Every nurse knows the feeling. You came into this profession to care for patients — to hold a hand during a difficult diagnosis, to catch the subtle change in breathing that a monitor misses, to be the human connection in a terrifying moment. Instead, you spend nearly half your shift staring at a screen, clicking through menus, and duplicating information that already exists somewhere in the system.
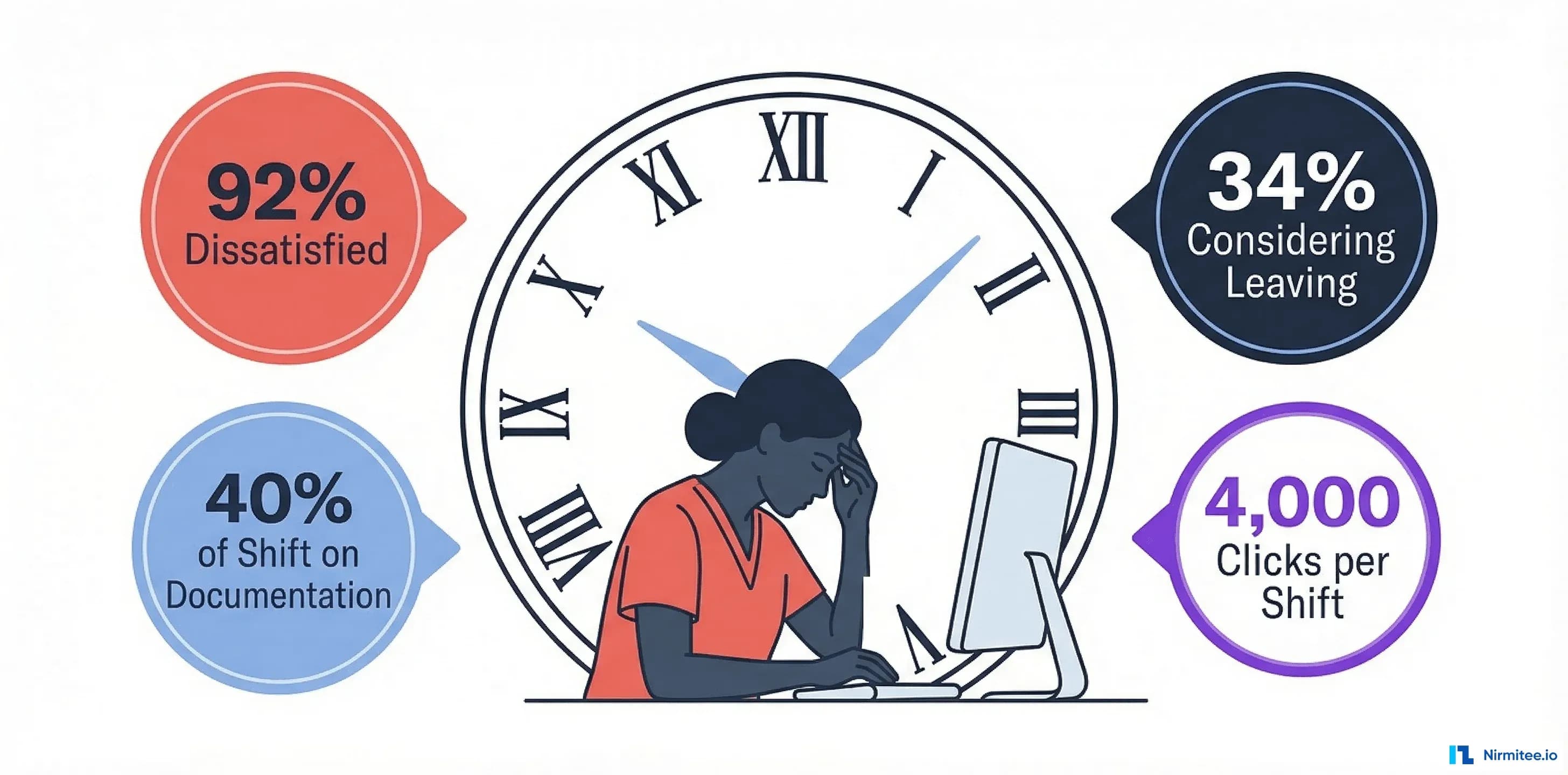
You are not alone. According to Black Book Research's 2025 National Survey, 92% of nurses report that their Electronic Health Record systems have negatively impacted their job satisfaction. That is not a typo — ninety-two percent. And 34% are actively considering leaving their current position within the next year because of EHR-related stress.
