Electronic health records are no longer a nice to have digital filing cabinet; they have become the backbone of modern care delivery, reimbursement, and regulatory compliance.
Nearly all non-federal acute care hospitals in the United States now use a certified electronic health record system, with adoption rates hovering around ninety-six percent, and more than three-quarters of office-based physicians relying on certified platforms in daily practice.
Globally, the electronic health records market is expected to grow from roughly 28 - 36 billion USD in 2025 to more than 44 billion USD by 2034, driven by steady investment in digital health infrastructure, cloud-based delivery models, and regulatory incentives.
At the same time, initiatives such as TEFCA in the United States and the Ayushman Bharat Digital Mission (ABDM) in India are pushing the sector toward a world where records move seamlessly across networks and providers, with strong consent and data-protection frameworks baked in from the start.
Against this backdrop, building or modernizing an EHR product in 2026 is both a significant opportunity and a serious engineering challenge. Many organizations still struggle with legacy platforms that clinicians dislike, data models that cannot cope with modern analytics, and rigid architectures that make interoperability or scaling painful.
Others are starting from scratch and want to avoid repeating the mistakes of the previous generation.
This guide walks through the end-to-end landscape of EHR software development for 2026: how to think about EHR versus EMR, when to choose custom development instead of an off-the-shelf package, which capabilities matter most, how to architect the solution, where interoperability and regulation fit in, and what to realistically expect in terms of cost, timelines, and vendor selection.
EHR vs EMR in 2026 — getting the foundation right
The terms EHR and EMR still get used interchangeably, yet the distinction is more important than ever because it shapes your product strategy, your data model, and your integration roadmap.
1.1 What an EMR really is
An electronic medical record is essentially the digital successor of a paper chart maintained by a single clinic or facility. It holds information created and used within one organization: diagnoses, progress notes, medications, immunizations, and procedure histories for visits handled by that practice.
In other words, EMR systems are:
- Practice-centric: focused on one clinic, one organization, or one tightly defined network.
- Transaction-focused: optimized around orders, encounters, and documentation for that particular site.
- Limited in exchange: some export or sharing may exist, but they are not designed as the primary fabric for regional or national data exchange.
If you are building a platform purely for a single clinic chain or a niche specialty group that does not need heavy cross-organization exchange, you may still label it an EMR and be done. However, most markets are moving beyond this.
1.2 What an EHR must be in 2026
An electronic health record is a longitudinal, patient-centric view of health that spans multiple providers, care settings, and time periods. It aggregates demographics, allergies, medications, problem lists, lab results, imaging, procedures, social determinants, and care plans from different facilities, networks, or even regions.
Key characteristics of a modern EHR:
- Patient-centric and longitudinal rather than visit-centric; it follows the individual across hospitals, clinics, laboratories, and digital tools.
- Interoperable by design, using standards such as HL7 v2, FHIR, and DICOM, and participating in frameworks like TEFCA or ABDM federated exchanges where applicable.
- Multi-stakeholder: built to serve clinicians, patients, payers, and regulators, each with distinct views and permissions.
If you are planning a product for 2026 and beyond, it is almost always wiser to architect for EHR-level
interoperability from day one, even if your first release looks like an EMR in scope. The regulatory and
market direction is clearly toward integrated health ecosystems and longitudinal records rather than siloed charts.
Custom vs off-the-shelf EHR: Which path should you choose?
Once the EHR vision is clear, the next decision is whether to buy an existing product or build (or heavily tailor) your own. There is no single correct answer; the right choice depends on your scale, specialization, regulatory context, and long-term strategy.
2.1 When an off-the-shelf platform makes sense
A pre-built EHR from a major vendor or regional specialist can be attractive when:
- You need rapid deployment for compliance or basic digitization.
- Your workflows are relatively standard (primary care, general hospital, ambulatory clinics with textbook workflows).
- You do not have an internal engineering organization dedicated to health-tech, and you prefer a subscription model with vendor-managed updates.
