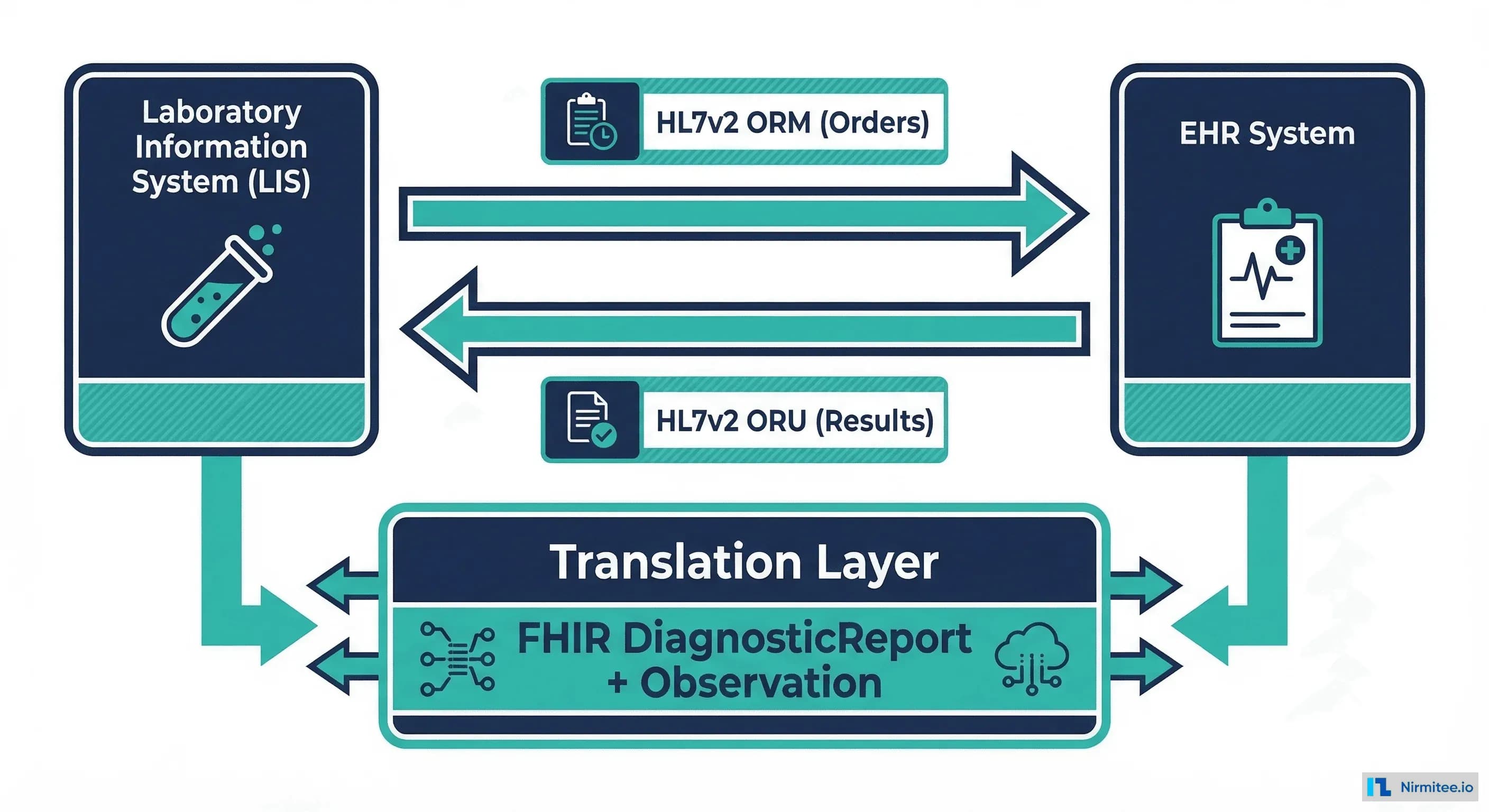
If you have built integrations between clinical systems, you already know the truth that vendor sales decks gloss over: lab integration is the single most painful point-to-point interface in healthcare IT. Not ADT feeds. Not scheduling. Not even medication reconciliation. The LIS-to-EHR pipeline, built on HL7v2 ORM and ORU messages, is where integration engineers lose sleep, because every reference lab, every hospital lab, and every point-of-care analyzer has its own interpretation of what a "standard" HL7 message should look like.
