Over 60% of US hospitals still run at least one critical application on legacy software that lacks native FHIR support. Yet with CMS-0057-F mandating four FHIR APIs by January 2027 and 98% of hospitals now expected to expose FHIR R4 endpoints, the gap between regulatory reality and legacy infrastructure has never been wider. The FHIR Facade pattern bridges that gap — without ripping out your existing systems.
This guide covers everything: architecture deep-dives, implementation approaches, when to use a facade versus a repository, vendor comparisons, real code examples, and the regulatory deadlines driving adoption. Whether you are a CTO evaluating modernization strategies or an engineer tasked with building FHIR compliance, this is the most comprehensive FHIR Facade resource available.
Related Reading
For more insights, explore our guides on SMART On FHIR Architecture Complete Visual Guide Developers and FHIR in Modern Healthcare.
You may also find value in EHR Software Development Guide and Building a Healthtech App.
What Is a FHIR Facade?
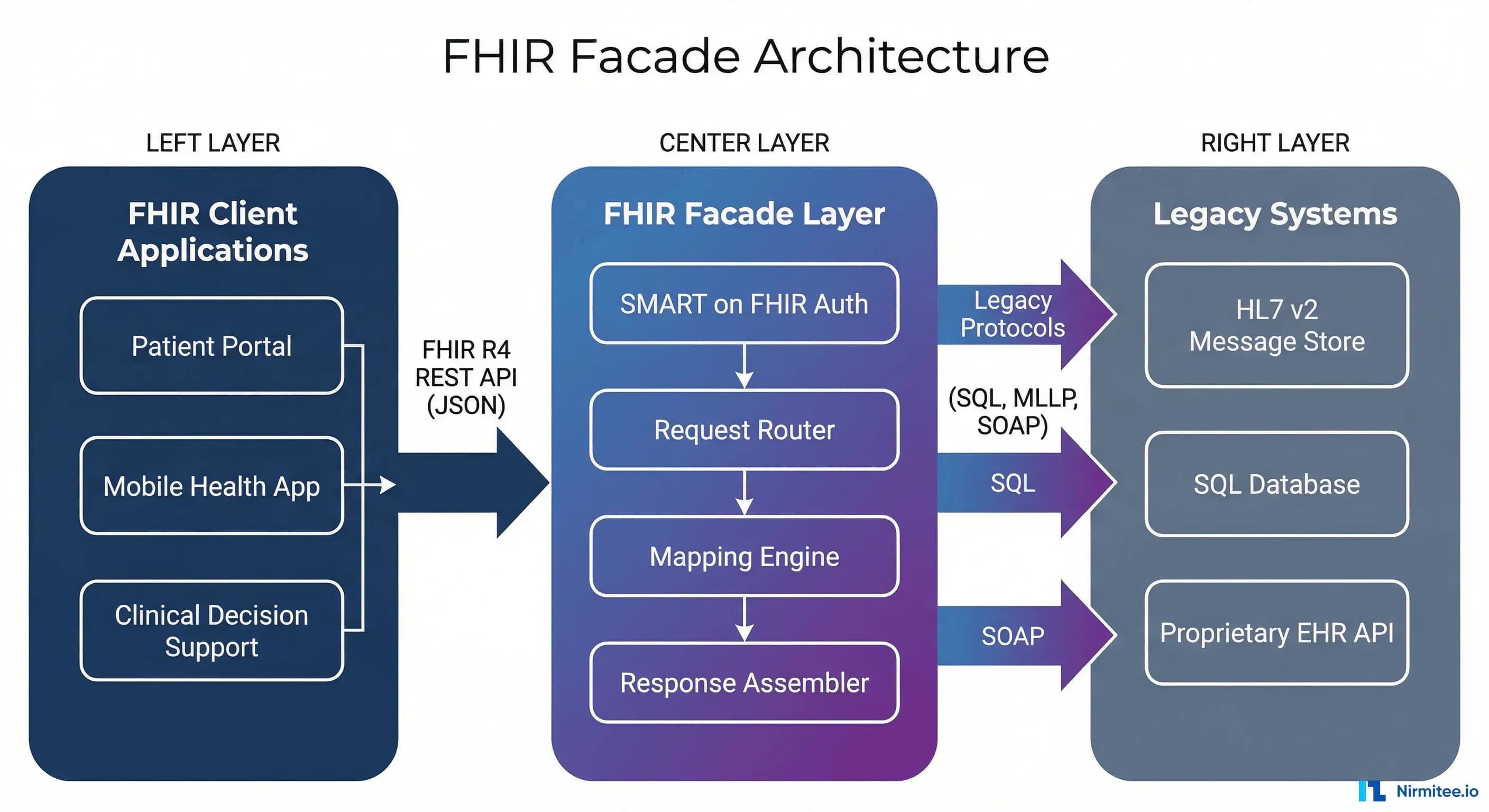
A FHIR Facade is an architectural layer that exposes a fully compliant FHIR R4 API on top of an existing non-FHIR system — whether that is a legacy EHR, an HL7 v2 message store, a relational database, or a proprietary clinical data warehouse. Data remains in its original source system. When a FHIR client sends a request, the facade translates it on the fly into whatever query language the legacy system understands, maps the response back to FHIR resources, and returns standards-compliant JSON or XML.
