healthcare transactions annually, giving them an unmatched dataset for training RCM-specific models.
Key capabilities: End-to-end claim lifecycle automation, AI-powered denial prevention, predictive eligibility verification. Their "Hubble" AI engine now handles autonomous prior authorization for participating payer-provider pairs.
Watch for: Waystar's Google Cloud integration is still early. The promise is significant, but production deployment of their agentic capabilities at scale is expected through 2026-2027.
Adonis
Adonis is the breakout startup story of 2025-2026 in healthcare RCM, achieving 4x revenue growth in 2025. Founded by former Palantir engineers, Adonis built their platform AI-first rather than retrofitting AI onto legacy RCM software. Their approach emphasizes real-time revenue intelligence — continuous monitoring of the revenue cycle with autonomous intervention when anomalies are detected.
Key capabilities: Real-time denial prediction and prevention, autonomous underpayment detection, AI-generated appeal packages. Their platform integrates directly with major EHR systems through FHIR APIs, avoiding the data latency issues that plague traditional clearinghouse-based approaches.
Watch for: Adonis is still scaling. They perform best with mid-size physician groups and specialty practices. Large health system deployments are in pilot phase.
FinThrive
FinThrive (formerly TransUnion Healthcare and Connance) made headlines at HFMA Annual Conference 2025 with their agentic AI demo showing autonomous end-to-end claim processing. Their advantage is deep payer connectivity — they maintain direct integrations with over 1,500 US health plans, giving their agents the ability to interact with payers programmatically rather than through portal scraping.
Key capabilities: Contract management AI, automated underpayment recovery, prior auth automation, and patient financial engagement. Their "Revenue Cycle Intelligence" platform provides predictive analytics overlaid on their transactional processing.
Watch for: FinThrive's legacy platform integration creates complexity. Organizations on their newer cloud platform see better results than those on the legacy stack.
UiPath Healthcare
UiPath brings a different angle — they are an RPA-first company that has layered AI on top. This is actually advantageous in healthcare RCM, where many critical systems lack APIs. UiPath's healthcare practice has built pre-built automation packages for major EHR systems (Epic, Cerner/Oracle Health, MEDITECH) and payer portals.
Key capabilities: Prior auth automation (their strongest use case), claim status checking, eligibility verification, and denial rework automation. Their "AI Center" now provides LLM-powered document understanding that enhances traditional RPA workflows.
Watch for: UiPath's approach is inherently more brittle than API-based solutions — portal layout changes can break automations. However, for organizations with legacy system dependencies, it may be the only viable option.
Enter Health
Enter Health has positioned itself as the AI-native clearinghouse, rebuilding the traditional clearinghouse model with agentic capabilities. Rather than simply transmitting claims, Enter Health's platform actively manages them — scrubbing, optimizing, monitoring, and intervening throughout the claim lifecycle.
Key capabilities: Intelligent claims routing, real-time payer rule updates, automated secondary billing, and AI-powered ERA processing. Their "ClearAI" engine provides per-claim optimization recommendations that are increasingly being applied autonomously.
Watch for: Enter Health is still building its payer network. They perform best in markets where their payer connections are strongest.
Ensemble HP
Ensemble Health Partners has taken a managed services + AI approach, combining human RCM expertise with AI augmentation. Their model is interesting because they own the outcome — they are typically paid on a percentage of collections, aligning their incentives with the health system's results.
Key capabilities: Full RCM outsourcing with AI augmentation, denial management analytics, coding optimization, and patient access automation. Their AI tools are embedded within their managed services workflow rather than sold as standalone software.
Watch for: Ensemble's model works best for health systems willing to outsource significant RCM functions. Organizations wanting to build internal AI capabilities may find their approach limiting.
CMS 2026 Regulatory Requirements: The Compliance Context
Deploying agentic AI in revenue cycle management does not happen in a regulatory vacuum. The regulatory landscape as of March 2026 is the most active it has been in a decade, and organizations must design their AI systems with compliance built in from day one.
CMS Prior Authorization Final Rule (CMS-0057-F)
The most impactful regulation for agentic RCM is the CMS Prior Authorization Final Rule, with key provisions taking effect in 2026:
- March 2026: Health plans must publicly report prior authorization turnaround times, approval/denial rates, and appeal outcomes. This transparency requirement creates public accountability for payer behavior and provides valuable data for AI systems to optimize against.
