A 400-bed health system in the Midwest processed 2.3 million claims last year. Their denial rate sat at 12.1%—slightly above the national average of 11.8% reported by Experian's 2025 State of Claims. Each denied claim cost them $118 to rework. The math is straightforward: $32.5 million in annual rework costs, consuming 47 FTEs who could have been doing something more valuable than chasing down missing modifier codes.
They did not need another RCM platform. They needed an agent pipeline—a chain of autonomous AI agents, each owning one stage of the revenue cycle, passing structured context to the next, with humans intervening only where clinical judgment or payer negotiation demands it.
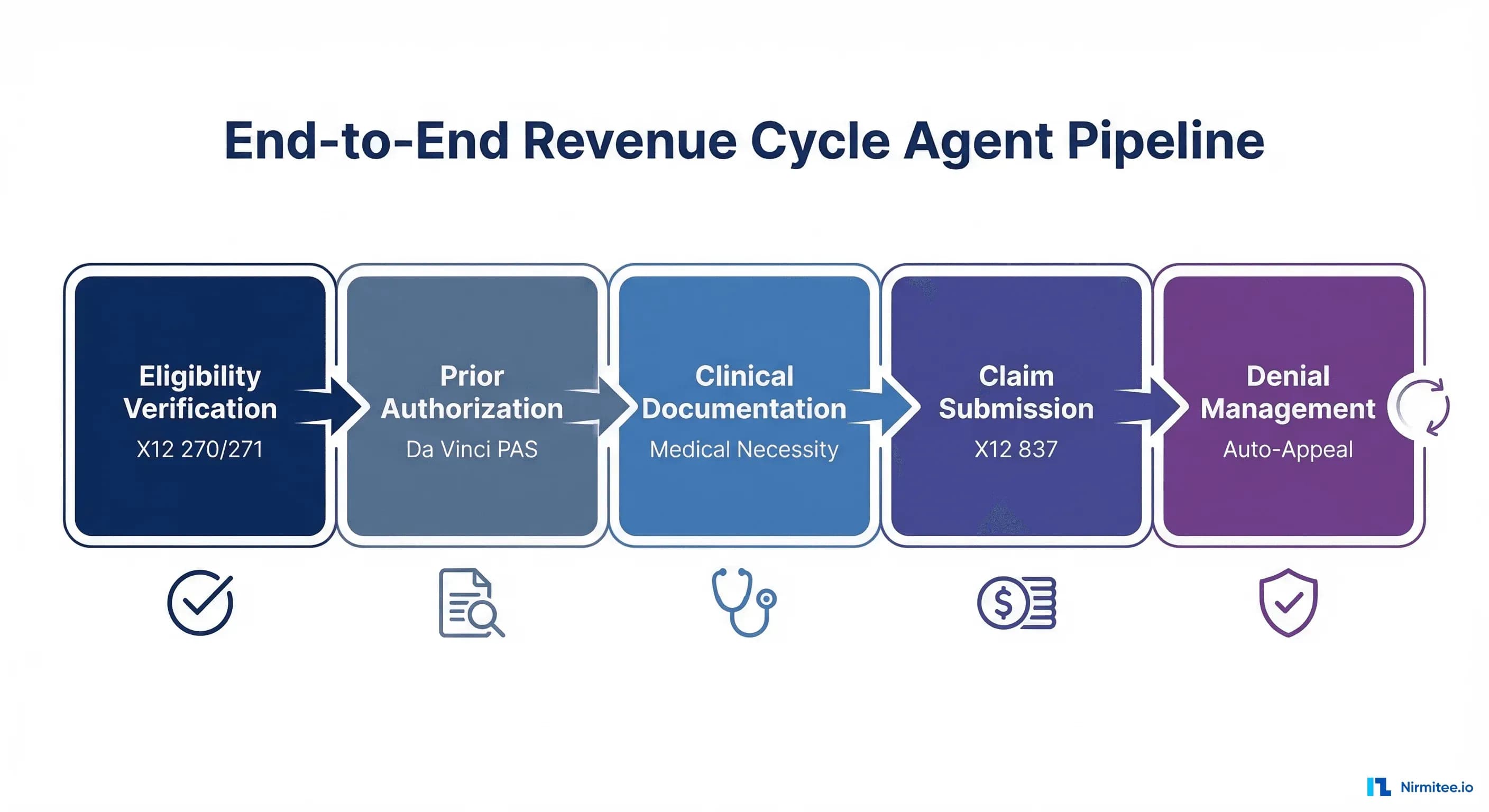
This is the architecture guide for building that pipeline. Five stages. Real transaction formats. Concrete ROI at each step.