This is not a technology complaint. This is a patient safety crisis, a workforce retention crisis, and a financial crisis — all wrapped in a software interface. In this article, we unpack exactly how bad the documentation burden has become, why existing EHR systems perpetuate it, what organizations like UCHealth have done to cut charting time in half, and what architectural and workflow changes actually move the needle.
The Numbers: How Bad Is Documentation Burden in 2026?
Let us start with the data, because the scale of the problem is often underestimated — even by people working in healthcare IT.
Nurses Spend More Time Documenting Than Caring for Patients
A 2024 time-and-motion study published in PMC tracked emergency department nurses minute by minute. The results were stark:
- 27% of shift time spent on EHR tasks (median), compared to just 25% on direct patient care
- Electronic documentation represented 31% of all tasks performed by frequency
- Compared to a 2007 study at the same institution, EHR time had tripled — from 10% to 27% — while direct patient care dropped from 32% to 25%
The Black Book survey paints an even bleaker picture at the national level: 40% of nursing shifts are consumed by documentation rather than direct patient interaction. For a 12-hour shift, that is 4.8 hours of charting.
Physicians Are Charting in Their Pajamas
Nurses are not the only ones drowning in documentation. According to the American Medical Association, 20.9% of physicians spend more than eight hours per week on EHR tasks outside of normal work hours — between 5:30 PM and 7:00 AM. This "pajama time" has remained flat since 2022 despite burnout reduction efforts.
Real-world example: see how we tackled this in production in our case study on addressing healthcare provider burnout with agentic AI.
Primary care physicians spend a median of 36 minutes on the EHR for every 30-minute patient visit — meaning they spend more time documenting the encounter than having it. Per visit, that breaks down to 6.2 minutes of pajama time and 7.8 minutes on the EHR inbox, according to AMA research.
The Retention Crisis Is Real
Documentation burden is not just frustrating — it is driving people out of healthcare:
- 34% of nurses are considering leaving their current position within a year due to EHR stress (Black Book 2025)
- 19% are contemplating exiting nursing entirely
- One-third of burned-out nurses cite EHRs as a major contributor, and 40% of those are likely to leave within two years (KLAS Research 2024)
- Hospitals with high nurse turnover are 3.5x more likely to be rated as using "difficult or outdated" EHRs
The 2025 NSI National Health Care Retention Report puts the average hospital RN turnover rate at 16.4%, with over 138,000 nurses exiting the workforce since 2022. When your EHR is a top-three reason clinicians leave, every percentage point of improvement in usability directly impacts your retention numbers — and your bottom line.
Why Existing EHRs Create Documentation Burden
Understanding the problem requires looking beyond "the software is bad" to the structural reasons EHRs generate so much friction. Most of these issues are not bugs — they are consequences of how these systems were designed and configured.
Click-Heavy Interfaces: Death by a Thousand Clicks
The most infamous example: ordering a single Tylenol in one hospital's EHR required 62 clicks. This is not an edge case — it is what happens when organizational customization layers accumulate without usability testing.
Consider the daily click burden:
- A typical ER shift involves approximately 4,000 mouse clicks
- Navigating to a patient chart takes 8-12 clicks depending on the system
- Documenting a single set of vital signs requires 15-20 clicks
- Each medication order can require 14-62 clicks depending on hospital configuration
Research published in the Journal of the American Medical Informatics Association found that the quality of medical residents' documentation actually decreased as the number of dialog boxes increased — a direct consequence of mouse-click fatigue. Clinicians are not just slow; they are making worse documentation when the interface fights them.
Duplicate Documentation: Entering the Same Data Three Times
One of the most demoralizing aspects of modern EHR use is the feeling that you are typing the same information into multiple places. A nurse records vital signs on a paper flowsheet at the bedside, enters them into the EHR, and then a physician documents them again in their note. The same medication list appears in the nursing assessment, the physician's H&P, the discharge summary, and the medication reconciliation form.
This happens because most EHR systems were built as document-oriented rather than data-oriented systems. Each clinical note is treated as a standalone artifact rather than a structured query against a shared clinical data model. The result: the same blood pressure reading might exist in four different places in the chart, with no guarantee they match.
Black Book found that 88% of nurses report their EHR systems create inefficiencies and redundancies in clinical workflows. The duplication is not laziness — it is architecture.