Think of it as a real-time translator sitting between the modern FHIR world and your existing infrastructure. No data migration. No warehouse duplication. No clinical workflow disruption.
The Three Core Functions
Every FHIR Facade performs three operations:
- Request interception and routing — The facade receives incoming FHIR REST calls (GET /Patient, POST /Observation, etc.) and routes them to the appropriate legacy system adapter.
- Data translation and mapping — This is the heart of the facade. Legacy data formats (HL7 v2 segments, flat database rows, proprietary XML) are mapped to FHIR resource structures. A patient name stored as
PID-5in HL7 v2 becomes aPatient.nameHumanName datatype in FHIR R4. - Response assembly — Individual mapped elements are assembled into valid FHIR resources, wrapped in Bundles when needed, and returned with proper HTTP status codes, OperationOutcome resources for errors, and FHIR-compliant pagination.
How a FHIR Facade Works: Request Flow
Understanding the request lifecycle is critical for implementation planning. Here is what happens when a consumer application queries GET /fhir/Patient?family=Smith against a facade:
- FHIR request arrives — The client sends a standard FHIR REST request to the facade endpoint.
- Authentication and authorization — The facade validates the request using SMART on FHIR scopes (e.g.,
patient/Patient.read). This is non-negotiable for ONC certification. - Search parameter parsing — FHIR search parameters (
family=Smith) are parsed and translated to legacy query equivalents (e.g., SQLWHERE last_name = 'Smith'or HL7 v2 QBP message). - Legacy system query — The facade issues the translated query to the source system.
- Response mapping — Legacy results are mapped to FHIR resources using the facade's mapping engine.
- FHIR Bundle assembly — Results are wrapped in a FHIR searchset Bundle with proper pagination links, total count, and self link.
- Response delivery — The FHIR-compliant response is returned to the client with appropriate HTTP headers.
FHIR Facade Architecture Deep Dive
A production-grade FHIR Facade is not a simple API wrapper. It contains multiple internal components that work together to deliver reliable, performant, and standards-compliant interoperability.
Component Breakdown
| Component | Purpose | Key Considerations |
|---|---|---|
| API Gateway / FHIR Server Shell | Handles HTTP routing, content negotiation (JSON/XML), FHIR version detection, and capability statement generation | Must support _format, _pretty, _summary parameters per FHIR spec |
| SMART on FHIR Auth Layer | OAuth 2.0 authorization, token validation, scope enforcement | Required for ONC HTI-1 certification. Must support standalone launch, EHR launch, and backend services |
| Resource Router | Maps incoming FHIR resource type + operation to the correct legacy system adapter | Patient queries might go to the MPI, Observations to the lab system, Medications to pharmacy |
| Mapping Engine | Translates between FHIR resource structures and legacy data models | The hardest part. Mapping complexity grows with each resource type and search parameter |
| Legacy System Adapters | Database connectors, HL7 v2 MLLP clients, SOAP clients, REST clients for each source system | Each adapter handles connection pooling, retries, and legacy-specific error handling |
| Audit Logger | HIPAA-compliant access logging, provenance tracking | Must log who accessed what data, when, and under what authorization context |
Implementation Example: Python FastAPI Facade
Here is a minimal but functional FHIR Facade built with Python FastAPI that wraps a legacy PostgreSQL patient database:
from fastapi import FastAPI, HTTPException, Query
from typing import Optional
import asyncpg
import json
from datetime import date
app = FastAPI(title="FHIR Facade", version="R4")
# Legacy database connection
async def get_db():
return await asyncpg.connect(
host="legacy-db", database="hospital_ehr",
user="fhir_readonly", password="***"
)
def map_patient_to_fhir(row: dict) -> dict:
"""Map legacy patient table row to FHIR Patient resource."""
