Why this guide exists
Most hospital asset management projects fail not because of the software, but because the hardware stack was assembled piecewise. The biomedical team picked the printer. Procurement chose the labels by lowest tender. IT speced the RFID readers. The result: incompatibilities, missed sequencing, and a 6-month commissioning that drags into 14.
This guide is the integrated playbook — printers, labels, RFID tags, readers and antennas — sequenced in the order a hospital should actually buy and deploy them. It applies whether your hospital is in Pune or Pittsburgh, NABH-aligned or Joint Commission-accredited, 200 beds or 1,500.
Step 1: Define your tracking method first — not the printer, not the software
Before any procurement, the hospital must answer one question: how often, and at what scope, do we need to count our assets?
- Annual or quarterly audits, under 1,000 assets: barcode-only is sufficient. Don't over-engineer.
- Monthly audits or 1,000-2,000 assets: hybrid — barcode for stationary equipment, UHF RFID for mobile.
- Daily audits or 2,000+ assets: full UHF RFID with portal readers at zone exits.
- Real-time location for critical-care equipment: BLE tags + Bluetooth gateways. Layered on top of barcode/RFID.
This decision drives every downstream choice — printer class, label material, reader infrastructure, and total program cost.
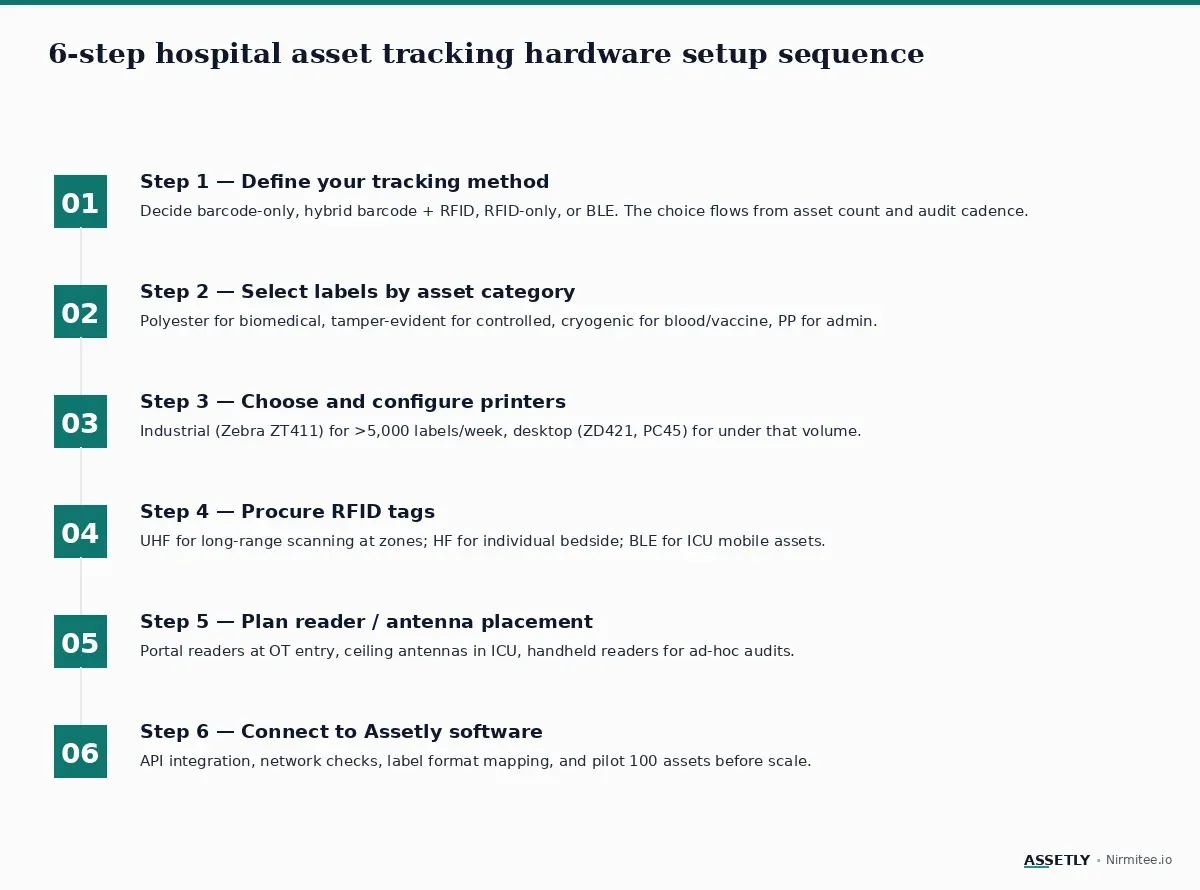
Step 2: Select label material by asset category
Hospitals run 4 distinct label categories in production:
- Polyester barcode/RFID labels (Brady M611, Z-Ultimate 3000T) for biomedical equipment.
