Every hospital in India has equipment that nobody can find. Not because it was stolen, but because nobody tagged it, nobody tracked it, and nobody knows whether the infusion pump is in Ward 3B, the store room, or being repaired in the biomedical engineering workshop. A Nursing Times/GS1 survey of 1,000 nurses found that one in three nurses spends over an hour per shift searching for equipment. Sixteen percent give up searching entirely and go without.
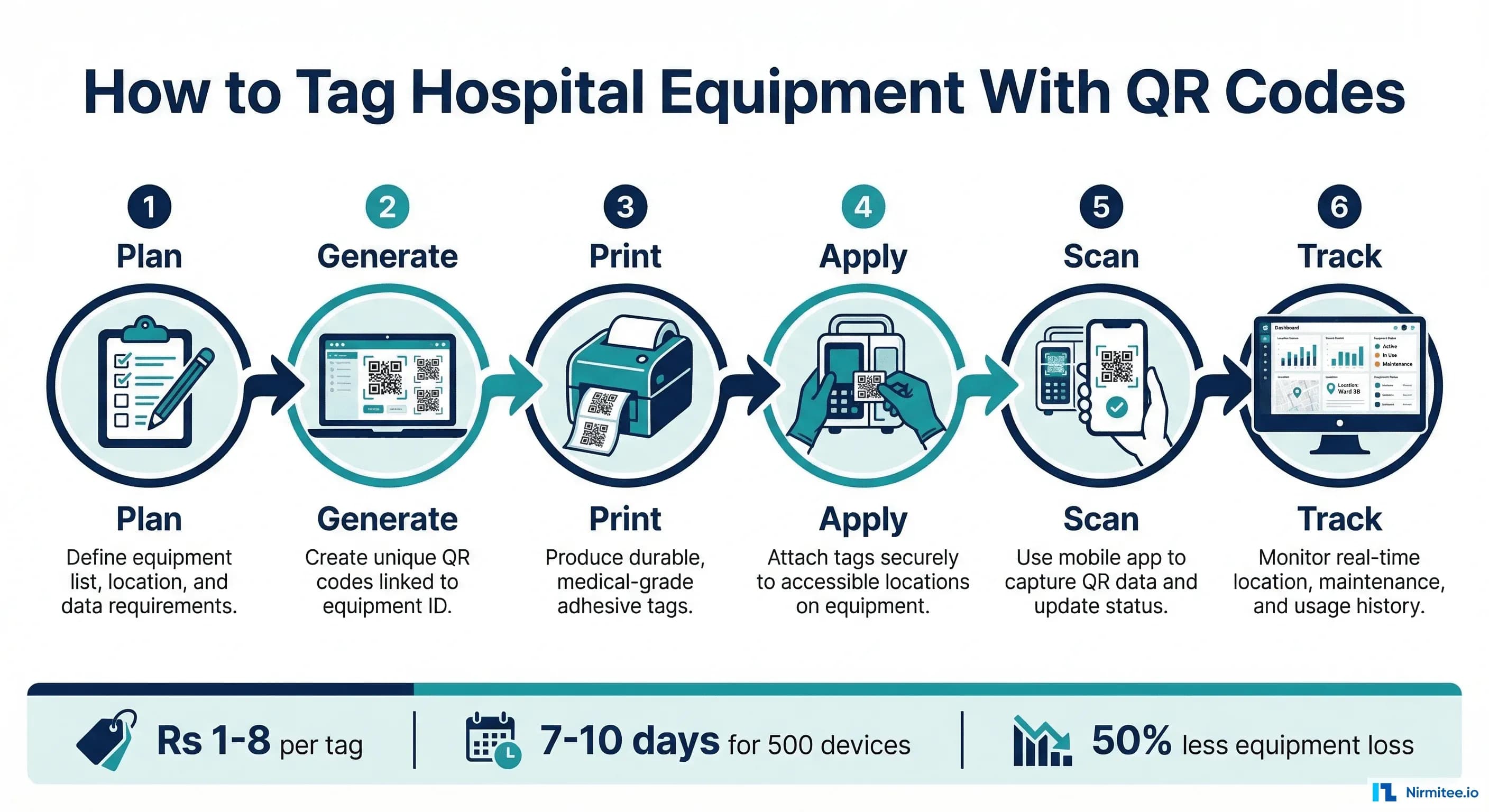
QR code tagging solves this for Rs 1-8 per device. No expensive RFID infrastructure, no BLE gateways, no annual tag battery replacements. A smartphone camera, a sheet of printed labels, and a systematic approach to labeling. That is all it takes to transform a hospital's equipment management from chaos to accountability.