The Revenue Cycle as an Agent Pipeline: Architecture Overview
Traditional RCM treats the revenue cycle as a monolithic process—a single team, a single vendor, a single dashboard. The agent pipeline model breaks it into five discrete stages, each with its own AI agent, its own data contracts, and its own success metrics:
| Stage | Agent Role | Standard | Human Touchpoint | Key Metric |
|---|---|---|---|---|
| 1. Eligibility Verification | Coverage discovery & validation | X12 270/271 | Patient identity edge cases | Verification time: 8 sec vs 12 min |
| 2. Prior Authorization | PA requirement detection & submission | Da Vinci PAS / FHIR Claim | Complex medical necessity appeals | Turnaround: 2-24 hrs vs 5-14 days |
| 3. Clinical Documentation | Medical necessity evidence assembly | C-CDA / FHIR DocumentReference | Physician attestation | Documentation completeness: 97% |
| 4. Claim Submission | Clean claim generation & scrubbing | X12 837P/837I | Outlier charge review | Clean claim rate: 96% vs 78% |
| 5. Denial Management | Categorization, appeal, resubmission | X12 835 / CARC/RARC codes | Payer escalation calls | Overturn rate: 72% vs 45% |
Each agent operates asynchronously. Each passes a structured payload to the next. When Stage 1 confirms active coverage with specific benefit details, that context flows directly into Stage 2's prior auth decision logic. When Stage 4 generates a clean claim, Stage 5 already has the original clinical documentation indexed for potential appeals.
This is not a theoretical architecture. The CMS-0057-F final rule mandates FHIR-based prior authorization APIs by January 2027, with operational improvements required by January 2026. Health systems building agent pipelines today are positioning themselves for compliance and competitive advantage simultaneously.
Stage 1: Eligibility Verification Agent (X12 270/271)
Every denied claim that traces back to an eligibility issue represents a failure at the front door. According to industry research, eligibility-related issues remain one of the top three denial reasons across U.S. healthcare. Facilities using real-time 270/271 transactions recover an average of $4.80 in revenue for every $1 spent on automation.
What the Agent Does
The eligibility verification agent fires on three triggers: appointment scheduling, 48-hour pre-visit batch, and day-of check-in. For each encounter, it:
- Constructs an X12 270 transaction with the patient's subscriber ID, group number, date of service, and service type codes (e.g., 30 for health benefit plan coverage, 47 for hospital, 88 for pharmacy)
- Routes through the appropriate clearinghouse (Availity, Change Healthcare, Waystar) or directly to the payer's HIPAA Eligibility Transaction System (HETS for Medicare)
- Parses the 271 response, extracting active/inactive status, plan details, copay amounts, deductible remaining, out-of-pocket maximums, and coordination of benefits information
- Flags discrepancies: coverage terminated, benefits exhausted, secondary insurance detected, plan type mismatch for scheduled service
- Updates the EHR patient record with verified coverage details via FHIR Coverage resource
The Code: Building a 270 Request
import json
from datetime import datetime
def build_270_request(patient, encounter):
"""Construct X12 270 eligibility inquiry."""
return {
"transaction_set": "270",
"submitter": {
"organization": "ACME_HEALTH_SYSTEM",
"contact": "RCM_AGENT_01"
},
"receiver": {
"payer_id": patient["primary_payer_id"],
"name": patient["payer_name"]
},
"subscriber": {
"member_id": patient["subscriber_id"],
"first_name": patient["first_name"],
"last_name": patient["last_name"],
"dob": patient["date_of_birth"],
"group_number": patient.get("group_number")
},
"inquiry": {
"date_of_service": encounter["scheduled_date"],
"service_type_codes": [
"30", # Health Benefit Plan Coverage
map_service_type(encounter["encounter_type"])
],
"procedure_codes": encounter.get("cpt_codes", [])
},
"trace_number": f"ELG-{datetime.now().strftime('%Y%m%d%H%M%S')}"
}
def parse_271_response(response):
"""Extract coverage details from 271 response."""