This guide is written for engineers who are about to map their first (or fiftieth) lab interface. We will walk through the HL7v2 ORM and ORU message structures, map every critical field to its FHIR R4 equivalent, and cover the production gotchas that textbooks skip. If you have ever stared at an OBX segment wondering why a CBC panel arrived as seventeen individual results instead of a grouped panel, this article is for you.
Why Lab Integration Is the Messiest Interface in Healthcare
Healthcare interoperability has made genuine progress in the last decade. CDA documents gave way to FHIR bundles. Argonaut accelerated adoption. CMS mandates forced payer APIs into production. But lab data? Lab data still moves on HL7v2 pipes that were designed in the 1990s, and the reason is straightforward: the LIS ecosystem is extraordinarily fragmented.
Consider the landscape a typical health system faces:
- Reference labs (Quest, Labcorp, BioReference) each send ORU messages with their own OBX segment ordering, proprietary result codes, and non-standard abnormal flag values.
- Hospital core labs running Sunquest, Cerner PathNet, or Epic Beaker produce ORU feeds that reflect their internal data models, not the receiving EHR's expectations.
- Point-of-care devices (i-STAT, Piccolo, glucometers) generate results that may arrive as ORU messages, as device-specific protocols, or as manual entries that someone typed into an interface engine.
- Specialty labs (genetics, toxicology, pathology) push results with embedded PDF reports in OBX-5, multi-line text narratives, or structured data that uses local coding systems instead of LOINC.
The HL7v2 specification is permissive by design. It defines segments and field positions, but it does not enforce content. Two labs can send a perfectly valid ORU message for the same test, and those messages can look nothing alike. That is the fundamental problem, and it is why every lab interface requires custom mapping work.
HL7v2 ORM: The Order Message
Before results flow back, orders flow out. The ORM (Order Message) is what the EHR sends to the LIS when a clinician orders a lab test. Understanding ORM structure matters because the order context directly affects how you interpret the results that come back.
Core ORM Segments
A typical ORM^O01 message contains these segments in order:
MSH|^~\&|EHR_SYSTEM|FACILITY_A|LAB_SYSTEM|REFERENCE_LAB|20260315120000||ORM^O01|MSG00001|P|2.5.1
PID|1||MRN12345^^^FACILITY_A^MR||DOE^JANE^M||19850315|F|||123 MAIN ST^^ANYTOWN^NY^12345
PV1|1|O|CLINIC_A^^^^OUTPATIENT|||SMITH^JOHN^DR^^^MD|||||||||||||VISIT98765
ORC|NW|ORD001|||||^^^20260315120000^^R||20260315120000|NURSE_JONES|SMITH^JOHN^DR^^^MD
OBR|1|ORD001||58410-2^CBC WITH DIFFERENTIAL^LN|||20260315120000||||||||SMITH^JOHN^DR^^^MD||||||||||1^^^20260315120000^^RLet us break down what each segment does:
- MSH (Message Header) — Identifies the sending and receiving systems, message type (ORM^O01), control ID for deduplication, and HL7 version. The field separator and encoding characters in MSH-1 and MSH-2 are critical; get them wrong and your parser chokes on the entire message.
- PID (Patient Identification) — Contains the patient's MRN (PID-3), name (PID-5), date of birth (PID-7), sex (PID-8), and address (PID-11). PID-3 is the join key you will use to match orders to patients in your FHIR Patient resource.
- PV1 (Patient Visit) — Captures the encounter context: patient class (inpatient, outpatient, emergency in PV1-2), attending physician (PV1-7), and visit number (PV1-19). This maps to the FHIR Encounter reference on your ServiceRequest.
- ORC (Common Order) — The order control segment. ORC-1 is the order control code (NW = new order, CA = cancel, XO = change). ORC-2 is the placer order number. ORC-12 is the ordering provider. This segment carries the workflow state of the order.
- OBR (Observation Request) — The actual test being ordered. OBR-4 is the universal service identifier, the code that tells the lab what to run. OBR-7 is the requested collection date/time. OBR-16 is the ordering provider. For FHIR mapping, OBR-4 is your
ServiceRequest.code.
HL7v2 ORU: The Result Message
The ORU^R01 message is where the real complexity lives. This is the lab sending results back to the EHR, and it is the message type that causes the most integration failures in production.