return {
"resourceType": "Patient",
"id": str(row["patient_id"]),
"meta": {"lastUpdated": row["modified_at"].isoformat()},
"identifier": [{
"system": "http://hospital.example.org/mrn",
"value": row["mrn"]
}],
"name": [{
"use": "official",
"family": row["last_name"],
"given": [row["first_name"]]
}],
"gender": row["sex"].lower(), # M/F -> male/female
"birthDate": row["dob"].isoformat()
}
@app.get("/fhir/Patient")
async def search_patient(
family: Optional[str] = Query(None),
given: Optional[str] = Query(None),
_id: Optional[str] = Query(None, alias="_id")
):
db = await get_db()
# Translate FHIR search params to SQL
conditions, params = [], []
if family:
conditions.append(f"last_name ILIKE ${len(params)+1}")
params.append(f"%{family}%")
if given:
conditions.append(f"first_name ILIKE ${len(params)+1}")
params.append(f"%{given}%")
if _id:
conditions.append(f"patient_id = ${len(params)+1}")
params.append(int(_id))
where = " AND ".join(conditions) if conditions else "1=1"
rows = await db.fetch(f"SELECT * FROM patients WHERE {where} LIMIT 50", *params)
await db.close()
entries = [{
"fullUrl": f"Patient/{row['patient_id']}",
"resource": map_patient_to_fhir(dict(row))
} for row in rows]
return {
"resourceType": "Bundle",
"type": "searchset",
"total": len(entries),
"entry": entries
}
@app.get("/fhir/metadata")
async def capability_statement():
return {
"resourceType": "CapabilityStatement",
"status": "active",
"kind": "instance",
"fhirVersion": "4.0.1",
"format": ["json"],
"rest": [{
"mode": "server",
"resource": [{
"type": "Patient",
"interaction": [{"code": "read"}, {"code": "search-type"}],
"searchParam": [
{"name": "family", "type": "string"},
{"name": "given", "type": "string"},
{"name": "_id", "type": "token"}
]
}]
}]
}This 80-line example demonstrates the core facade pattern: receive FHIR requests, translate search parameters to SQL, map database rows to FHIR resources, and return a standards-compliant Bundle. A production implementation would add connection pooling, error handling, pagination, and SMART on FHIR authentication.
FHIR Facade vs. Repository vs. Hybrid: How to Choose
The FHIR Facade is one of three architectural models. Choosing the wrong one wastes months of engineering effort. Here is a definitive comparison.
| Dimension | FHIR Facade | FHIR Repository | Hybrid (Facade + Cache) |
|---|---|---|---|
| Data storage | Data stays in source system | Data copied to FHIR-native store | Hot data cached in FHIR store, rest queried live |
| Data freshness | Always real-time | Depends on sync frequency (minutes to hours) | Cached data may be stale, live queries are real-time |
| Query performance | Bounded by legacy system speed | Optimized for FHIR search | Fast for cached resources, legacy-speed for others |
| FHIR search coverage | Limited to what you map | Full FHIR search spec support | Full for cached, limited for live |
| Write support | Complex — must reverse-map to legacy | Native FHIR writes | Writes go to repository, synced back to legacy |
| Implementation effort | Moderate (per resource type) | High upfront, low per-resource | Highest — maintain both paths |
| Data duplication | None | Full duplication | Partial duplication |
| Compliance risk | Low — single source of truth | Higher — must keep stores in sync | Medium — sync logic adds complexity |
| Best for | Read-heavy, real-time access, regulatory compliance | Analytics, research, bulk data export | Mixed workloads, gradual migration |
| Time to first API | Weeks | Months | Months |
The Decision Framework
Choose a FHIR Facade when:
- Your primary need is read access to existing data via FHIR APIs
- Data freshness is critical — you need real-time results, not stale copies
- You have regulatory deadlines (CMS-0057-F, ONC HTI-1) and need compliance fast
- Budget is constrained — you cannot afford a multi-month data migration project
- The legacy system is staying — there is no plan to replace it
Choose a FHIR Repository when:
- You need full FHIR search capabilities including chained searches,
_include,_revinclude - Analytics and bulk data export ($export) are core use cases
- You are building a new system or doing a greenfield implementation
- Write operations (creating/updating resources) are a primary workflow
Choose a Hybrid when:
- You need the real-time accuracy of a facade for clinical data but fast search for analytics
- You are on a multi-year migration path from legacy to FHIR-native
- Different resource types have different freshness requirements
Legacy System Integration: What Can Be Wrapped
A FHIR Facade can wrap virtually any data source. Here are the most common legacy system types and the complexity involved in wrapping each.