- 7-day standard decision timeline: CMS has reduced the maximum turnaround time for standard prior authorization decisions from 14 calendar days to 7 calendar days. Urgent requests remain at 72 hours. This compressed timeline makes AI automation not just beneficial but essential for payer compliance.
- Electronic prior auth API requirement: CMS now requires that payers implement FHIR-based Prior Authorization APIs (based on the Da Vinci Prior Authorization Support Implementation Guide). This is a game-changer for agentic AI systems — it provides a standardized, machine-readable interface for prior auth submission and status checking.
State-Level AI Oversight Laws
Multiple states have moved ahead of federal regulation in requiring human oversight for AI in healthcare administrative decisions:
- Texas (SB 2288): Requires that any AI-generated claim denial be reviewed by a licensed clinical professional before being communicated to the provider. Applies to commercial and Medicaid managed care plans operating in Texas.
- Arizona (HB 2847): Mandates that health plans disclose when AI is used in coverage determinations and provides patients the right to request a human review of any AI-influenced decision.
- Maryland (SB 1046): Requires health plans to maintain human oversight committees for AI-driven utilization management and prior authorization decisions, with quarterly reporting to the state insurance commissioner.
These state laws have a practical implication for agentic AI on the provider side: your autonomous agents must be designed with transparent reasoning and full audit trails, because the regulatory environment increasingly demands explainability.
HIPAA and AI
The HHS Office for Civil Rights (OCR) issued updated guidance in late 2025 clarifying that AI systems processing PHI must comply with all existing HIPAA requirements, including:
- Minimum necessary standard: AI agents should only access the PHI required for the specific task at hand — a denial management agent should not have broad access to a patient's full medical record unless the denial specifically requires clinical documentation review.
- Business Associate Agreements: Cloud-based AI services (including LLM APIs from OpenAI, Anthropic, or Google) used to process PHI require BAAs. All major cloud AI providers now offer HIPAA-eligible configurations, but implementation details matter.
- Audit controls: All AI interactions with PHI must be logged in a manner consistent with the HIPAA Security Rule's audit control requirements (45 CFR 164.312(b)).
The Trust Gap
Regulation reflects a broader trust challenge. According to KLAS Research's 2025 survey, 50% of healthcare leaders cite data privacy as the biggest barrier to AI adoption, and 41% say it is difficult to trust AI results fully. These concerns are not irrational — they reflect the legitimate complexity of deploying autonomous systems in a highly regulated, high-stakes environment.
