Gartner reports that roughly 50% of RPA projects fail to deliver expected value, and healthcare's failure rate runs higher because workflow variation is wider. Every claim is a snowflake. Every prior auth has a different format. Yet automation isn't dead — it's just hit a ceiling that pure scripting can't break through.
This blog explains where traditional automation still wins, where it breaks, and where AI agents add capability that RPA fundamentally cannot replicate. For the bigger picture, see our pillar on AI Agents in Healthcare.
What Is "Traditional Automation" in Healthcare?
Rule-based systems, RPA bots, workflow engines, integration platforms — anything deterministic. Given the same input, the same output. These tools are good at repetitive, structured, exception-light work: posting clean ERAs, routing eligibility responses, pushing demographics between systems, generating appointment reminders.
For all of these, you don't want intelligence. You want correctness. RPA delivers correctness cheaply, with a clear audit trail.
Where Traditional Automation Breaks
The problem starts the moment the workflow has variation. Healthcare workflows have variation everywhere — payer rules, EHR conventions, documentation styles, patient situations.
Traditional automation handles variation by exception. Every exception becomes a new branch. Every new branch creates more branches. Within 18 months, the automation has more exception handlers than business logic.
This is why healthcare workflows keep breaking even after automation projects are completed. The bot didn't fail — the workflow grew faster than the rules could.
What AI Agents Add
An agent introduces three capabilities traditional automation can't:
- Reasoning over unstructured data — clinical notes, faxed referrals, scanned forms, free-text claim notes. The agent reads and acts.
- Decision under uncertainty — when the data is incomplete or contradictory, the agent decides what to do next instead of throwing an exception.
- Multi-step planning — break a goal into sub-tasks, execute each, observe results, adjust.
That third capability is the most underestimated. RPA can do step 1, then 2, then 3. An agent can do step 1, observe an unexpected result, decide that step 4 is now right, do that, then circle back to step 2.