Off-the-shelf products tend to come with certified modules for ordering, e-prescribing, basic interoperability, and reporting out of the box. For organizations that simply want to move off paper and satisfy regulatory incentives, this can be the pragmatic path.
However, once you start demanding deep specialty support, highly customized pathways, or heavy integration with your own digital front door, off-the-shelf solutions often become complex and expensive to bend into shape.
2.2 When custom EHR development is the better option
Custom or heavily tailored EHR development becomes the smarter choice when:
- You operate in specialty care (oncology, fertility, behavioral health, complex surgery, home health, occupational health) with unique documentation and workflows.
- You are a digital health product company or health-tech startup that wants to differentiate on clinician experience, workflow automation, or patient engagement.
- You need tight integration with national frameworks and bespoke systems, such as ABDM in India, insurer platforms, lab networks, or bespoke clinical decision support tools.
- You expect frequent product iteration and want the EHR to evolve alongside your business rather than being constrained by a vendor roadmap.
Custom development demands more effort and governance, but it lets you encode your unique care model into software instead of forcing clinicians and patients to adapt to generic screens designed a decade ago.
2.3 A hybrid approach
Many organizations succeed with a hybrid pattern:
- Start with a stable, certified core (for example, a commercially available EHR or an open-source backbone).
- Surround it with custom modules, microservices, and experience layers that deliver the differentiated workflows, analytics, and integrations you actually care about.
This approach preserves regulatory compliance and accelerates go-live while still giving you enough room to innovate at the edges.
Essential capabilities for a 2026-ready EHR platform
Regardless of whether you build or buy, any EHR that expects to be relevant in 2026 should deliver a certain baseline of capabilities. Think of these as the table stakes for safe, efficient, and compliant care.
3.1 Comprehensive patient management
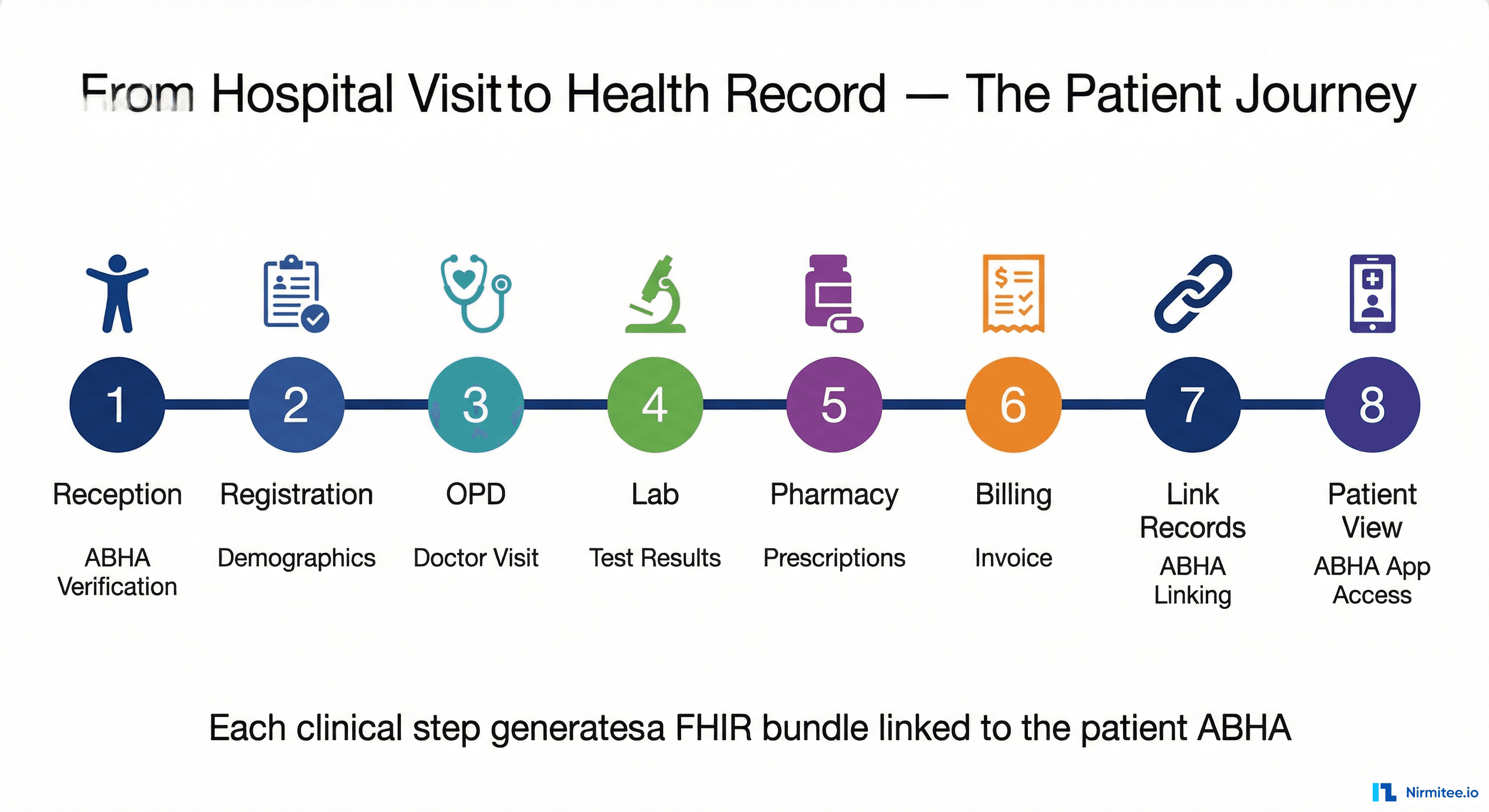
At the heart of the system lies a robust patient master record, able to handle identity resolution across multiple sources, duplicate detection, and linkage to national identifiers where applicable (such as ABHA numbers in India or local patient identifiers elsewhere).
This involves:
- Rich demographic and contact details with support for multiple addresses and phone numbers.
- Allergy, problem, and medication lists maintained over time rather than overwritten, with complete version history.
- Support for multiple insurance coverages, guarantors, and payer relationships.
The data model must gracefully handle patients with fragmented histories, cross-border care, or complex social histories without becoming a tangle of free-text notes.
3.2 Appointment and resource scheduling
Scheduling is no longer a simple calendar feature; it is the backbone of access and capacity management. A modern EHR should coordinate:
- Provider calendars across locations, including teleconsultation windows.
- Room, equipment, and procedure slot booking.
- Wait-lists, overbooking rules, and automated reminders via SMS, email, or in-app notifications.
In high-volume settings, the scheduling module should work alongside triage rules to prioritize high-risk patients, post-discharge follow-ups, or chronic disease reviews instead of blindly filling slots on a first-come, first-served basis.
3.3 Clinical documentation that clinicians actually use
Documentation has historically been the source of most clinician frustration. For 2026-ready systems, the expectations are far higher:
- Template-driven notes that adapt to specialty, visit type, and context rather than one giant generic form.
- Structured capture of problems, procedures, and findings using standard terminologies such as SNOMED CT, LOINC, and ICD for analytics, reporting, and interoperability.
- Support for rich media such as diagrams, images, and annotated scans within the encounter note.
- Smart defaults, autopopulation of known values, and context-aware prompts to minimize repetitive data entry.
The goal is not to increase the number of fields but to help clinicians document complex encounters quickly without relying on copy-paste or free-text shortcuts.
3.4 Order entry, e-prescribing, and results management
Order entry should include diagnostic tests, procedures, referrals, and medications, with clear order sets for common conditions.
For prescriptions, the system should:
- Check for drug - drug and drug - allergy interactions.
- Validate formulary rules and prior authorization requirements where applicable.
- Support electronic transmission to pharmacies or dispensing units and capture fulfillment status.
Results management must give clinicians a single, unified place to see labs, imaging, and other diagnostics, including:
- Critical value alerts.
- Longitudinal visualization of results.
- Tools to acknowledge, annotate, and document follow-up actions.