Organizations that address trust proactively — through transparent AI governance, rigorous validation, and clear human oversight protocols — will move faster than those that treat compliance as an afterthought.
Implementation Roadmap: From Pilot to Production
For health system leaders ready to move on agentic RCM, here is a phased implementation roadmap based on patterns observed across successful deployments.
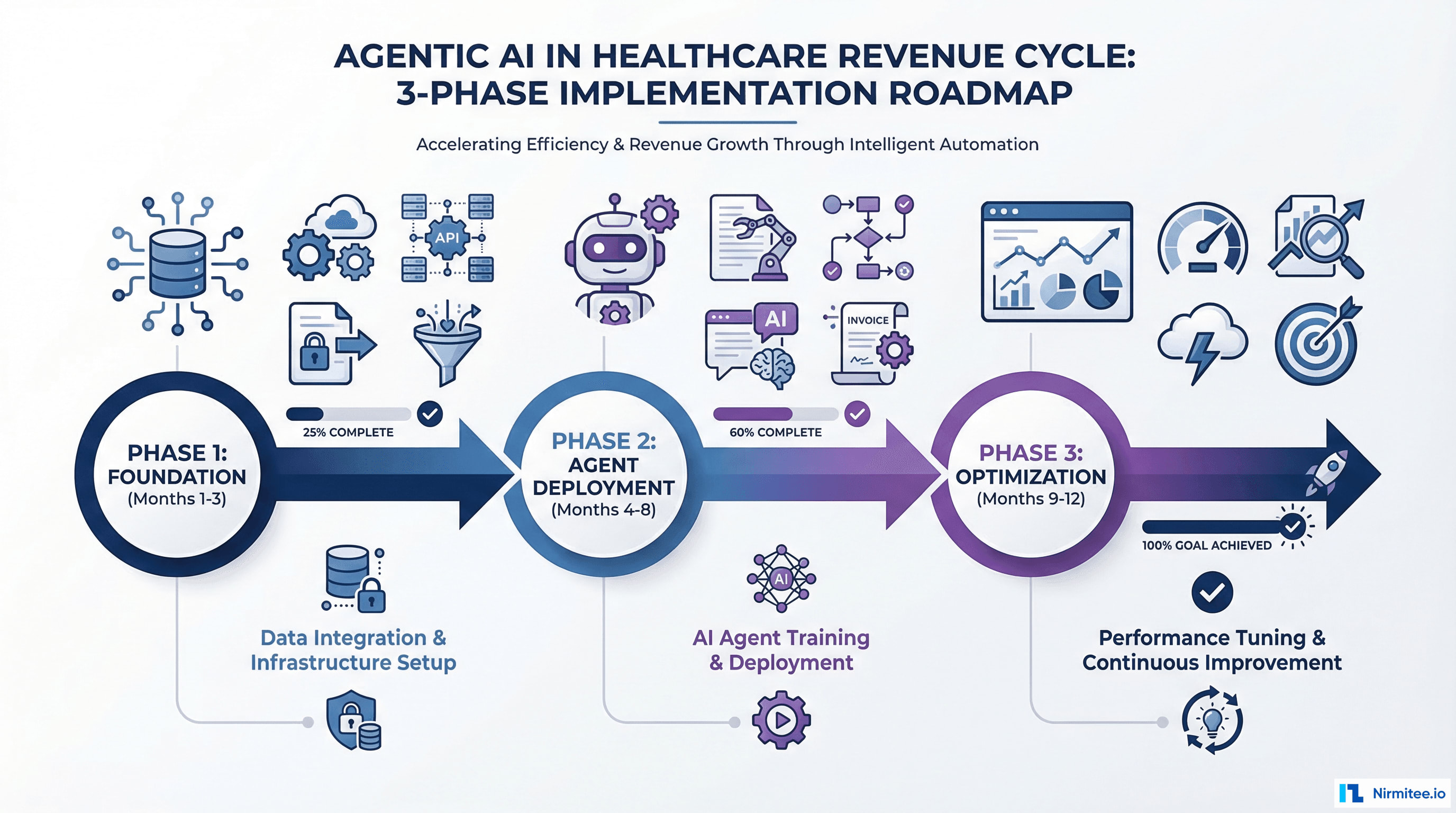
Phase 1: Foundation (Months 1-3)
Objective: Establish the data infrastructure and governance framework that agentic systems require.
Key activities:
- Data audit: Catalog all revenue cycle data sources — EHR, practice management, clearinghouse, payer portals, bank/lockbox. Identify data quality issues, access mechanisms (API vs. file vs. screen scrape), and latency characteristics.
- FHIR API activation: If not already enabled, activate FHIR R4 APIs on your EHR. For Epic, this means enabling the App Orchard APIs. For Oracle Health (Cerner), the Millennium FHIR server. These APIs are the primary data access mechanism for clinical data.
- Governance framework: Establish an AI governance committee with representation from revenue cycle, clinical leadership, compliance, IT, and legal. Define the policies for AI autonomy levels, human override triggers, and performance thresholds.
- Vendor evaluation: Based on your current technology stack, evaluate 2-3 vendors from the landscape analysis above. Prioritize vendors with strong integration capabilities for your specific EHR and payer mix.
- Baseline metrics: Document current performance across key RCM metrics: denial rate, clean claim rate, days in AR, cost to collect, prior auth turnaround, and patient collection rate. These become the benchmarks against which AI impact is measured.
Phase 2: Agent Deployment (Months 4-8)
Objective: Deploy agentic AI for 2-3 high-impact use cases, starting with the highest-ROI, lowest-risk opportunities.
Recommended deployment sequence:
Month 4-5: Eligibility Verification Agent
- Lowest risk, highest volume — an ideal starting point
- Success criteria: 90%+ auto-verification rate, less than 2% error rate
- Deploy in shadow mode for 2 weeks (agent runs but humans still process), then supervised mode (agent processes, humans spot-check), then autonomous mode
Month 5-6: Claims Scrubbing Agent
- Builds on eligibility verification data, extends coverage to pre-submission claim optimization
- Success criteria: 94%+ clean claim rate, measurable reduction in preventable denials
- Deploy with mandatory human review for high-value claims (>$10,000) initially, then progressively increase the autonomy threshold
Month 7-8: Denial Management Agent
- Higher complexity but highest financial impact
- Success criteria: 60%+ appeal success rate, average appeal submission within 72 hours of denial receipt
- Deploy with clinical review for all clinical denials initially, autonomous processing for administrative denials
Phase 3: Optimization and Expansion (Months 9-12)
Objective: Optimize deployed agents, expand to additional use cases, and begin cross-agent orchestration.