A Concrete Side-by-Side: Prior Authorization
An RPA bot can submit a clean prior auth packet. Here's what each system does when the payer responds with "additional documentation required":
| Step | RPA | AI Agent |
|---|---|---|
| Submit packet | Yes | Yes |
| Receive request for more docs | Routes to human queue | Reads the request, identifies what's missing |
| Find the documentation | Human task | Pulls from EHR via FHIR, identifies relevant note sections |
| Format and resubmit | Human task | Drafts response, formats per payer rules, resubmits |
| Cycle time | 3–14 days | Often under 24 hours |
The agent isn't replacing the RPA. The agent is doing the work the RPA couldn't — see Why Prior Authorization Is Broken and What AI Agents Change.
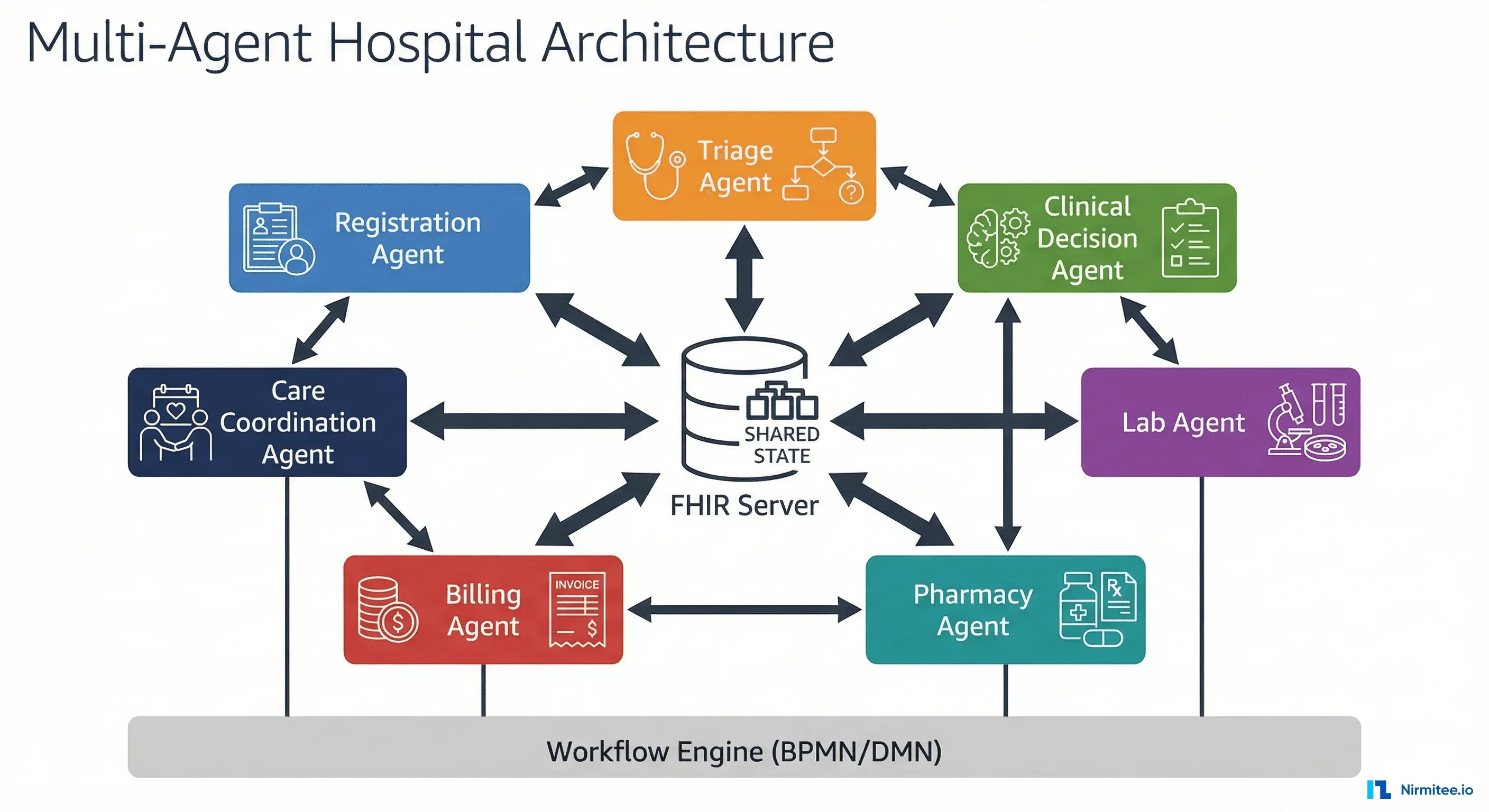
The Right Mental Model: Layers, Not Replacement
The wrong mental model is "agents replace RPA." The right model is layered:
- Deterministic foundation — RPA and workflow engines handle the structured 60–70%.
- Intelligent layer — agents handle the unstructured, exception-heavy 30–40%.
- Human-in-the-loop — for the small fraction that genuinely requires judgment.
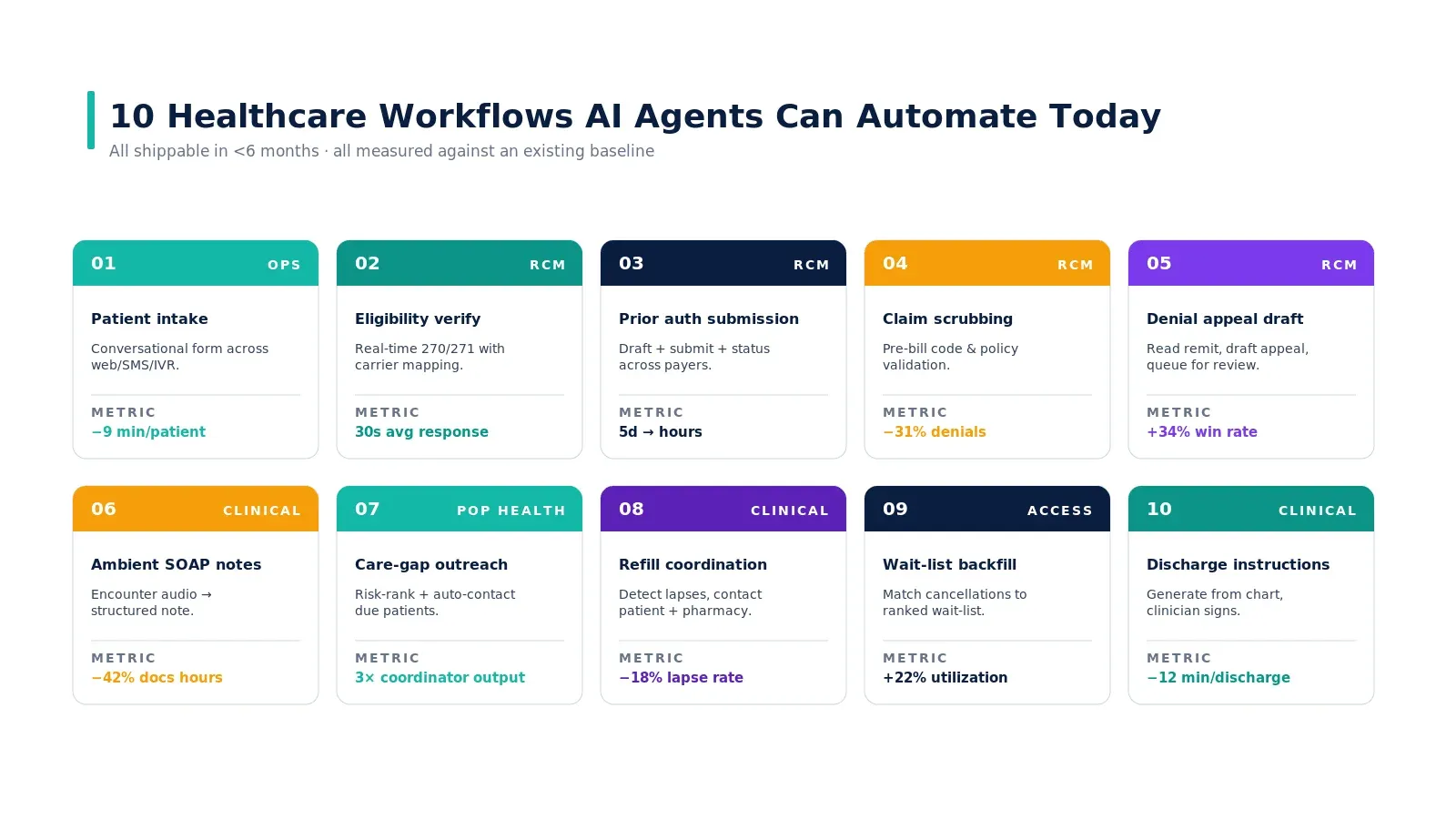
The right starting point is your exception queue. Wherever your existing automation kicks tasks to humans is where agents create the most value, fastest. See 10 healthcare workflows AI agents can automate today for concrete examples.
Real-World Example
The CAQH 2024 Index estimates that the US healthcare industry could save more than $20 billion annually by fully automating administrative transactions. Yet despite a decade of RPA investment, much of that potential remains unrealised because workflows have variation traditional automation can't absorb. Health systems like Geisinger, Intermountain, and Providence have publicly discussed shifting denial management and prior auth to agentic workflows precisely for this reason — automation gets them to the easy 60%, and intelligence is needed for the rest.
Common Pitfalls When Layering Agents on Automation
Teams that try to integrate AI agents with existing RPA stacks consistently hit these traps:
- Replacing RPA with agents wholesale. The deterministic foundation is doing real work. Ripping it out forces the agent to handle structured cases it shouldn't — slower, more expensive, harder to audit. Keep the RPA for what it's good at.
- Skipping the hand-off design. The interesting failure mode isn't the RPA failing or the agent failing — it's the hand-off between them. When does the RPA bot escalate to the agent? When does the agent return control? Without explicit hand-off contracts, both layers end up doing the same work or neither does it.
- Not instrumenting the agent's reasoning. When the agent makes a judgment call that turns out to be wrong, you need to know why. Without observability across the full chain — RPA logs + agent reasoning trace + outcome — you can't debug and you can't trust.
When to Start Layering
The honest test: look at your top 5 RPA exception queues by volume. If three or more of them are "human reads unstructured input and routes," that's the layering signal. Start there. Pilot one workflow end-to-end. Measure cycle time before and after. Then scale. Trying to layer agents everywhere at once is how the project becomes unmanageable.
Most successful deployments we see follow a 3-step progression: prove the architecture on one workflow, expand to 3-5 adjacent workflows, then formalise the layering across the entire ops function.
Key Takeaways
- RPA is fine for structured, exception-light workflows. Don't rip it out.
- Pure automation hits a ceiling because healthcare workflows have variation everywhere.
- AI agents add three things RPA can't: reasoning over unstructured data, decision under uncertainty, and multi-step planning.
- The production-grade architecture is layered: automation + agents + human-in-the-loop.
- Start with your exception queue — that's where agents deliver the fastest ROI.
Call to Action
This blog is one piece of a larger picture. For the full overview, read the pillar guide: What Are AI Agents in Healthcare and How Are They Transforming Care Delivery.
Want to build or evaluate an AI agent for your healthcare product? Get in touch with Nirmitee — we ship FHIR-native, HIPAA-compliant AI agents for US healthtech teams and global hospitals.