Core ORU Segments
MSH|^~\&|LAB_SYSTEM|REFERENCE_LAB|EHR_SYSTEM|FACILITY_A|20260315143000||ORU^R01|MSG00042|P|2.5.1
PID|1||MRN12345^^^FACILITY_A^MR||DOE^JANE^M||19850315|F
OBR|1|ORD001|LAB_ACC_001|58410-2^CBC WITH DIFFERENTIAL^LN|||20260315121500|||||||20260315121500|BLOOD^VENOUS|SMITH^JOHN^DR^^^MD||||||20260315143000|||F
OBX|1|NM|6690-2^LEUKOCYTES [#/VOLUME] IN BLOOD^LN||7.2|10*3/uL|4.5-11.0|N|||F
OBX|2|NM|789-8^ERYTHROCYTES [#/VOLUME] IN BLOOD^LN||4.85|10*6/uL|4.10-5.10|N|||F
OBX|3|NM|718-7^HEMOGLOBIN [MASS/VOLUME] IN BLOOD^LN||14.2|g/dL|12.0-16.0|N|||F
OBX|4|NM|4544-3^HEMATOCRIT [VOLUME FRACTION] OF BLOOD^LN||42.1|%|36.0-46.0|N|||F
OBX|5|NM|787-2^MCV [ENTITIC VOLUME]^LN||86.8|fL|80.0-100.0|N|||F
OBX|6|NM|785-6^MCH [ENTITIC MASS]^LN||29.3|pg|27.0-33.0|N|||F
OBX|7|NM|786-4^MCHC [MASS/VOLUME]^LN||33.7|g/dL|32.0-36.0|N|||F
OBX|8|NM|777-3^PLATELETS [#/VOLUME] IN BLOOD^LN||245|10*3/uL|150-400|N|||FThe critical fields in the ORU message:
- OBR-4 (Universal Service Identifier) — The LOINC code (or local code) for the panel or test ordered. In our example,
58410-2is the LOINC for CBC with Differential. This becomes yourDiagnosticReport.code. - OBR-25 (Result Status) — Single character:
Pfor preliminary,Ffor final,Cfor corrected,Xfor cancelled. This maps directly toDiagnosticReport.status. - OBX-2 (Value Type) — Tells your parser how to interpret OBX-5.
NMmeans numeric,STmeans string,CEmeans coded entry,TXmeans free text. This determines which FHIRvalue[x]type to use. - OBX-3 (Observation Identifier) — The LOINC code for the individual result.
6690-2is Leukocytes in Blood. This becomesObservation.code. - OBX-5 (Observation Value) — The actual result value. For numeric types, this is the number. For coded entries, this is a coded triplet. For text, this can be multi-line.
- OBX-6 (Units) — The unit of measure, ideally in UCUM format. Maps to
Observation.valueQuantity.unit. - OBX-7 (Reference Range) — The normal range, typically formatted as
low-high. Maps toObservation.referenceRange. - OBX-8 (Abnormal Flags) —
Nfor normal,Hfor high,Lfor low,HHfor critical high,LLfor critical low,Afor abnormal. Maps toObservation.interpretation.
OBX Value Types: The Parsing Minefield
The OBX-2 field is a two-character code that changes how you must parse OBX-5. Getting this wrong means corrupted data in your FHIR Observations. Here is the complete mapping:
| OBX-2 Type | Description | FHIR value[x] | Example OBX-5 |
|---|---|---|---|
| NM | Numeric | valueQuantity | 7.2 |
| ST | String | valueString | POSITIVE |
| CE | Coded Entry | valueCodeableConcept | 260373001^Detected^SCT |
| TX | Text (multi-line) | valueString | See comment below |
| SN | Structured Numeric | valueQuantity or valueRange | <10 or >500 |
| DT | Date | valueDateTime | 20260315 |
| FT | Formatted Text | valueString | \.br\Line one\.br\Line two |
| ED | Encapsulated Data | Binary (as media) | Base64-encoded PDF |
The SN (Structured Numeric) type deserves special attention. Labs use it for results like <10 or >500 where the value is a comparator plus a number. In HL7v2, this arrives as a multi-component field: ^<^10. In FHIR, you have two choices: encode it as a valueQuantity with a comparator, or as a valueString. The semantically correct approach is valueQuantity with the comparator field set.
The ED (Encapsulated Data) type is how labs send PDF reports. The base64-encoded PDF lives in OBX-5, and you need to decode it, store it as a FHIR Binary resource, and reference it from DiagnosticReport.presentedForm. Genetics labs and pathology reports frequently arrive this way.
The FHIR Mapping: ORM to ServiceRequest, ORU to DiagnosticReport
Now for the part you came here for. How do HL7v2 lab messages translate into FHIR R4 resources?