Key activities:
- Performance tuning: Analyze agent performance data to identify accuracy gaps, false positive/negative patterns, and edge cases. Fine-tune models and decision thresholds based on real-world results.
- Cross-agent orchestration: Connect the eligibility, claims scrubbing, and denial management agents into a unified workflow where insights from one agent inform the actions of others. For example, denial patterns identified by the denial agent should feed back into the claims scrubbing agent's rules.
- Prior auth deployment: Deploy the prior authorization agent, which is typically the most complex but also the highest-satisfaction use case from a clinical perspective.
- Patient collections: Deploy the patient collections agent, leveraging the financial data now flowing through the automated revenue cycle.
- ROI documentation: Compile comprehensive ROI analysis comparing pre-deployment baselines to current performance. This data is essential for securing budget for continued AI investment and for demonstrating value to the board.
Budget Planning
For a mid-size health system (300-500 beds), expect the following investment range:
- Phase 1: $150,000 - $300,000 (consulting, data infrastructure, governance setup)
- Phase 2: $500,000 - $1,200,000 (vendor licensing, integration, deployment)
- Phase 3: $200,000 - $500,000 (optimization, expansion, additional use cases)
- Ongoing annual: $300,000 - $800,000 (licensing, maintenance, model updates)
Against expected returns of $2-5 million annually in recovered revenue, reduced write-offs, and labor cost avoidance, the ROI case is compelling — typically 3-6 month payback on Phase 2 investments.
What's Next: The Touchless Revenue Cycle
The endgame is not incremental efficiency improvement. It is a fundamental transformation of how healthcare gets paid.
The touchless revenue cycle — where the vast majority of financial transactions flow from service delivery through payment without human intervention — is not a 10-year vision. The building blocks exist today. The question is how quickly individual health systems will assemble them.
Near-term (2026-2027): Agent Specialization
Individual AI agents will become highly specialized and reliable for specific RCM functions. Expect to see eligibility verification and claims scrubbing reach 98%+ automation rates. Prior authorization agents will handle 70-80% of requests autonomously. Denial management agents will draft and submit appeals within hours, not weeks.
Medium-term (2027-2028): Agent Orchestration
The real leap comes when specialized agents are orchestrated into end-to-end workflows. A single patient encounter will trigger a cascade of autonomous actions: eligibility verified, clinical documentation coded, claim scrubbed and submitted, payment posted, patient balance calculated and communicated — all without a human touching the transaction.
This is McKinsey's Level 4 — systemic transformation. It requires not just good individual agents but sophisticated orchestration, robust error handling, and comprehensive governance.
Long-term (2028-2030): Predictive Revenue Cycles
The ultimate evolution is a revenue cycle that is not just reactive but predictive. AI systems will forecast revenue at the point of service delivery, predict payer behavior before claims are submitted, and proactively restructure billing strategies to maximize reimbursement. The revenue cycle will shift from a back-office cost center to a strategic financial intelligence function.
Health systems that begin building their agentic AI capabilities today will be positioned to capture this value. Those that wait will face a widening competitive gap — not just in operational efficiency, but in their ability to attract and retain the clinical and administrative talent that increasingly expects to work with modern technology.
The Strategic Imperative
The $262 billion in annual RCM waste is not just a financial problem. It represents clinical resources that could be deployed for patient care, investments that could be made in community health, and margins that could sustain the financial viability of the US healthcare system.
Agentic AI offers a path to reclaim a significant portion of that waste. The technology is ready. The vendors are competing. The regulatory framework, while still evolving, is supportive. The only variable is organizational willingness to act.
The race to a touchless revenue cycle has begun. The question for every health system leader is not whether to participate, but how quickly to move.
Building agentic AI for revenue cycle operations? Our team specializes in HIPAA-compliant, FHIR-integrated autonomous systems for healthcare. Talk to us →