Alert Fatigue: 56 Alerts Per Day, 49 Minutes Responding
Clinical decision support (CDS) alerts were designed to prevent medication errors and catch dangerous interactions. In practice, they have become one of the largest sources of documentation interruption. According to research cited by the Journal of the American Medical Informatics Association:
- Primary care clinicians receive an average of 56 alerts per day
- Responding to those alerts consumes 49 minutes daily
- Override rates exceed 90% for most alert types — meaning clinicians dismiss almost all of them
- In one study, the same alert fired 70 times for a single provider without once driving the desired action
When 90%+ of alerts are overridden, the system has trained clinicians to click through everything — including the rare genuinely dangerous interaction. This is not a documentation problem alone; it is a patient safety problem created by documentation design.
Poor Mobile and Bedside Experience
Despite healthcare being a fundamentally mobile profession — nurses walk 4-5 miles per shift — most EHR systems were designed for desktop workstations. Charting at the bedside often means wheeling a COW (computer on wheels) into the room, logging in (again), finding the patient (again), and navigating to the right screen while the patient waits.
The login problem alone is significant. Nurses at busy units may log in and out of the EHR 70+ times per shift as they move between patients and workstations. Each login sequence takes 15-30 seconds — adding up to 15-35 minutes per shift just on authentication.
Modern mobile-first interfaces with proximity-based authentication (badge tap, biometric) and role-based dashboards could eliminate this entirely. Yet most hospitals are still running desktop-era interfaces on rolling carts.
What UCHealth Did to Cut Charting Time by 50%
It is easy to catalog problems. What is harder — and more valuable — is understanding what actually works. UCHealth, a major health system using Epic, achieved a 50% reduction in documentation time and a 75% improvement in nurse satisfaction through a multi-pronged approach that did not require replacing their EHR.
What They Changed
According to a retrospective study published in PMC and UCHealth's own case study, their approach included:
- Redesigned training from classroom to virtual + hands-on: New hires gained Epic access after just 4 hours of initial training, getting them to the floor faster with ongoing micro-learning modules
- Epic SmartUser personalization program: Over 1,000 nurses enrolled since May 2025. Participants learned to customize their personal EHR settings — Quick Actions, favorites, personalized templates — to match their specific workflows
- Role-specific template customization: Rather than one-size-fits-all documentation templates, UCHealth created tailored views for different nursing specialties (ICU, ED, med-surg, L&D)
- Workflow optimization with clinician input: Nurses were included in EHR governance decisions, not just consulted after the fact
The Results
Time spent in the Notes module per day dropped from 56.6 minutes to approximately 29 minutes — a 50% reduction at 3 months post-training. Nurses reported saving 10-15 minutes per shift after completing SmartUser courses.
The key insight: the EHR itself did not change. The same Epic instance, the same version, the same modules. What changed was how it was configured, how clinicians were trained, and whether nurses had a voice in workflow design. This suggests that a significant portion of documentation burden is organizational, not purely technological.
Lessons for Other Health Systems
- Invest in personalization, not just implementation: Most EHR rollouts focus on go-live. UCHealth showed that ongoing optimization matters more than initial deployment
- Give nurses a seat at the table: Black Book found that Magnet-designated hospitals — which emphasize nurse leadership — had 87% of nurses rating EHRs as supportive, versus just 21% at non-Magnet facilities
- Measure what matters: UCHealth tracked actual time-in-module, not just satisfaction surveys. Objective metrics drove real improvements
How EHR Architecture Drives Usability
Workflow optimization and training can achieve significant gains — but they have limits. Ultimately, the architecture of an EHR determines the ceiling of usability improvement. A system built on a 1990s document model will always require workarounds that a modern data-oriented architecture would not.
API-First Design Enables Custom Workflows
Legacy EHR systems treat customization as "configuration within the vendor's UI." Modern API-first architectures treat the EHR as a data platform that multiple interfaces can consume. This distinction matters enormously for documentation burden.
With a robust API layer, health systems can:
- Build role-specific interfaces: A triage nurse sees a streamlined intake screen. An ICU nurse sees a real-time monitoring dashboard. A charge nurse sees staffing and throughput. Same data, different views — no clicks wasted navigating to irrelevant modules.
- Automate data pre-population: When a patient arrives, their demographics, allergies, active medications, and recent labs auto-populate from the shared data layer. No re-entry.
- Integrate bedside devices directly: Vital signs from monitors flow into the chart without manual transcription — eliminating one of the most time-consuming and error-prone documentation tasks.