coverage = {
"status": "ACTIVE" if response["eligibility_code"] == "1" else "INACTIVE",
"plan_name": response.get("plan_description"),
"copay": extract_benefit(response, "B"),
"deductible_remaining": extract_benefit(response, "C"),
"oop_remaining": extract_benefit(response, "G"),
"coinsurance_pct": extract_benefit(response, "A"),
"prior_auth_required": response.get("auth_indicator") == "Y",
"effective_date": response.get("plan_begin_date"),
"coordination_of_benefits": response.get("cob_info")
}
return coverageWhat Stays Human
Patient identity resolution when demographics do not match. Patients with name changes, transposed digits in subscriber IDs, or dual-eligible Medicare/Medicaid scenarios. The agent flags these as exceptions; a staff member resolves them with a 2-minute phone call rather than a 12-minute manual verification of the entire coverage.
ROI Math
At $3.41 per manual eligibility check (CAQH 2024 Index) versus $0.05 per automated transaction: a 500-provider health system running 850,000 eligibility checks per year saves $2.86 million annually. Add the downstream impact—facilities moving from manual to automated verification reduced eligibility-related write-offs by 61% in the first year (HFMA 2024).
Stage 2: Prior Authorization Agent (Da Vinci PAS)
Prior authorization is the single most expensive administrative transaction in U.S. healthcare. The total annual cost across the system is $93.3 billion—$26.7 billion borne by physicians alone. Physicians spend an average of 1 hour per week on PA, while billing specialists spend 11 hours per week (AMA 2025).
What the Agent Does
The PA agent monitors the EHR order queue. When a new order fires (imaging study, surgical procedure, specialty medication), it:
- Checks payer rules: Queries an internal rules database mapping CPT/HCPCS codes to payer-specific PA requirements. Not all services require PA—the agent prevents unnecessary submissions that waste time and create audit risk
- Assembles the FHIR Claim resource: Builds a Da Vinci PAS-compliant request with the Claim resource (category: preauthorization), supporting clinical data as DocumentReference attachments, and the relevant diagnosis (Condition) and procedure (ServiceRequest) resources
- Submits via FHIR API: Posts the Bundle to the payer's $submit endpoint. Under CMS-0057-F, payers must respond within 72 hours for urgent requests and 7 calendar days for standard
- Monitors and parses the response: ClaimResponse with outcome codes—approved, denied, pended for additional information
- Triggers Stage 3 when additional clinical documentation is requested
The Code: Da Vinci PAS Submission
import requests
from fhir.resources.claim import Claim
from fhir.resources.bundle import Bundle
def submit_prior_auth(order, patient_coverage, clinical_docs):
"""Submit PA request via Da Vinci PAS FHIR API."""
claim = Claim(
status="active",
type={"coding": [{"system": "http://terminology.hl7.org/CodeSystem/claim-type",
"code": "professional"}]},
use="preauthorization",
patient={"reference": f"Patient/{order['patient_id']}"},
provider={"reference": f"Organization/{order['provider_org']}"},
priority={"coding": [{"code": "normal"}]},
insurance=[{
"sequence": 1,
"focal": True,
"coverage": {"reference": f"Coverage/{patient_coverage['id']}"}
}],
item=[{
"sequence": 1,
"productOrService": {
"coding": [{"system": "http://www.ama-assn.org/go/cpt",
"code": order["cpt_code"]}]
},
"servicedDate": order["requested_date"],
"quantity": {"value": order.get("units", 1)}
}],
diagnosis=[{
"sequence": 1,
"diagnosisCodeableConcept": {
"coding": [{"system": "http://hl7.org/fhir/sid/icd-10-cm",
"code": order["icd10_code"]}]
}
}]
)
bundle = Bundle(
type="collection",
entry=[
{"resource": claim.dict()},
*[{"resource": doc} for doc in clinical_docs]
]
)
response = requests.post(
f"{patient_coverage['payer_pas_endpoint']}/$submit",
json=bundle.dict(),
headers={"Authorization": f"Bearer {get_payer_token()}"}
)
return parse_claim_response(response.json())What Stays Human
Peer-to-peer reviews. When a payer denies a PA and offers a physician-to-physician discussion, that conversation requires clinical reasoning, persuasion, and the ability to cite specific patient circumstances. The agent prepares the brief—pulling relevant lab results, imaging reports, and clinical notes—but the physician makes the case.
ROI Math
Manual PA costs $6 per transaction (CAQH 2024). Automated PA via FHIR API: $0.50. For a health system processing 120,000 PAs per year, that is $660,000 in direct savings. The bigger number: reducing PA turnaround from 5-14 days to 2-24 hours means patients receive care faster, reducing downstream complications and readmissions.