| Legacy System Type | Translation Complexity | Common Tools | Key Challenge |
|---|---|---|---|
| HL7 v2 Message Store | Medium | HAPI v2, Mirth Connect, Rhapsody | v2 segments do not map 1:1 to FHIR resources. OBX alone can become Observation, DiagnosticReport, or DocumentReference depending on context. |
| Relational Database (SQL) | Low-Medium | Custom code, ORM mappers | Schema-specific. Every hospital's patient table is different. Mapping must be built per deployment. |
| C-CDA Documents | Medium-High | HL7 CCDA-on-FHIR IG, XSLT | C-CDA sections are document-oriented; FHIR is resource-oriented. Requires section-level parsing and resource extraction. |
| X12 EDI (837/835/278) | High | Edifecs, custom parsers | X12 is financial transaction-oriented with complex loop structures. Mapping to clinical FHIR resources requires domain expertise. |
| Proprietary EHR APIs | Varies | Custom adapters | Vendor-specific data models, auth mechanisms, and rate limits. Epic, Cerner, and MEDITECH each require unique adapters. |
| Flat Files (CSV/HL7 v2 batch) | Low | Python/Node.js scripts | Batch-oriented. The facade must handle incremental loads and maintain state for change detection. |
Regulatory Drivers: Why Organizations Need FHIR Facades Now
The urgency behind FHIR Facade adoption is not theoretical — it is driven by hard regulatory deadlines with financial penalties for non-compliance.
The Regulatory Timeline
According to the 2025 State of FHIR Survey by HL7 and Firely, 73% of country-level regulations now mandate or recommend FHIR (up from 56% in 2023). In the US specifically:
- ONC HTI-1 Final Rule (January 2025) — All certified health IT must support USCDI v3 via FHIR R4 APIs. This means every EHR vendor must expose patient data through FHIR. Organizations using legacy systems without native FHIR need a facade to comply.
- CMS-0057-F Prior Authorization API (January 2026) — Payers must respond to prior authorization requests within 7 calendar days (standard) or 72 hours (urgent) via FHIR APIs. Payers running legacy claims adjudication systems need facades to expose this data.
- CMS-0057-F Full API Mandate (January 2027) — Four FHIR APIs become mandatory for payers: Patient Access API, Provider Access API, Payer-to-Payer API, and Prior Authorization Support API. This is the biggest FHIR compliance deadline in US healthcare history.
For payer organizations, the math is simple: a FHIR Facade that wraps your existing claims platform can be built in weeks to months. A full FHIR repository migration takes 12-24 months. With January 2027 approaching, the facade is often the only viable path to compliance.
FHIR Adoption Statistics
The data confirms that FHIR is no longer optional:
- 98% of US hospitals now use FHIR-based interoperability (mandated by the 21st Century Cures Act)
- 71% of surveyed countries report FHIR is actively used, up from 66% in 2024 (HL7/Firely 2025 Survey)
- 76% of FHIR adopters cite lack of FHIR expertise as the top implementation barrier
- 73% of healthcare providers still rely on legacy software solutions
- Up to 75-80% of healthcare IT budgets are consumed by maintaining legacy systems
These numbers explain why FHIR Facades are seeing explosive adoption: organizations need FHIR compliance but cannot replace their core systems fast enough.