This is the approach behind modern EHR development — building the data layer right so the interface layer can flex to clinical needs.
FHIR Reduces Documentation Duplication
FHIR (Fast Healthcare Interoperability Resources) is not just an interoperability standard — it is an architecture pattern that can fundamentally reduce documentation duplication. When clinical data is stored as discrete FHIR resources (Observations, Conditions, MedicationRequests), it exists once and can be referenced from any document or view.
Consider a patient's blood pressure:
- Legacy approach: The nurse types "BP 138/82" into a nursing note. The physician types "hypertensive, BP 138/82" into their assessment. The discharge planner copies it into the discharge summary. Three entries, three potential transcription errors.
- FHIR approach: The nurse creates a single
Observationresource with systolic=138 and diastolic=82. The physician's note references that Observation. The discharge summary pulls it automatically. One entry, zero duplication.
According to HIMSS survey data, FHIR-based integrations reduce implementation time by 40% compared to legacy HL7 interfaces while providing superior data access. For documentation specifically, the structured data model means information entered once propagates everywhere it is needed.
Ambient AI + Structured Data: The Emerging Solution
The most promising technology for reducing documentation burden is ambient AI documentation — systems that listen to the clinical encounter and generate structured notes automatically. Early adopters are reporting 30-50% reductions in documentation time with improved note quality.
But ambient AI works best when it generates structured data, not just free text. A system that converts a physician-patient conversation into both a readable note AND discrete FHIR resources (diagnoses, medications, orders) eliminates the need for separate coding, order entry, and problem list updates.
The key architectural requirement is a clinical data repository that can ingest structured output from AI systems and make it available across all clinical workflows. This is where the choice between modern clinical data platforms and legacy document-oriented EHRs becomes critical.
The 5 EHR Features That Actually Reduce Documentation Time
Based on the research, case studies, and architectural analysis above, these are the five features with the strongest evidence for reducing clinical documentation burden.
1. Smart Defaults and Pre-Populated Fields
Every field that auto-populates is a field a clinician does not have to fill in manually. Effective smart defaults include:
- Context-aware order sets: When a nurse documents a patient with chest pain, the most likely orders (troponin, ECG, aspirin) should be one click away — not buried in a catalog of 50,000 orderable items
- Pre-populated vital sign ranges: Normal ranges for the patient's age and condition auto-fill, requiring the nurse to only enter the actual value
- Auto-populated medication reconciliation: The current med list from pharmacy feeds the reconciliation form, requiring only confirmation rather than re-entry
Organizations that implement comprehensive smart defaults report 30-40% reductions in clicks per encounter.
2. Voice and Ambient Documentation
Voice-to-text has existed for decades, but modern ambient AI goes far beyond simple dictation. Current-generation systems can:
- Generate structured clinical notes from conversational speech during the patient encounter
- Extract discrete data elements (diagnoses, medications, procedures) and populate the appropriate EHR fields
- Draft after-visit summaries in patient-friendly language
- Pre-fill billing codes based on the documented encounter
Clinicians at organizations using Epic's AI tools are completing discharge summaries 20-30% faster, and Riverside Health reported clinicians spending up to 32% less time on documentation and communication tasks.
3. Role-Based Configurable Templates
A one-size-fits-all documentation template guarantees that everyone wastes time. An ICU nurse documenting a ventilated patient has entirely different needs than an outpatient clinic nurse documenting a well-child visit. Effective template systems offer:
- Specialty-specific default views that load automatically based on unit and role
- User-configurable Quick Actions for the 10-15 most common tasks per role
- Conditional logic that shows or hides fields based on clinical context (e.g., pregnancy-related fields only appear for OB patients)
4. Intelligent Alert Management
Reducing alert fatigue requires more than turning off alerts — it requires making alerts smarter. Evidence-based approaches include:
- Tiered severity: Only truly dangerous interactions (e.g., life-threatening drug-drug interactions) generate hard stops. Low-severity alerts appear as passive information, not modal dialog boxes
- Role-based filtering: A pharmacist sees drug interaction details. A nurse sees dosing guidance. Neither sees alerts irrelevant to their role
- Frequency capping: If a clinician has overridden the same alert for the same patient 3 times, stop showing it. The clinical decision has been made
- Contextual suppression: Alerts about renal dosing adjustments should not fire for patients with normal kidney function
Organizations that implement tiered alert systems report 40-60% reductions in alert volume with no increase in adverse events — because the remaining alerts are actually relevant and actionable.