Stage 3: Clinical Documentation Agent
The clinical documentation agent is the bridge between the clinical and financial sides of healthcare. When a prior auth request gets pended or denied for insufficient documentation, this agent assembles the medical necessity case.
What the Agent Does
- Extracts relevant clinical data from the EHR: Problem list, medication history, lab results, imaging reports, prior treatment attempts—all mapped to the specific payer's medical policy criteria
- Structures the narrative: Generates a medical necessity letter that maps clinical findings to the payer's published criteria. For example: "Patient has failed conservative therapy (physical therapy x 12 sessions, 2024-08 through 2024-11) and NSAID trial (ibuprofen 800mg TID x 6 weeks) prior to requesting MRI of lumbar spine"
- Identifies documentation gaps: If the EHR lacks a required data element (e.g., BMI for bariatric surgery PA, or HbA1c for continuous glucose monitor), the agent creates a task for the clinical team with the specific missing element
- Packages as C-CDA or FHIR DocumentReference: Attaches the compiled documentation to the PA resubmission in the format the payer accepts
Research shows AI documentation tools can reduce charting time by up to 70% (Healos 2026). For revenue cycle specifically, the impact is in documentation completeness—capturing the clinical evidence that prevents denials before they happen.
What Stays Human
Physician attestation. The agent drafts the medical necessity narrative, but a physician must review and sign. This is both a regulatory requirement and a clinical safety guardrail. The agent reduces physician time from 15 minutes of chart-digging to 90 seconds of review-and-sign.
Stage 4: Claim Submission Agent (X12 837)
Nearly 95% of provider claims are already submitted electronically via X12 837. The opportunity is not in going electronic—it is in going intelligent. The difference between a clean claim rate of 78% and 96% is millions of dollars in rework costs and weeks of cash flow delay.
What the Agent Does
- Pre-submission scrubbing: Validates every field against payer-specific rules before the claim leaves the building. Not just format validation (is the NPI 10 digits?) but semantic validation (does this E/M code match the documented complexity level?)
- Cross-references Stage 1 and Stage 2 outputs: Confirms coverage is still active (coverage can change between scheduling and service), verifies PA approval number is attached, checks that authorized units match billed units
- Optimizes coding: Identifies missed modifiers, unbundling opportunities, and correct place-of-service codes. Not upcoding—accurate coding that captures the full complexity of the service delivered
- Routes to the correct payer: Handles coordination of benefits logic, splitting claims across primary and secondary payers based on Stage 1's COB analysis
- Generates the X12 837P (professional) or 837I (institutional) transaction: With all loops, segments, and qualifiers populated correctly
The Code: Claim Validation Pipeline
class ClaimValidationPipeline:
def __init__(self, payer_rules_db):
self.rules = payer_rules_db
self.validators = [
self.validate_patient_demographics,
self.validate_coverage_active,
self.validate_prior_auth,
self.validate_diagnosis_codes,
self.validate_procedure_codes,
self.validate_modifiers,
self.validate_place_of_service,
self.validate_npi_taxonomy,
self.validate_timely_filing,
]
def scrub(self, claim, eligibility_result, pa_result):
"""Run all validations. Return clean claim or error list."""
errors = []
warnings = []
for validator in self.validators:
result = validator(claim, eligibility_result, pa_result)
errors.extend(result.get("errors", []))
warnings.extend(result.get("warnings", []))
if not errors:
return {"status": "CLEAN", "claim": claim, "warnings": warnings}
return {"status": "HOLD", "errors": errors, "warnings": warnings}
def validate_prior_auth(self, claim, elig, pa):
"""Ensure PA number matches and covers billed services."""
if not pa:
return {"errors": ["Prior auth required but not found"]}
if pa["status"] != "APPROVED":
return {"errors": [f"PA status is {pa['status']}, not APPROVED"]}
if claim["units"] > pa["authorized_units"]:
return {"errors": [
f"Billed units ({claim['units']}) exceed authorized ({pa['authorized_units']})"
]}
if claim["service_date"] > pa["expiration_date"]:
return {"errors": ["Service date after PA expiration"]}
return {"warnings": [] if pa["remaining_units"] > 5
else [f"Only {pa['remaining_units']} authorized units remaining"]}What Stays Human
Outlier charge review. When the agent flags a claim that is 3x the average charge for a given DRG, a human reviews it. This could be a legitimate complex case or a data entry error. The agent provides the context (comparison data, clinical documentation)—the human makes the call.