Implementation Approaches: Build vs. Buy
There are four main paths to implementing a FHIR Facade, each with different trade-offs.
| Approach | Technology | Best For | Effort | Cost Model |
|---|---|---|---|---|
| Open-Source Framework | HAPI FHIR Plain Server (Java), Aidbox (Docker), python-fhir | Engineering-heavy orgs with FHIR expertise | Medium-High | Free license, engineering cost |
| Commercial FHIR Platform | Firely Server (.NET), Smile CDR (Java), InterSystems IRIS | Orgs needing vendor support + SLA | Low-Medium | License + implementation |
| Cloud-Native Service | Azure Health Data Services, AWS HealthLake, Google Cloud Healthcare API | Cloud-first orgs, already on the platform | Low | Pay-per-use, scaling costs |
| Custom Build | Python (FastAPI/Django), Node.js (Express), Go | Specific legacy systems, unique requirements | High | Full engineering ownership |
How to Choose
Start with HAPI FHIR Plain Server if you have Java developers and want maximum control. HAPI is the reference implementation — battle-tested in thousands of deployments. The Plain Server mode is specifically designed for facades: you implement resource provider interfaces and HAPI handles everything else (parsing, serialization, search parameter handling, capability statement).
Use a commercial platform (Firely, Smile CDR) if you need certification support, vendor SLAs, and faster time-to-market. Commercial platforms include pre-built mapping tools, SMART on FHIR servers, and compliance testing suites.
Go cloud-native if you are already on Azure/AWS/GCP and your data is accessible from the cloud. Azure Health Data Services includes a built-in FHIR server with conversion pipelines for HL7 v2 and C-CDA.
Build custom only when your legacy system is so unique that no framework supports it, or when you need a lightweight facade for a narrow use case (e.g., wrapping a single legacy API for a specific AI agent integration).
Incremental Migration: The Phased Approach
One of the most powerful aspects of the FHIR Facade pattern is that it enables incremental modernization. You do not need to wrap every resource type on day one.
Recommended Phasing
- Phase 1 (Weeks 1-4): Patient Demographics — Start with the Patient resource. This is the foundation of every FHIR interaction, has relatively simple mapping, and immediately enables patient-facing apps.
- Phase 2 (Weeks 5-8): Clinical Core — Add Condition, AllergyIntolerance, and Medication resources. These cover the US Core Data for Interoperability (USCDI) required elements.
- Phase 3 (Weeks 9-12): Diagnostics — Add Observation (lab results, vitals), DiagnosticReport, and clinical data for dashboards. These resources have higher mapping complexity due to varied coding systems.
- Phase 4 (Weeks 13-16): Documents and Operations — Add DocumentReference (for C-CDA/PDF access), Encounter, and Procedure. Implement bulk data export ($export) if required.
- Phase 5 (Ongoing): Advanced Features — Add write operations, subscriptions, and remaining USCDI resources as needed. At this point, evaluate whether to begin migrating high-query resources to a hybrid model.
Common Pitfalls and Anti-Patterns
After working with healthcare organizations across the US and India on FHIR implementations, these are the mistakes we see most often:
1. Mapping Everything at Once
Trying to map all 150+ FHIR resource types before launching. Start with the 8-10 resources that cover your use case (US Core profiles cover most regulatory requirements with ~20 resources).
2. Ignoring Search Parameter Complexity
Each FHIR search parameter you support requires a translation rule. Supporting Patient?name=Smith is simple. Supporting Observation?code=http://loinc.org|85354-9&date=gt2024-01-01&_include=Observation:patient is an order of magnitude more complex. Plan your search parameter support deliberately.
3. Skipping the Capability Statement
The /metadata endpoint is not optional. It is how FHIR clients discover what your server supports. An inaccurate capability statement causes cascading failures in client applications and will fail ONC certification testing.
4. No Caching Strategy
Pure facades query the legacy system on every request. For high-traffic resources like Patient, this can overwhelm the legacy database. Implement HTTP caching headers (ETag, Last-Modified) and consider a thin cache layer for frequently accessed resources.
5. Underestimating Terminology Mapping
Legacy systems often use local codes ("Lab code 4532") instead of standard terminologies (LOINC, SNOMED CT, ICD-10). Your facade needs a terminology mapping layer or crosswalk tables to produce standards-compliant resources. Without this, your FHIR API returns syntactically valid but semantically useless data.
6. Treating Authorization as an Afterthought
SMART on FHIR authorization is required for ONC certification and is expected by every modern FHIR client. Bolting it on after building the facade creates security gaps. Design your auth layer from day one.