3.5 Billing, coding, and revenue cycle integration
In most health systems, financial workflows are tightly intertwined with clinical documentation. The EHR must therefore:
- Support structured coding of diagnoses and procedures using ICD, CPT, or local coding systems.
- Generate claims or invoices using rules based on encounter type, coverage status, and bundled payment logic.
- Integrate with external billing systems, payer portals, or national schemes, with clear reconciliation and denial-tracking workflows.
In markets shifting toward value-based care, the revenue cycle must also support outcome metrics rather than only fee-for-service billing.
3.6 Patient portal and engagement features
Patients increasingly expect seamless digital access to their health information. Modern EHR platforms should offer:
- A secure portal or mobile app with access to visit summaries, lab results, immunization records, and prescriptions.
- Self-service scheduling, rescheduling, and cancellation.
- Digital consent management so patients can manage sharing permissions across providers, aligned with frameworks like ABDM's consent model.
A well-designed portal becomes a collaborative space between clinicians and patients rather than a static information repository.
3.7 Reporting and operational analytics
EHRs gather massive amounts of structured data. Without strong analytics, this becomes a wasted asset. A capable reporting layer should:
- Provide operational dashboards (patient volumes, wait times, occupancy, billing performance).
- Surface quality and safety indicators (readmissions, adverse events, missed follow-ups).
- Allow export and integration with external analytics systems or data warehouses.
In mature organizations, this evolves into real-time monitoring of patient flow, staffing, and resource utilization to drive continuous improvement.
Advanced Capabilities
Once the fundamentals are stable, the real competitive differentiation comes from how the EHR helps clinicians make better decisions, reduces administrative burden, and supports new models of care.
4.1 Clinical decision support built on real-world data
Modern decision support is moving away from static rule libraries and toward engines that blend clinical guidelines with real-world patterns. Effective platforms combine:
- Rules for medication dosing, contraindications, and preventive care reminders.
- Pathway guidance for chronic conditions and complex procedures, tailored to local protocols.
- Early-warning scores for sepsis, deterioration, or readmission risk, derived from historical data trends.
The challenge is to embed these tools in a way that supports clinicians without overwhelming them with alerts. This requires thoughtful governance, explainability, and continuous monitoring for potential bias.
4.2 Remote monitoring and connected devices
Continuous data from wearables, home monitoring devices, and digital therapeutics is becoming routine in many health systems. A 2026-ready EHR should be able to:
- Ingest structured streams such as blood pressure, glucose levels, weight, sleep, and activity data from trusted devices.
- Highlight exceptions instead of raw data dumps - for example, flagging patterns that signal worsening control of a chronic condition.
- Provide configurable dashboards for virtual wards, chronic disease programs, or home-health teams.
This requires strong consent handling, personalized thresholds, and clear escalation workflows so clinicians receive actionable insights instead of noise.
4.3 Intelligent automation for administrative workflows
Much of the administrative load in healthcare comes from repetitive documentation and clerical tasks. Next-generation EHR systems reduce this by:
- Auto-extracting key information from structured and semi-structured documents.
- Supporting smart scheduling suggestions based on predicted slot demand and patient risk.
- Streamlining coding and billing workflows with upfront checks that prevent common claim errors.
While these features rely on advanced pattern recognition behind the scenes, the user experience should feel intuitive - as if the system simply anticipates the next required action.
4.4 Telehealth deeply integrated with core workflows
Telehealth is no longer a standalone feature. In a modern EHR:
- Remote visits are treated as first-class encounter types with full documentation, orders, and billing.
- Scheduling, reminders, and virtual waiting rooms are fully integrated.
- Consent, identity verification, and recording policies reflect local regulatory requirements.
When telehealth is woven naturally into the care workflow, organizations can expand reach and manage capacity without fragmenting patient records across separate systems.
Architecture and tech stack decisions that age well
Technology choices for an EHR have long-term consequences; the platform you design now will still be in production many years from today. The goal is not chasing fashionable frameworks, but choosing an architecture that remains maintainable, secure, and adaptable.