5. Single Sign-On and Proximity Authentication
This seems mundane compared to AI-powered documentation, but it may have the highest ROI per dollar spent. If nurses log in 70+ times per shift and each login takes 20 seconds, that is 23+ minutes per shift on authentication alone. Solutions include:
- Badge-tap authentication: Tap an ID badge to log in instantly at any workstation
- Biometric login: Fingerprint or facial recognition at shared terminals
- Session roaming: A nurse's session follows them from workstation to workstation. Walk up to a new COW, tap your badge, and your patient chart is already open
- Automatic timeout with fast resume: Sessions lock after inactivity for HIPAA compliance but resume instantly with badge tap
An EHR Buyer's Usability Checklist
If you are a CNO, CMIO, or CIO evaluating EHR systems — or negotiating an optimization engagement with your current vendor — here is what to demand. This is not a wish list; every item on it has demonstrated evidence for reducing documentation burden.
| Requirement | Why It Matters | Questions to Ask the Vendor |
|---|---|---|
| Mobile/tablet support at bedside | Eliminates the COW bottleneck; enables documentation at point of care | Can nurses chart on an iPad at the bedside with full functionality? |
| Customizable templates by role and specialty | Reduces irrelevant fields; 30-40% click reduction | How many organizations have built custom nursing templates? Show me examples. |
| Voice/ambient documentation support | 20-50% reduction in documentation time | What ambient AI partnerships exist? What is the accuracy rate in production? |
| Smart defaults and context-aware pre-population | Eliminates redundant data entry | How many clicks to order the 10 most common medications? Show me the workflow. |
| FHIR R4+ API for custom workflows | Enables third-party innovation; avoids vendor lock-in | What percentage of clinical data is accessible via FHIR APIs? Is write-back supported? |
| Configurable alert severity tiers | Reduces 56 daily alerts to actionable subset | What is the current override rate? Can we configure severity tiers by clinician role? |
| Single sign-on with proximity/biometric auth | Saves 15-35 min/shift on authentication | Do you support badge-tap login and session roaming between workstations? |
| Clinician-led governance program | UCHealth: 50% reduction when nurses have input | What is your recommended model for ongoing clinician optimization governance? |
Red Flags During an EHR Demo
- The demo shows a physician workflow but not a nursing workflow
- Click counts for common tasks are not disclosed or benchmarked
- Alert configuration is described as "admin-managed" with no clinician input
- Mobile support is "on the roadmap" rather than in production
- FHIR access is limited to read-only or a subset of resources
- Template customization requires vendor professional services (not self-service)
The Path Forward: Making Documentation Serve Clinicians
The 92% dissatisfaction rate is not a technology problem that a single product can solve. It is a systems problem that requires coordinated action across technology, training, governance, and organizational culture.
Here is what the evidence tells us works:
- Optimize what you have: UCHealth's 50% reduction came from training and personalization, not a new system. Start here — it is faster and cheaper than replacement.
- Put nurses in charge of nursing workflows: Magnet hospitals with nurse-led EHR governance see 4x higher satisfaction rates. Stop designing nursing documentation by committee without nurses.
- Invest in architecture, not just interfaces: FHIR-based data models, API-first design, and structured clinical data repositories eliminate duplication at the root. This is the long-term play that pays dividends across every workflow.
- Deploy ambient AI strategically: Start with the highest-burden documentation tasks (H&Ps, discharge summaries, progress notes) and expand based on measured time savings.
- Measure relentlessly: Track time-in-EHR, clicks-per-task, pajama time hours, and alert override rates. If you are not measuring it, you are not improving it.
At Nirmitee, we build custom EHR platforms and healthcare integration solutions designed around clinician workflows — not the other way around. Our API-first, FHIR-native architecture ensures that data flows where it needs to go without manual re-entry, and our ambient AI integration capabilities bring documentation into the conversation rather than making it a separate task.
Documentation should serve clinicians. Clinicians should not serve documentation. If your current EHR has that equation backwards, it is time to explore what a purpose-built, clinician-centered platform can do.
Ready to reduce your documentation burden? Talk to our healthcare engineering team about building an EHR experience your nurses will actually want to use.
Building production-grade healthcare AI agents requires careful architecture. Our Agentic AI for Healthcare team ships agents that meet clinical and compliance standards. We also offer specialized Custom Healthcare Software Development services. Talk to our team to get started.