Performance Considerations
A FHIR Facade's performance is bounded by the slowest legacy system it wraps. Key optimization strategies:
- Connection pooling — Maintain persistent connections to legacy databases instead of opening/closing per request
- Parallel queries — When a FHIR Bundle requires data from multiple legacy systems, query them concurrently
- Pagination enforcement — Never return unbounded result sets. Enforce
_countlimits (default: 20-50 resources per page) - Response caching — Cache frequently accessed, slowly changing resources (e.g., Patient demographics) with short TTLs (5-15 minutes)
- Lazy loading — Only resolve
_includeand_revincludereferences when explicitly requested
Target response times: under 500ms for single resource reads, under 2 seconds for search queries returning up to 50 results. If your legacy system cannot meet these targets, consider the hybrid approach with a FHIR cache for hot data.
FHIR R4 to R6: Future-Proofing Your Facade
FHIR R4 is the current standard, but FHIR R6 is expected in late 2026 with most resources reaching normative status. How does this affect your facade strategy?
The good news: FHIR maintains strong backward compatibility. A well-designed facade with a clean mapping layer can support multiple FHIR versions simultaneously by implementing version-specific mappers behind the same legacy system adapter. The facade pattern actually makes version migration easier than a repository migration, because you are only changing the output mapping — not migrating stored data.
Design recommendation: Keep your mapping logic in a separate module from your legacy system adapter. When R6 arrives, you add new mappers without touching your database integration code.
Frequently Asked Questions
What is the difference between a FHIR Facade and a FHIR server?
A FHIR server (repository) stores data natively in FHIR format. A FHIR Facade does not store data — it translates data from existing non-FHIR systems into FHIR format on-the-fly. Both expose FHIR-compliant APIs, but the data storage model is fundamentally different.
How long does it take to implement a FHIR Facade?
For a single resource type (e.g., Patient) with basic search parameters: 2-4 weeks. For a comprehensive facade covering US Core profiles (~20 resources): 3-6 months. For a full implementation with SMART on FHIR, bulk data, and write operations: 6-12 months. These timelines assume a team with FHIR experience; add 30-50% for teams new to FHIR.
Can a FHIR Facade support write operations?
Yes, but with significant complexity. Write operations require reverse-mapping from FHIR resources back to legacy data formats, handling legacy system constraints (required fields, validation rules, referential integrity), and managing error translation. Most organizations start with read-only facades and add write support incrementally.
Is a FHIR Facade sufficient for ONC certification?
A FHIR Facade can pass ONC certification (specifically the (g)(10) Standardized API criterion) if it implements: FHIR R4, US Core profiles, SMART on FHIR authorization, bulk data export ($export), and the required USCDI data elements. The certification tests do not distinguish between facade and repository implementations — they test API compliance.
How does a FHIR Facade handle data from multiple legacy systems?
Through the Resource Router component. Different FHIR resource types can be routed to different legacy systems. Patient data might come from the MPI, lab results from the LIS, medications from the pharmacy system, and documents from the ECM. The facade assembles a unified FHIR API from multiple disparate sources — this is one of its greatest strengths.
What about FHIR Facades for ABDM compliance in India?
India's Ayushman Bharat Digital Mission (ABDM) mandates FHIR R4 bundles for health information exchange. Healthcare facilities running legacy HIS/HMIS systems use FHIR Facades to generate compliant FHIR Bundles for M1 (registration), M2 (health records), and M3 (consent-based data sharing) milestones without replacing their core systems. The facade pattern is particularly relevant for the thousands of small and mid-size hospitals in India running proprietary software.
Conclusion: The Pragmatic Path to FHIR Compliance
The FHIR Facade is not a temporary workaround — it is a proven architectural pattern used by organizations from 50-bed hospitals to national payer networks. It delivers FHIR compliance without the risk, cost, and disruption of a full system replacement.
With CMS-0057-F deadlines approaching, the 76% of organizations citing FHIR expertise gaps, and 73% still running legacy systems, the facade pattern will only grow in importance. Start with Patient, prove the pattern works, and expand from there.
At Nirmitee.io, we build FHIR Facades for healthcare organizations in the US and India — from EHR-level implementations to payer API platforms. If you need help navigating your FHIR compliance journey, let's talk.