5.1 Modular, service-oriented architecture
Monolithic applications become hard to evolve as regulations, workflows, and integrations change. A modular design, whether based on microservices or well-structured modules within a monolith, should:
- Separate concerns such as identity, scheduling, documentation, orders, billing, and analytics.
- Use clear, versioned internal APIs, enabling teams to update or replace modules independently.
- Support horizontal scaling for high-load components such as order entry or patient portals while keeping lower-volume modules lighter.
The right level of granularity depends on your team and deployment environment; over-fragmentation can be as damaging as a giant ball of mud.
5.2 Backend technologies
On the server side, languages and frameworks such as Java, .NET, Python, or Node.js remain common choices in healthcare because of their ecosystem maturity, security tooling, and scaling characteristics. The specific choice matters less than:
- The team's familiarity with the stack.
- The availability of libraries and tooling for interoperability standards (FHIR servers, HL7 parsers, DICOM toolkits).
- Long-term support and compatibility with your hosting environment, whether on-premises or cloud.
For high-throughput scenarios such as event streams or large-scale analytics, technologies like Kafka and columnar databases can complement the transactional core.
5.3 Frontend and user experience
Clinician experience is now a competitive differentiator. A modern EHR frontend typically uses:
- Component-based frameworks such as React, Angular, or Vue to deliver responsive, role-aware interfaces.
- Design systems that enforce consistency across modules, including typography, spacing, iconography, and interaction patterns.
- Offline-tolerant modules for environments with unstable connectivity, particularly in home-care or rural settings.
The most important investment is rigorous UX research with real clinicians, patients, and administrative staff, rather than guessing at screen layouts in isolation.
5.4 Data storage and persistence
Transactional data is usually best stored in relational databases such as PostgreSQL or MySQL for strong consistency and familiar querying.
However, a complete EHR landscape often includes multiple data stores:
- Relational databases for core clinical and financial records.
- Document or key-value stores for audit trails, configuration, and unstructured attachments.
- Data warehouses and lakehouses for longitudinal analytics, population health, and research.
The key is to define clear boundaries: which data live where, how they are synchronized, and how data lineage and provenance are tracked.
5.5 Cloud, hybrid, or on-premises
Cloud platforms (AWS, Azure, Google Cloud) offer elasticity, managed services, and global reach; yet regulatory and client constraints sometimes demand on-premises or sovereign hosting.
In 2026, many EHR deployments follow one of these patterns:
- Pure cloud for startup products or cross-border digital health platforms that need rapid scaling.
- Hybrid where sensitive data stays in regional data centers, while non-identifiable analytics or ancillary services run in the public cloud.
- Private cloud or on-premises environments for government, defence, or highly regulated institutions.
Your architecture should be cloud-ready even if you start on-premises, so that future migration or regional expansion does not require a complete rewrite.
EHR development lifecycle: from concept to go-live
EHR development is not a linear software project; it is a transformation program that touches clinical practice, operations, and compliance. A structured lifecycle helps avoid the common pitfalls.
6.1 Discovery and workflow mapping
The first phase involves deep discovery:
- Mapping current clinical and administrative workflows across departments.
- Understanding pain points, workarounds, and informal communication channels.
- Prioritizing use cases that deliver immediate value while designing with the end-state architecture in mind.
Workshops, shadowing sessions, and process mapping are invaluable. Our aim not to simply digitize legacy paper processes, but to streamline and improve them.
6.2 Requirements, regulation, and data standards
Once workflows are understood, teams can specify:
- Functional requirements for each module.
- Regulatory obligations (HIPAA in the United States, GDPR in Europe, ABDM and Indian EHR standards, and local data-protection laws).
- Data standards and terminologies that will underpin interoperability and analytics.
Capturing these requirements early prevents costly rework when integrating with national exchanges or responding to compliance audits.
6.3 Experience design and prototyping
With requirements defined, cross-functional teams design:
- Personas for different user types from senior consultants and nurses to billing clerks and patients.
- Screen flows for high-frequency tasks such as creating encounters, writing progress notes, or ordering tests.