- Tamper-evident labels (Brady THT-15-458) for narcotics cabinets and controlled-access assets.
- Cryogenic labels (Lintec) for blood banks, vaccine refrigerators, lab sample storage.
- Polypropylene or paper labels for admin equipment — laptops, projectors, conference room assets.
Don't try to standardise on one label type. Hospitals that do either overspend on admin assets or underspecify on biomedical.
Step 3: Choose printers in matched pairs
The mistake most hospitals make is buying one printer. The right configuration is two: a primary printer for biomedical, and a secondary printer for admin. This prevents downtime on either workflow.
- Primary biomedical printer: Zebra ZD421 (under 1,000 assets) or ZT411 (over 1,000, with RFID encoder if RFID program). Thermal transfer only — direct thermal labels won't survive autoclave.
- Secondary admin printer: Brother QL-820NWB or any low-cost desktop. Direct thermal is fine for short-life admin labels.
Step 4: Procure RFID tags by department workflow
RFID tag selection is workflow-driven, not size-driven:
- UHF RFID (860-960 MHz) — long read range (1-10m). Best for stationary equipment scanned at zone entry/exit (OT, ICU, central stores).
- HF RFID / NFC (13.56 MHz) — short range (10cm). Best for individual bedside check-out at a nurse station.
- BLE tags — battery-powered, real-time location. Best for ICU mobile assets — infusion pumps, ventilators, wheelchairs.
- On-metal RFID tags — special tags for surgical instrument trays and metal-bodied equipment.
Step 5: Plan reader and antenna placement
RFID readers and antennas must be placed before software go-live, not after:
- Portal readers at OT entry, central store loading dock, and biomedical workshop exits.
- Ceiling-mount antennas in ICU and high-traffic corridors for real-time location.
- Handheld readers (1 per 200 assets) for ad-hoc audits and roving biomedical staff.
- Network: PoE-enabled switches at every reader location. Wi-Fi for handhelds.
Step 6: Connect everything to Assetly
The hardware stack is only useful when wired into asset management software. The integration sequence:
- Map label format (barcode symbology, RFID EPC scheme) to Assetly's asset record schema.
- Connect printers via the Assetly print spooler — labels print on asset commissioning, not as a manual step.
- Onboard RFID readers via Assetly's middleware API — reader events stream into the asset event log.
- Pilot 100 assets across 3 departments for 30 days before full rollout. Measure label survival, scan accuracy, and reader read-rate.