ORM Maps to ServiceRequest + Task
An ORM^O01 message becomes a FHIR ServiceRequest resource that represents the lab order. If you need to track fulfillment state (accepted, in-progress, completed), you also create a Task resource. Here is the mapping:
{
"resourceType": "ServiceRequest",
"id": "lab-order-001",
"status": "active",
"intent": "order",
"code": {
"coding": [{
"system": "http://loinc.org",
"code": "58410-2",
"display": "CBC with Differential"
}]
},
"subject": {
"reference": "Patient/patient-jane-doe"
},
"encounter": {
"reference": "Encounter/visit-98765"
},
"requester": {
"reference": "Practitioner/dr-smith",
"display": "Dr. John Smith"
},
"authoredOn": "2026-03-15T12:00:00Z",
"specimen": [{
"reference": "Specimen/specimen-001"
}]
}ORU Maps to DiagnosticReport + Observation Bundle
An ORU^R01 message becomes a DiagnosticReport resource that references individual Observation resources for each OBX segment. This is the core transformation:
{
"resourceType": "DiagnosticReport",
"id": "cbc-report-001",
"status": "final",
"code": {
"coding": [{
"system": "http://loinc.org",
"code": "58410-2",
"display": "CBC with Differential"
}]
},
"subject": {
"reference": "Patient/patient-jane-doe"
},
"effectiveDateTime": "2026-03-15T12:15:00Z",
"issued": "2026-03-15T14:30:00Z",
"result": [
{"reference": "Observation/wbc-001"},
{"reference": "Observation/rbc-001"},
{"reference": "Observation/hgb-001"},
{"reference": "Observation/hct-001"},
{"reference": "Observation/plt-001"}
],
"basedOn": [{
"reference": "ServiceRequest/lab-order-001"
}]
}Each OBX segment becomes an Observation. Here is the WBC result mapped to FHIR:
{
"resourceType": "Observation",
"id": "wbc-001",
"status": "final",
"code": {
"coding": [{
"system": "http://loinc.org",
"code": "6690-2",
"display": "Leukocytes [#/volume] in Blood"
}]
},
"subject": {
"reference": "Patient/patient-jane-doe"
},
"valueQuantity": {
"value": 7.2,
"unit": "10*3/uL",
"system": "http://unitsofmeasure.org",
"code": "10*3/uL"
},
"referenceRange": [{
"low": {"value": 4.5, "unit": "10*3/uL"},
"high": {"value": 11.0, "unit": "10*3/uL"}
}],
"interpretation": [{
"coding": [{
"system": "http://terminology.hl7.org/CodeSystem/v3-ObservationInterpretation",
"code": "N",
"display": "Normal"
}]
}]
}The Complete Field Mapping Reference
Here is the definitive mapping table between HL7v2 ORM/ORU fields and FHIR R4 resources. Pin this to your wall.
| HL7v2 Field | FHIR Resource | FHIR Path | Notes |
|---|---|---|---|
| PID-3 | Patient | Patient.identifier | MRN; use assigner for facility |
| PID-5 | Patient | Patient.name | Map family, given, prefix components |
| PV1-2 | Encounter | Encounter.class | I=inpatient, O=outpatient, E=emergency |
| PV1-19 | Encounter | Encounter.identifier | Visit number |
| ORC-1 | Task | Task.status | NW=requested, CA=cancelled, SC=active |
| ORC-2 | ServiceRequest | ServiceRequest.identifier | Placer order number |
| ORC-3 | ServiceRequest | ServiceRequest.identifier | Filler order number (lab's ID) |
| OBR-4 | ServiceRequest / DiagnosticReport | .code | Universal service ID; use LOINC |
| OBR-7 | DiagnosticReport | .effectiveDateTime | Observation date/time |
| OBR-22 | DiagnosticReport | .issued | Results report date/time |
| OBR-25 | DiagnosticReport | .status | P=preliminary, F=final, C=corrected |
| OBX-3 | Observation | .code | Observation identifier; LOINC code |
| OBX-5 | Observation | .value[x] | Type determined by OBX-2 |
| OBX-6 | Observation | .valueQuantity.unit | Units; prefer UCUM |
| OBX-7 | Observation | .referenceRange | Parse low-high format |
| OBX-8 | Observation | .interpretation | Map to v3-ObservationInterpretation |
| OBX-11 | Observation | .status | F=final, P=preliminary, C=corrected |
Production Gotchas That Will Bite You
The mapping table looks clean. Production is not. Here are the issues that cause real failures in live lab interfaces.