- Interactive prototypes that clinicians can test and critique before development begins.
This stage eliminates unnecessary clicks, reduces cognitive load, and ensures the system mirrors the way clinicians naturally think and work.
6.4 Incremental development and integration
Rather than aiming for a single large release, teams typically:
- Build modules iteratively, starting with core registration, scheduling, and documentation.
- Integrate with identity services, laboratory systems, imaging archives, and billing engines as modules mature.
- Maintain continuous integration pipelines with automated tests for performance, security, and interoperability.
Close feedback loops with early adopters help refine workflows long before full deployment.
6.5 Testing, validation, and go-live
Testing for an EHR extends far beyond functional checks:
- Clinical safety testing to ensure orders, alerts, and documentation behave correctly in realistic scenarios.
- Performance testing under predicted loads, including traffic from external health exchanges such as TEFCA or ABDM.
- Security assessments such as penetration tests and validation within national digital health sandbox environments where required.
Go-live is best treated as a staged rollout with pilot sites, hypercare support, and rollback strategies - never a single abrupt organization-wide switch.
6.6 Training, change management, and continuous improvement
Successful EHR programs invest in:
- Role-specific training that focuses on real workflows, not merely screen navigation.
- Super-user programs where motivated clinicians become local champions and trainers.
- Continuous feedback cycles that inform backlog refinement and feature evolution.
After implementation, the EHR must be treated as a living product with ongoing enhancements, not a one-time deployment.
Interoperability, national programs, and third-party integrations
By 2026, interoperability is no longer optional. Many countries are building national frameworks that require compliant systems to share data securely and consistently.
7.1 Standards and frameworks to align with
On the standards side, your EHR should support at least:
- HL7 v2 for many existing lab and hospital interfaces.
- FHIR for modern, resource-based exchange across mobile and web applications.
- DICOM for imaging workflows in radiology, cardiology, and related specialties.
On the framework side:
- In the United States, TEFCA has gone live with multiple Qualified Health Information Networks (QHINs), enabling nationwide exchange under unified rules.
- In India, ABDM and the associated EHR standards define participation in a federated, consent-driven health data ecosystem built around ABHA identifiers and strict data governance policies.
Designing with these frameworks from the start prevents costly retrofits when introducing consent workflows, identity mapping, or large-scale exchange capabilities later.
7.2 Key third-party integrations
Most EHR deployments must connect to a broad ecosystem of systems and devices:
- Laboratory information systems for biochemistry, hematology, pathology, and microbiology results.
- Imaging systems and PACS for radiology, cardiology, and other imaging-heavy specialties.
- Pharmacy and medication dispensing systems with formulary validation, e-prescribing, and fulfillment updates.
- Payment gateways and billing platforms for copay collection, installment plans, and insurer submissions.
- Public health and registry systems for immunization, disease surveillance, and mandatory registries such as cancer programs.
Each integration introduces its own standards, security considerations, throttling patterns, and operational expectations. A robust integration layer with monitoring dashboards, retry logic, auditing, and structured error handling is just as critical as the clinical interface itself.
Security, privacy, and compliance for modern EHRs
Healthcare data is among the most sensitive categories of personal information, and regulators are tightening requirements across jurisdictions.
8.1 Core security controls
A credible EHR platform in 2026 must implement layered defenses:
- Strong identity and access management with multi-factor authentication, fine-grained roles, and just-enough privilege.
- Encryption of data in transit and at rest across primary databases, backups, logs, and message queues.
- Comprehensive audit logging that records who accessed records, what actions were taken, and from which device or location.
- Regular patching, vulnerability scans, and secure-coding practices, especially for internet-facing portals and APIs.
8.2 Regulatory frameworks
Depending on where your EHR is deployed, you must align with:
- HIPAA in the United States includes breach notification obligations and business associate agreements.
- GDPR in Europe, covering data-subject rights, lawful bases for processing, and cross-border transfer requirements.
- ABDM Health Data Management Policy and Indian EHR Standards, which define consent, anonymization, and security expectations within the national digital health ecosystem.