ROI Math
The healthcare sector avoided over $11.2 billion in costs in 2023 by using electronic versus manual claim submission. For a single health system, moving clean claim rates from 78% to 96% on 200,000 annual claims at $25 per rework: $900,000 saved in rework costs plus 15-day improvement in days-in-accounts-receivable.
Stage 5: Denial Management and Auto-Appeal Agent
Here is where the revenue cycle bleeds most visibly. Initial claim denial rates hit 11.8% in 2024—up from 10.2% just a few years prior. More alarming: payers are deploying AI to review and deny claims at scale and speed that manual provider workflows cannot match. This is an arms race, and providers without their own AI agents are bringing a fax machine to a gunfight.
What the Agent Does
- Ingests and parses X12 835 remittance advice: Extracts CARC (Claim Adjustment Reason Code) and RARC (Remittance Advice Remark Code) for every denied or adjusted line item
- Categorizes by root cause: Maps denial codes to actionable categories—missing information (CO-16), lack of medical necessity (CO-50), duplicate claim (CO-18), timely filing (CO-29), authorization issues (CO-197)
- Routes to the optimal recovery path: Not all denials deserve the same response. The agent calculates expected recovery value (probability of overturn x claim amount) and prioritizes accordingly
- Generates appeal letters: For medical necessity denials, pulls the original clinical documentation from Stage 3, adds any new clinical evidence, and drafts a payer-specific appeal letter citing the relevant medical policy and clinical guidelines
- Tracks appeal deadlines: Payer-specific timely filing limits for appeals range from 30 to 365 days. Missing a deadline means losing the revenue permanently
- Resubmits corrected claims: For coding errors or missing information, fixes the issue and resubmits without human intervention
What Stays Human
Payer escalation. When an appeal is denied and the claim amount exceeds a configurable threshold (typically $5,000+), the agent escalates to a human specialist who can negotiate with the payer representative. The agent provides the full case file, appeal history, and suggested negotiation points.
ROI Math
70% of denied claims are eventually paid, but only after costly reviews (OS Healthcare 2025). AI-powered denial management improves overturn rates from 45% to 72% and reduces appeal cycle time from 45 days to 4 days. For a health system with $15M in annual denials: recovering an additional 27% = $4.05 million in recovered revenue.
The Complete Pipeline: Integration Architecture
Individual agents deliver incremental value. The pipeline delivers transformational value. Here is how the five stages connect:
| Integration Point | Data Passed | Why It Matters |
|---|---|---|
| Stage 1 → Stage 2 | Coverage details, PA requirement flags | Prevents unnecessary PA submissions; pre-populates payer info |
| Stage 2 → Stage 3 | Pended items, required documentation list | Targets documentation assembly to specific payer criteria |
| Stage 3 → Stage 4 | Complete clinical documentation package | Ensures claims ship with supporting evidence already attached |
| Stage 1+2+3 → Stage 4 | Eligibility, PA number, clinical docs | Single source of truth for clean claim generation |
| Stage 4 → Stage 5 | Original claim, all supporting context | Appeals reference the exact documentation submitted with the claim |
| Stage 5 → Stage 1 | Denial patterns, payer behavior data | Feeds back into eligibility rules; prevents repeat denials |
The feedback loop from Stage 5 to Stage 1 is the most undervalued integration. When the denial agent identifies that Blue Cross of Illinois is denying 40% of MRI orders without a specific CPT modifier, that intelligence flows back to the eligibility and PA agents to prevent the same denial on future claims.
Technology Stack for the Agent Pipeline
Building this pipeline requires specific infrastructure choices. Based on production deployments we have guided at Nirmitee, here is the stack that works:
- Agent orchestration: LangGraph or Temporal for stateful, long-running workflows with HIPAA-compliant audit trails
- EHR integration: FHIR R4 APIs via SMART on FHIR for reading patient data; HL7v2 ADT feeds for real-time event triggers
- EDI processing: Stedi or custom X12 parser for 270/271, 837, and 835 transactions
- Payer connectivity: Clearinghouse APIs (Availity, Change Healthcare) or direct payer connections via Da Vinci PAS
- Rules engine: Payer-specific rules database with version control—payer policies change quarterly
- Monitoring: OpenTelemetry for pipeline observability; real-time dashboards for clean claim rates, denial rates, and appeal outcomes
Implementation Roadmap: 90 Days to Production
Do not try to build all five stages at once. The proven sequence:
Weeks 1-4: Stage 1 (Eligibility)
Start here because it delivers immediate, measurable ROI with the lowest integration complexity. X12 270/271 is a well-established standard, clearinghouse APIs are mature, and the risk profile is low—a failed eligibility check does not delay patient care, it just adds a manual verification step.