1. Panels vs. Individual Tests
A CBC with Differential is a panel, a single order that produces multiple results. Some labs send this as one OBR with multiple OBX segments underneath (correct). Others send it as multiple OBR segments, each with one OBX (technically valid but harder to group). A few send a parent OBR with child OBR segments linked by OBR-29 (Parent Result Observation Identifier).
In FHIR, you handle this with DiagnosticReport.result[] referencing multiple Observations, and optionally using Observation.hasMember[] for hierarchical grouping. But first you have to detect whether the incoming HL7 message uses flat or nested grouping, and that varies by vendor.
2. Abnormal Flag Mapping Is Not 1:1
The HL7v2 spec defines abnormal flags in Table 0078: N, H, L, HH, LL, A, AA, and more. FHIR uses the v3-ObservationInterpretation code system. Most flags map cleanly, but watch for these traps:
- Vendor-specific flags — Some labs send
*for abnormal,**for critical, or proprietary codes likeABN. You need a lookup table per lab vendor. - Multiple flags — OBX-8 can repeat. A result might be both
H(high) andA(abnormal). In FHIR,interpretationis an array, so you can include both. - Empty flags — Some labs omit OBX-8 entirely for normal results instead of sending
N. Your mapper should default to "Normal" when the flag is absent and the value falls within the reference range.
3. Preliminary vs. Final Results and the Overwrite Problem
Labs frequently send preliminary results (OBR-25 = P) followed by final results (OBR-25 = F). The mapping to DiagnosticReport.status is straightforward:
P→preliminaryF→finalC→correctedX→cancelled
The gotcha is idempotency. When the final result arrives, you must update the existing DiagnosticReport and its Observations, not create new ones. Use ORC-2 (placer order number) + ORC-3 (filler order number) as your correlation key. If you create duplicate resources, clinicians see the same result twice in their chart, and that is a patient safety issue.
Even worse: some labs send a corrected result (C) after the final. Your system must handle the state machine: preliminary → final → corrected. Going backward (final → preliminary) should be rejected or flagged.
4. Missing or Local LOINC Codes
In an ideal world, every OBX-3 contains a LOINC code. In reality, many labs send local codes in the first component and LOINC in an alternate component, or no LOINC at all. A typical OBX-3 from a lab that does it right:
OBX|1|NM|6690-2^LEUKOCYTES [#/VOLUME] IN BLOOD^LN||7.2|10*3/uLA typical OBX-3 from a lab that does not:
OBX|1|NM|WBC^WHITE BLOOD COUNT^L||7.2|10*3/uLThat L in the third component means "Local" coding system. You now need a mapping table that translates WBC^L to LOINC 6690-2. For a large reference lab with thousands of test codes, building and maintaining this table is a project in itself. This is where LOINC adoption matters: without standard codes, semantic interoperability is impossible. You cannot aggregate results across systems if one calls it WBC and another calls it 6690-2.
5. Timezone and Date/Time Parsing
HL7v2 timestamps use the format YYYYMMDDHHMMSS[+/-ZZZZ]. The timezone offset is optional, and many labs omit it. When OBR-7 says 20260315121500 with no timezone, is that Eastern? Central? UTC? You need a per-interface configuration that specifies the lab's timezone. Getting this wrong means a result collected at 12:15 PM Eastern gets stored as 12:15 PM UTC, which is actually 7:15 AM Eastern. Clinicians will see the wrong collection time.
FHIR requires ISO 8601 format with timezone: 2026-03-15T12:15:00-04:00. Your mapper must reliably convert HL7v2 timestamps to this format, applying the correct timezone offset for each lab interface.
6. Specimen Handling
OBR-15 contains the specimen source (e.g., BLOOD^VENOUS). This maps to a FHIR Specimen resource referenced by both ServiceRequest.specimen and DiagnosticReport.specimen. Labs often send specimen information inconsistently: some use OBR-15, others use SPM segments (Specimen), and some include specimen details only in the OBR-13 (Relevant Clinical Information) as free text. Your mapper needs to handle all three patterns.
LOINC: The Lingua Franca of Lab Results
Every mapping discussion eventually comes back to LOINC (Logical Observation Identifiers Names and Codes). LOINC is the standard coding system for laboratory observations, and it is what makes lab data computable across systems.