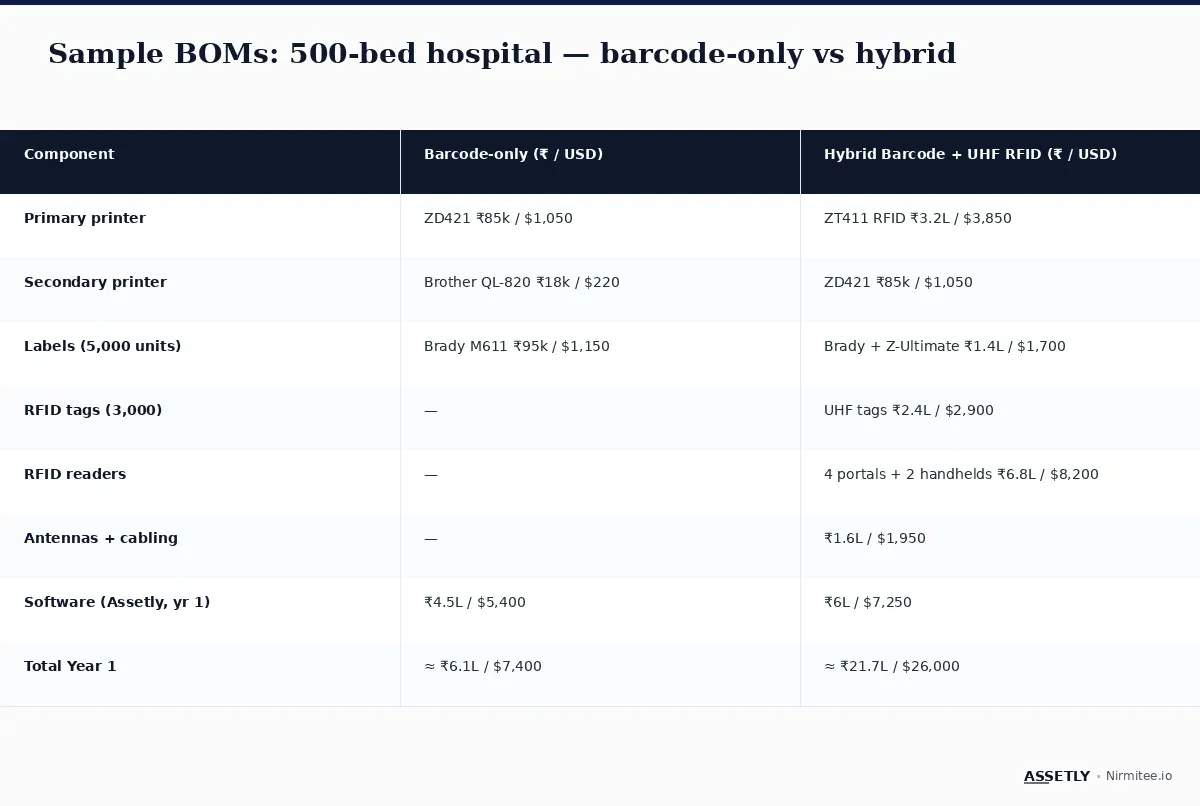
Sample bills of materials
Two reference BOMs for a 500-bed hospital — one barcode-only, one hybrid barcode + UHF RFID. Numbers are 2026 India procurement averages with USD equivalents for global reference.
Real-world: a 700-bed hospital's sequencing mistake
A 700-bed hospital in Maharashtra began its program by purchasing labels first, then realising the labels they bought didn't match the printer's media path. Two months and ₹1.8 lakh ($2,150) wasted. The hospital then bought RFID readers before deciding which RFID tags to use — installing UHF readers when their workflow actually demanded BLE for ICU. Total sequencing cost: ₹4.2 lakh ($5,000) and a 4-month delay. The learning: define tracking method first, then specify hardware in the order this guide outlines.
Key takeaways
- Define your tracking method (barcode / RFID / hybrid / BLE) before procuring any hardware.
- Plan for 3-4 label types, not one. Match each to its asset category.
- Buy two printers, not one — primary biomedical and secondary admin.
- Choose RFID tag type by workflow (UHF for zones, HF for bedside, BLE for ICU mobility).
- Place readers and antennas before software go-live, not after.
- Pilot 100 assets across 3 departments for 30 days before scaling.
Building a hospital asset management program?
Get the sequencing right and the program runs for a decade. Read our pillar guide on healthcare asset management, or talk to the Assetly team about a hardware audit for your hospital.