Weeks 5-8: Stage 4 (Claim Scrubbing)
Yes, Stage 4 before Stage 2. Clean claim submission has a more direct revenue impact than prior auth automation in most health systems. You already have the eligibility data from Stage 1 feeding into the claim validation pipeline.
Weeks 9-12: Stages 2 + 3 (Prior Auth + Documentation)
Build these together because they are tightly coupled. The PA agent needs the documentation agent for pended requests, and the documentation agent's primary trigger is PA-related.
Weeks 13-16: Stage 5 (Denial Management)
Deploy last because it benefits most from having all upstream stages operational. The denial agent's effectiveness increases dramatically when it has access to the original eligibility check, PA approval, clinical documentation, and claim details from Stages 1-4.
Measuring Pipeline Health: The Dashboard
Revenue cycle directors need five numbers on a daily basis:
- Pre-service eligibility verification rate: Target 98%+ of scheduled encounters verified 48 hours before service
- PA turnaround time: Median hours from order to decision. Target: under 24 hours for standard requests
- Clean claim rate: Percentage of claims accepted on first submission. Target: 96%+
- Initial denial rate: Target below 5% (the national average is 11.8%)
- Net collection rate: Total collected / total expected. Target: 96%+ with the pipeline reducing leakage at every stage
Track these daily. Review weekly. The pipeline should show measurable improvement within 30 days of each stage going live.
Common Pitfalls and How to Avoid Them
After deploying revenue cycle agent pipelines across multiple health systems, we have seen the same mistakes repeat:
- Building Stage 5 first: Denial management is the most visible pain point, so organizations want to start there. But denial agents without upstream data are just faster fax machines. Build the pipeline in order.
- Ignoring payer-specific rules: Each payer has different PA requirements, modifier rules, and appeal processes. A generic rules engine fails. You need payer-specific configuration that updates quarterly.
- No human-in-the-loop design: Regulators and clinicians will not trust a fully autonomous revenue cycle. Design clear escalation paths with defined thresholds for human review. See our analysis of common scale-up traps for health system AI deployments.
- Underinvesting in monitoring: A revenue cycle pipeline without observability is a liability. Every agent action must be auditable. Every decision must be traceable. Healthcare downtime costs $7,900 per minute—your RCM pipeline needs the same monitoring rigor as clinical systems.
The Bottom Line: What This Pipeline Delivers
For a mid-size health system (400 beds, $800M net patient revenue):
| Metric | Before Pipeline | After Pipeline | Annual Impact |
|---|---|---|---|
| Eligibility verification cost | $3.41/check | $0.05/check | $2.86M saved |
| Prior auth turnaround | 5-14 days | 2-24 hours | Faster patient access |
| Clean claim rate | 78% | 96% | $900K saved in rework |
| Denial rate | 11.8% | 4.2% | $5.8M fewer denials |
| Appeal overturn rate | 45% | 72% | $4.05M recovered |
| Staff reallocation | 47 FTEs on rework | 12 FTEs on exceptions | 35 FTEs redirected |
Combined annual impact: $13.6 million in recovered and saved revenue. Implementation cost: approximately $300-500K including integration, rules configuration, and change management. Payback period: 2-3 weeks.
The revenue cycle agent pipeline is not a future concept. The standards exist (X12, FHIR, Da Vinci PAS). The regulatory mandate is in place (CMS-0057-F). The ROI math is proven. The question is not whether to build it, but how fast you can deploy.
At Nirmitee, we architect and build end-to-end revenue cycle agent pipelines for health systems and healthtech companies. From X12 integration to FHIR-based prior auth to AI-powered denial management—we ship production systems, not prototypes. Talk to our team about your revenue cycle automation roadmap.
Related reading
For more insights, explore our guides on what AI agents do in healthcare and FHIR in Modern Healthcare.
You may also find value in EHR Software Development Guide and Building a Healthtech App.