For multi-region products, it is often wise to design to the highest applicable standard and configure region-specific variations only where required by law.
8.3 Data governance and lifecycle
Security is only one layer; data governance defines how information is handled over time:
- Retention rules for different types of records and how they are archived or anonymized after their retention period.
- Access policies for research or secondary use, including de-identification and approvals workflows.
- Backup, disaster-recovery, and business-continuity processes to keep life-critical systems resilient to outages, cyberattacks, or infrastructure failures.
Clear governance policies, backed by enforceable technical controls, safeguard both patients and providers while ensuring regulatory alignment.
Cost and timeline expectations in 2026
EHR programs have a reputation for overruns and disappointments, often because stakeholders underestimate the scope of change. While exact figures vary by region and scale, a few patterns hold.
9.1 Cost drivers
Major cost components include:
- Initial product build or licensing: architecture, design, development, configuration, and customizations.
- Integration work with laboratories, imaging systems, billing platforms, national exchanges, and other third-party tools.
- Infrastructure and hosting costs, whether cloud or on-premises, including redundancy, monitoring, and disaster-recovery setups.
- Change management and training, which often require more investment than engineering alone.
- Ongoing maintenance: bug fixes, regulatory updates, performance improvements, and support operations.
Custom solutions typically involve higher initial investment but often deliver greater long-term value, especially when they match organizational workflows closely and eliminate the need for costly workarounds.
9.2 Typical timelines
For a greenfield custom EHR covering registration, scheduling, documentation, ordering, and billing - plus a moderate set of integrations - organizations commonly observe:
- Six to nine months for discovery, workflow mapping, design, and development of an MVP for one or two departments.
- An additional six to twelve months to expand feature depth, finalize integrations, conduct rigorous testing, and deploy across an entire hospital or network.
More complex national integrations, multi-country deployments, or deep specialty requirements can extend timelines further. The most successful programs implement phased rollouts with clear value delivered at each step, rather than deferring all benefits to a distant - big bang - launch.
Choosing the right EHR development partner
Even when you have a strong internal technology team, external partners often play a crucial role in bringing an EHR product to life and ensuring that it remains aligned with evolving standards and regulatory expectations.
When evaluating a technology partner:
Healthcare depth matters more than generic software experience
Look for a track record in healthcare domains such as EHR platforms, interoperability gateways, health information exchanges, or clinical information systems. Prior experience with standards like FHIR, HL7, and DICOM, and familiarity with national frameworks such as TEFCA or ABDM, reduces risk and accelerates delivery.
Evidence of successful implementations
Case studies, production references, and working live systems reveal how the partner handles real-world challenges from clinician adoption and workflow design to complex integrations and edge-case failures. Speak with customers who have gone through both go-live and at least one major upgrade cycle.
Capability to provide long-term support
An EHR is a long-term program, not a short-term project. Your partner should demonstrate strength in support operations, incident management, monitoring, capacity planning, and release management. They should also maintain an evolving roadmap that stays ahead of regulatory and technological changes.
Alignment with your product vision
The best partner behaves like an extension of your clinical and product teams. They challenge assumptions, bring learnings from other markets, prioritize safety and usability, and focus on real patient and clinician outcomes not just closing tickets or meeting minimum specifications.
Conclusion: building EHRs that clinicians and patients actually trust
By 2026, the question is no longer whether to digitize health records; that debate is settled. The real question is whether your EHR becomes just another system clinicians tolerate, or a platform that genuinely improves care, reduces administrative burden, and positions your organization for the next decade of digital health innovation.
That outcome depends on a few foundational choices:
- Treating the EHR as a longitudinal, patient-centric platform rather than a static digital chart.
- Designing around real workflows and clinician experience instead of focusing solely on abstract data models.
- Committing to interoperability, national frameworks, and consent-driven data exchange from the very beginning.
- Embedding strong security, governance, and auditability so that stakeholders can trust the system with their most sensitive information.
- Choosing partners and architectures that support continuous evolution rather than locking the organization into rigid patterns.