This guide is the step-by-step implementation manual that nobody else has written. Not a high-level overview. Not a vendor pitch. An actual procedure, with the asset numbering convention, the label material specifications, the placement rules, the data structure, and the department-by-department rollout plan that a biomedical engineer can follow starting Monday morning.
Why QR Codes Beat Every Other Tagging Option for Most Indian Hospitals
Before we get into the how, let us settle the technology question definitively. Indian hospitals have four tagging options, and for the vast majority, QR codes are the right starting point.
QR codes cost Rs 1-8 per tag. Passive RFID costs Rs 25-65. Active RFID/BLE costs Rs 1,600-4,000. When you have 500+ devices to tag, the difference between Rs 4,000 (QR for everything) and Rs 8,00,000+ (BLE for everything) is the difference between a project that gets approved and one that sits in next year's budget.
QR codes hold up to 2,500 characters of data. Barcodes hold 20. This means a QR code can encode not just an asset ID, but a URL that links to the complete equipment profile, including maintenance history, calibration records, and real-time status.
Every smartphone manufactured in the last five years can scan QR codes natively. No special hardware. No app installation on most devices. Your staff already know how to scan QR codes because they have used them for UPI payments.
The limitation is real-time tracking: QR codes tell you where equipment was at the last scan, not where it is right now. For hospitals that need live location tracking of high-value mobile equipment, the answer is not "use RFID instead of QR" but "use QR for everything and add BLE to the 50-100 most critical mobile devices." That hybrid approach is covered in our equipment tracking software features guide.
Step 1: Design Your Asset Numbering Convention
Before you print a single label, you need a systematic numbering convention that every department in the hospital will use consistently. This is where most tagging projects fail: they start printing labels with ad-hoc numbers and end up with duplicates, inconsistencies, and a database that makes no sense six months later.
The Recommended Format: DEPT-FLOOR-TYPE-SERIAL
Each asset ID has four components separated by hyphens:
Format: DEPT-FLOOR-TYPE-SERIAL
DEPT (Department Code - 2-4 characters):
ICU = Intensive Care Unit
OT = Operation Theatre
RAD = Radiology
LAB = Laboratory
ER = Emergency Room
WARD = General Ward
NICU = Neonatal ICU
CCU = Cardiac Care Unit
CSSD = Central Sterile Supply Department
PHARM = Pharmacy
ADMIN = Administration
FLOOR (Location Code - 2-3 characters):
GF = Ground Floor
1F = First Floor
2F = Second Floor
B1 = Basement Level 1
AN = Annexe Building
TYPE (Equipment Type Code - 2-4 characters):
VENT = Ventilator MON = Patient Monitor
DEF = Defibrillator INF = Infusion Pump
MRI = MRI Scanner CT = CT Scanner
XRAY = X-Ray Machine USG = Ultrasound
ECG = ECG Machine ABG = Blood Gas Analyzer
AUTO = Autoclave SURG = Surgical Light
BED = Hospital Bed WCH = Wheelchair
SUC = Suction Machine NEB = Nebulizer
SYR = Syringe Pump CENT = Centrifuge
MICR = Microscope SPEC = Spectrophotometer
SERIAL (Sequential Number - 3 digits):
001 through 999
Examples:
ICU-3F-VENT-007 = ICU, 3rd Floor, Ventilator #7
RAD-2F-MRI-001 = Radiology, 2nd Floor, MRI Scanner #1
OT-1F-DEF-003 = Operation Theatre, 1st Floor, Defibrillator #3
LAB-GF-CENT-012 = Laboratory, Ground Floor, Centrifuge #12
ER-GF-MON-015 = Emergency, Ground Floor, Monitor #15Rules for the numbering convention:
- The asset ID is permanent. If a ventilator moves from ICU to WARD, the ID stays ICU-3F-VENT-007. The current location is tracked in the system, not in the ID.