A LOINC code encodes five axes:
- Component — What is being measured (Hemoglobin)
- Property — The characteristic (Mass concentration)
- Time — Point in time vs. over a period
- System — The specimen type (Blood)
- Scale — Quantitative, ordinal, or nominal
When OBX-3 contains a LOINC code, your FHIR Observation can use system: "http://loinc.org" and any downstream system, a clinical decision support engine, a quality measure calculator, a public health registry, can interpret the result without human translation. When OBX-3 contains a local code, that pipeline breaks.
The practical implication: if you are building a new lab interface, negotiate LOINC coding as a contractual requirement with the lab. If you are dealing with legacy interfaces that send local codes, invest in building a LOINC mapping table and maintain it as the lab adds new tests.
Putting It All Together: A Complete ORU-to-FHIR Pipeline
Here is the processing flow for converting an ORU^R01 message into FHIR resources:
- Parse — Split the HL7v2 message into segments. Validate MSH. Extract PID, OBR, and OBX segments.
- Identify patient — Use PID-3 (MRN) to look up or create the FHIR Patient resource. Handle patient matching carefully; MRN collisions across facilities are real.
- Correlate order — Use ORC-2/ORC-3 to find the existing ServiceRequest. If this is an update (OBR-25 = F after a P), find the existing DiagnosticReport to update.
- Map OBR to DiagnosticReport — Create or update the DiagnosticReport with status from OBR-25, code from OBR-4, dates from OBR-7 and OBR-22.
- Map each OBX to Observation — For each OBX segment, create an Observation with code from OBX-3, value from OBX-5 (typed by OBX-2), units from OBX-6, range from OBX-7, interpretation from OBX-8.
- Bundle and persist — Wrap everything in a FHIR Transaction Bundle and POST to your FHIR server. Use conditional creates to prevent duplicates.
{
"resourceType": "Bundle",
"type": "transaction",
"entry": [
{
"resource": {
"resourceType": "DiagnosticReport",
"id": "cbc-report-001",
"status": "final",
"code": {
"coding": [{"system": "http://loinc.org", "code": "58410-2"}]
},
"result": [
{"reference": "Observation/wbc-001"},
{"reference": "Observation/rbc-001"},
{"reference": "Observation/hgb-001"}
]
},
"request": {
"method": "PUT",
"url": "DiagnosticReport?identifier=LAB_ACC_001"
}
},
{
"resource": {
"resourceType": "Observation",
"id": "wbc-001",
"status": "final",
"code": {
"coding": [{"system": "http://loinc.org", "code": "6690-2"}]
},
"valueQuantity": {"value": 7.2, "unit": "10*3/uL"}
},
"request": {
"method": "PUT",
"url": "Observation?identifier=LAB_ACC_001-OBX1"
}
}
]
}How Nirmitee Approaches Lab Integration
At Nirmitee, lab integration is a core part of our EHR platform work. Our approach is straightforward: we build configurable HL7v2 parsing pipelines that normalize vendor-specific message variations before the FHIR mapping layer sees them. Each lab interface gets a configuration profile that defines its OBX ordering behavior, coding system preferences, timezone, and abnormal flag vocabulary. The FHIR mapping layer itself stays clean and standard-compliant because the normalization layer absorbs the vendor chaos.
We maintain LOINC mapping tables for the major reference labs and update them quarterly. For new interfaces, our onboarding process includes a message analysis phase where we process sample ORU messages from the lab to identify deviations from expected patterns before writing any mapping code. This front-loaded analysis catches ninety percent of production issues before they become production issues.
Key Takeaways
- Lab integration is hard not because the standards are bad, but because adherence varies wildly across vendors. Budget time for per-vendor mapping.
- ORM maps to ServiceRequest + Task. ORU maps to DiagnosticReport + Observation. OBR is the bridge between the order and the report.
- OBX-2 (value type) determines everything about how you parse OBX-5. Build your parser to handle all types, not just NM and ST.
- LOINC in OBX-3 is non-negotiable for interoperability. If the lab sends local codes, build a mapping table.
- Preliminary-to-final result updates require idempotent write logic. Use placer/filler order numbers as correlation keys.
- Timezones, abnormal flags, and panel grouping are the three production issues that every lab interface encounters. Design for them from the start.
Lab integration will never be a "plug and play" exercise. But with solid HL7v2 parsing, disciplined FHIR mapping, and per-vendor configuration, it can be a reliable, maintainable pipeline instead of the fragile point-to-point interface it so often becomes.
Building interoperable healthcare systems is complex. Our Healthcare Interoperability Solutions team has deep experience shipping production integrations. We also offer specialized Healthcare Software Product Development services. Talk to our team to get started.