If you approach EHR software development with this mindset in 2026, the result becomes more than a compliance requirement; it evolves into a strategic asset that shapes how your organization delivers care, collaborates across the ecosystem, and builds new services on top of a resilient digital foundation.
Frequently Asked Questions
What are the main benefits of a modern EHR system?
In practice, a system brings together clinical, operational, and financial information into a single, consistent view of the patient. This improves clinical decision-making, reduces duplicate tests, enables safer prescribing, and supports coordinated care across teams and locations. It also streamlines billing and reporting, supports participation in national digital health programs, and creates a high-quality data asset for quality improvement and population-health initiatives.
Notably, a system brings together clinical, operational, and financial information into a single, consistent view of the patient. This improves clinical decision-making, reduces duplicate tests, enables safer prescribing, and supports coordinated care across teams and locations. It also streamlines billing and reporting, supports participation in national digital health programs, and creates a high-quality data asset for quality improvement and population-health initiatives.How do I decide between custom EHR development and an off-the-shelf product?
If your organization has relatively standard workflows, a limited appetite for product ownership, and an urgent need for basic digitization and compliance, a proven off-the-shelf product may be the most pragmatic choice. If you operate in specialized domains, expect to differentiate on workflow, patient experience, or analytics, or must integrate deeply with national frameworks and proprietary systems; custom or hybrid approaches usually deliver a better fit and long-term value.
If your organization has relatively standard workflows, a limited appetite for product ownership, and an urgent need for basic digitization and compliance, a proven off-the-shelf product may be the most pragmatic choice. If you operate in specialized domains, expect to differentiate on workflow, patient experience, or analytics, or must integrate deeply with national frameworks and proprietary systems; custom or hybrid approaches usually deliver a better fit and long-term value.How can I ensure the security of patient data in an EHR system?
Security starts with strong identity and access management, encryption of data at rest and in transit, and rigorous audit trails. On top of this, you should align with applicable regulations such as HIPAA, GDPR, or ABDM Health Data Management Policy; perform regular security assessments and penetration tests; and maintain clear governance for data retention, backups, and incident response.
Security starts with strong identity and access management, encryption of data at rest and in transit, and rigorous audit trails. On top of this, you should align with applicable regulations such as HIPAA, GDPR, or ABDM Health Data Management Policy; perform regular security assessments and penetration tests; and maintain clear governance for data retention, backups, and incident response.What are the key interoperability requirements for 2026-ready EHRs?
At a minimum, your system should support HL7 v2 for legacy integrations, FHIR for modern, resource-based APIs, and DICOM for imaging, with profiles that match national or regional implementation guides. In markets like the United States and India, participation in frameworks such as TEFCA and ABDM may be necessary to enable cross-network exchange and to access national services such as identifiers and registries.
At a minimum, your system should support HL7 v2 for legacy integrations, FHIR for modern, resource-based APIs, and DICOM for imaging, with profiles that match national or regional implementation guides. In markets like the United States and India, participation in frameworks such as TEFCA and ABDM may be necessary to enable cross-network exchange and to access national services such as identifiers and registries.How do I measure the return on investment for an EHR implementation?
Return on investment is multi-dimensional. Financial metrics include reductions in paper handling, transcription, and manual billing effort, as well as improved claims acceptance and reduced denials. Operational metrics include appointment throughput, reduced waiting times, and fewer missed follow-ups. Clinical metrics include guideline adherence, adverse event rates, and patient outcomes. The most effective programs define these indicators up front and monitor them over time using the reporting and analytics capabilities of the EHR and associated data platforms.
Return on investment is multi-dimensional. Financial metrics include reductions in paper handling, transcription, and manual billing effort, as well as improved claims acceptance and reduced denials. Operational metrics include appointment throughput, reduced waiting times, and fewer missed follow-ups. Clinical metrics include guideline adherence, adverse event rates, and patient outcomes.
Struggling with healthcare data exchange? Our Healthcare Interoperability Solutions practice helps organizations connect clinical systems at scale. We also offer specialized Healthcare Software Product Development services. Talk to our team to get started.