- Do not reuse IDs. If ICU-3F-VENT-007 is condemned, that number is retired. The replacement gets ICU-3F-VENT-008.
- For multi-site hospital groups, add a site prefix: MUM-ICU-3F-VENT-007 (Mumbai), PUN-ICU-2F-VENT-003 (Pune).
- Print the asset ID in human-readable text alongside the QR code. When the QR code is damaged or the scanner is unavailable, staff can enter the ID manually.
Step 2: Choose the Right Label Material
This is where Indian hospital environments demand specific attention. Humidity in coastal cities, autoclave sterilization in CSSDs, chemical disinfectants in ICUs, and rough handling in emergency departments all destroy cheap labels within weeks.
Paper Labels (Rs 0.50-1 per label)
Use only for administrative equipment: computers, printers, office furniture. Paper labels in clinical environments will degrade within 3-6 months from cleaning chemicals, humidity, and handling. Do not use paper labels on any medical device.
Polyester/Synthetic Labels (Rs 2-5 per label) — Recommended for Most Equipment
Water-resistant, chemical-resistant (standard hospital disinfectants), UV-resistant, and durable for 2-5 years. These are the workhorse labels for clinical equipment. Available from medical label suppliers in India in pre-cut sheets compatible with standard laser printers. For thermal transfer printers, polyester ribbon labels offer even better durability.
Metalphoto Anodized Aluminum Tags (Rs 15-40 per tag)
For equipment that undergoes autoclave sterilization (surgical instruments, CSSD trays, reusable containers). These tags withstand multiple sterilization cycles at 134 degrees Celsius, meet FDA ANSI/AAMI ST79 standards, do not harbor bacteria, and remain legible after hundreds of high-heat wash cycles. Essential for surgical instrument tracking.
Ceramic-Coated Metal Tags (Rs 50-100 per tag)
For permanent installation on high-value imaging equipment (MRI, CT, linear accelerators) where the tag needs to last the entire 10-20 year equipment lifespan. Resistant to all chemicals, extreme temperatures, and physical abrasion. Overkill for general equipment but appropriate for assets worth Rs 1 crore or more.
Label Printing Setup
For a hospital-wide tagging project, you need:
- QR code generator software: Free options include qr-code-generator.com (batch generation) or open-source libraries like Python's
qrcodemodule for programmatic generation - Label printer: A thermal transfer printer (Brother, Zebra, TSC) costs Rs 15,000-50,000 and prints polyester labels directly. Alternatively, use a standard laser printer with pre-cut polyester label sheets
- Label design: Each label should include the QR code (minimum 25mm x 25mm for reliable scanning), the human-readable asset ID below it, and optionally the equipment name and department
# Python script to generate QR codes in batch
import qrcode
import csv
# Read equipment list from CSV
with open('equipment_list.csv', 'r') as f:
reader = csv.DictReader(f)
for row in reader:
asset_id = row['asset_id']
# URL that links to equipment profile in your tracking system
url = f"https://assets.yourhospital.in/v/{asset_id}"
qr = qrcode.QRCode(version=1, box_size=10, border=4)
qr.add_data(url)
qr.make(fit=True)
img = qr.make_image(fill_color="black", back_color="white")
img.save(f"labels/{asset_id}.png")
print(f"Generated: {asset_id}")Step 3: Conduct Physical Verification and Inventory
This is the most labor-intensive step and cannot be skipped. Every device must be physically located, verified, and recorded before tagging. This is also a NABH requirement: physical verification of assets must be documented.
The Verification Process
- Form a tagging team: 2-3 biomedical engineers or trained technicians. Include one person from each department to identify equipment and confirm its status.
- Create a master spreadsheet with columns: Asset ID, Equipment Name, Manufacturer, Model, Serial Number, Department, Room Number, Condition (Functional/Needs Repair/Non-Functional), Risk Class, Purchase Date, Purchase Cost.
- Go department by department. Do not try to tag the entire hospital in one pass. Start with one department, complete it, learn from the process, then move to the next.
- Record every device. Every medical device, regardless of size. Infusion pumps, patient monitors, pulse oximeters, nebulizers, suction machines, hospital beds, wheelchairs, examination lights. Everything with a plug or a battery.
- Photograph the nameplate of every device. This captures the manufacturer, model, and serial number without transcription errors.
- Note discrepancies: Equipment not in the existing register, equipment that has been moved without documentation, equipment that is non-functional and has been sitting in storage for months.
Time estimate: A team of 2-3 people can physically verify and tag approximately 50-80 devices per day. For a 200-bed hospital with 500 devices: 7-10 working days. For a 500-bed hospital with 1,500+ devices: 3-4 weeks.
Step 4: Apply QR Labels Correctly
Label placement is not arbitrary. Incorrect placement results in labels that are damaged by cleaning, obscured by accessories, or impossible to scan without moving the equipment.
Placement Rules
- Visible without moving the equipment: The tag should be scannable while the device is in its normal operating position. Do not place tags on the bottom or the back against a wall.
- Away from heat sources: Not near sterilizer doors, autoclave vents, or heating elements. Even polyester labels degrade above 120 degrees Celsius.
- Away from moisture concentration: Not on surfaces that collect condensation, near drain points, or in areas sprayed directly during cleaning.
- Not blocking controls or displays: Never place a tag on a control panel, display screen, or any surface a clinician needs to interact with.
- Consistent location by equipment type: All ventilators get tagged in the same position. All monitors in the same position. This consistency helps staff know where to look without searching the device.
- Surface preparation: Clean the surface with isopropyl alcohol before applying the adhesive label. Allow to dry completely. Press firmly for 30 seconds. For metal surfaces, this is usually sufficient. For textured plastic, use a primer adhesive pad underneath.
Placement by Equipment Type
Ventilators: Right side panel, upper third, away from air intake
Patient Monitors: Top surface or mounting bracket, near power cord entry
Infusion Pumps: Back panel, upper half, visible when mounted on IV pole
Defibrillators: Carry case exterior or device top surface (not near paddles)
Hospital Beds: Foot rail, left side (consistent across all beds)
Wheelchairs: Rear frame, left side, above the axle
Ultrasound: Right side panel, near the handle
ECG Machines: Top surface, near the cable storage area
Autoclaves: Right side panel, away from door seal and steam vents
X-Ray machines: Control panel housing, left sideStep 5: Configure Your Digital Tracking System
What the QR Code Should Encode
There are two approaches, and the choice depends on whether you have tracking software or are starting with a simpler system:
Approach 1: URL-Based (Recommended)
Encode a URL that links to the equipment profile in your asset management system. When scanned, the staff member's phone opens a browser showing the complete equipment record: current location, maintenance history, calibration status, and an option to report an issue or log a transfer.
URL format: https://assets.yourhospital.in/v/ICU-3F-VENT-007
Scanning this URL shows:
- Equipment: Hamilton C6 Ventilator
- Serial: SN-HC6-2024-4521
- Department: ICU, Room 312
- Status: Functional
- Last PM: 2026-02-15 (next due: 2026-03-15)
- Calibration: Valid until 2026-06-30
- [Report Issue] [Log Transfer] [View History]Approach 2: Offline Data (For Hospitals Without Software)
Encode the essential data directly in the QR code as a JSON or plain text string. This works without internet connectivity and without tracking software, but provides less functionality.
Encoded data:
ID: ICU-3F-VENT-007
Name: Hamilton C6 Ventilator
SN: SN-HC6-2024-4521
Dept: ICU
Risk: Critical
PM Freq: MonthlyDatabase Setup
If you are using tracking software (commercial or custom-built), configure these data fields for each equipment record:
Required Fields (NABH Compliance):
- asset_id (unique, follows naming convention)
- equipment_name
- manufacturer, model, serial_number
- department, building, floor, room
- risk_classification (Critical/High/Standard/Low)
- purchase_date, purchase_cost, supplier
- warranty_expiry, amc_vendor, amc_expiry
- condition (Functional/Under Repair/Non-Functional/Condemned)
Maintenance Fields:
- pm_frequency (Monthly/Bi-Monthly/Quarterly/Semi-Annual)
- last_pm_date, next_pm_due
- last_calibration_date, calibration_due
- cumulative_maintenance_cost
- total_downtime_hours
Financial Fields:
- depreciation_method, useful_life_years
- current_book_value
- insurance_coverageStep 6: Roll Out Department by Department
Recommended Rollout Sequence
Week 1-2: ICU (Pilot Department)
Start with the ICU because it has the highest concentration of critical, high-value equipment. If your tagging process works here — where equipment moves frequently, gets cleaned aggressively, and uptime is life-or-death — it will work everywhere. Tag all ventilators, monitors, infusion pumps, defibrillators, and syringe pumps. Train ICU nursing staff and the biomedical engineering team on the scanning workflow.
Week 2-3: Operation Theatre and CSSD
OT has valuable equipment (anesthesia machines, electrosurgical units, surgical lights), and CSSD handles sterilization equipment that needs metalphoto aluminum tags. This tests your label material selection in the harshest environment.
Week 3-4: Radiology and Laboratory
High-value imaging equipment (MRI, CT, X-ray, ultrasound) and laboratory analyzers. These are relatively stationary, making tagging straightforward. Focus on calibration tracking integration for lab equipment.
Week 4-6: Wards, Emergency, and Remaining Departments
General wards have the highest volume of mobile equipment (beds, wheelchairs, IV stands, portable monitors). The ER has equipment that moves between zones rapidly. Complete the remaining departments and validate the full hospital inventory against your database.
Staff Training Protocol
Keep training sessions to 15-20 minutes per department. Cover:
- How to scan the QR code (open camera, point at code, tap the notification)
- How to report a problem (scan code, tap "Report Issue," describe the problem)
- How to log a transfer (scan code when you take equipment to another department)
- What to do if a label is damaged or missing (report to biomedical engineering for replacement)
Step 7: Maintain the System
Tagging is not a one-time project. The system needs ongoing maintenance:
- New equipment: Tag and register every new device on the day it is received, before it enters clinical service
- Damaged labels: Inspect labels during PM visits. Replace any label that is peeling, faded, or not scanning reliably. Keep a stock of blank labels and a portable printer in the biomedical engineering department
- Quarterly audits: Walk through each department with a scanner. Verify that every tagged device is in the database and that every database entry has a physical device. Discrepancies indicate equipment that has been moved without logging, lost, or disposed of without documentation
- Annual physical verification: Full inventory reconciliation, required by NABH and standard accounting practice. With QR codes, this takes hours instead of days
Cost Breakdown: What QR Tagging Actually Costs
For a 200-bed hospital with approximately 500 medical devices:
One-Time Costs:
Polyester labels (500 qty, including spares): Rs 2,500 - 5,000
Metalphoto tags for CSSD/OT equipment (50 qty): Rs 1,000 - 2,000
Label printer (thermal transfer): Rs 15,000 - 30,000
QR code generation software: Free (open source)
Physical verification labor (10 days x 3 staff): Rs 30,000 - 50,000
Staff training (6 sessions x 20 minutes): Rs 5,000 (time cost)
-----------------------------------------------
Total One-Time Cost: Rs 53,500 - 92,000
Annual Recurring Costs:
Replacement labels (10% attrition): Rs 500 - 1,000
Label consumables (ribbon, sheets): Rs 2,000 - 5,000
Quarterly audit labor (4 audits x 2 days): Rs 20,000 - 30,000
-----------------------------------------------
Total Annual Cost: Rs 22,500 - 36,000
Tracking Software (if applicable):
Cloud-based SaaS: Rs 50,000 - 2,00,000/year
OR custom-built on existing infrastructure: Rs 0 (absorbed in IT budget)Compare this to the cost of NOT tagging: Rs 80 lakh to Rs 1.6 crore in annual losses from missing equipment, wasted clinical time, and duplicate purchases. The ROI is measured in weeks, not years.
From concept to deployment, our Custom Healthcare Software Development team ships healthcare applications that clinicians actually use.
The Bottom Line
QR code tagging is the highest-ROI equipment management initiative a hospital can undertake. For under Rs 1 lakh, a 200-bed hospital can tag every medical device, establish a systematic identification convention, and lay the foundation for a complete asset management program that meets NABH standards.
The technology is commoditized. The labels cost rupees. The scanning hardware is already in every staff member's pocket. The only investment required is the organizational discipline to do it systematically: design the numbering convention, choose the right materials, verify every device physically, place labels consistently, and maintain the system over time.
Start with one department. Prove it works. Then scale. The hospital that knows where every piece of equipment is, and what condition it is in, is the hospital that keeps patients safe, passes accreditation audits, and stops hemorrhaging crores in equipment losses every year.