The choice is not "which is better" — it's "which fits"
RFID is not always better than barcode. Barcode is not always cheaper at year 5. The defensible question for a hospital evaluating asset tracking technology is: at what scale and audit cadence does each earn its keep?
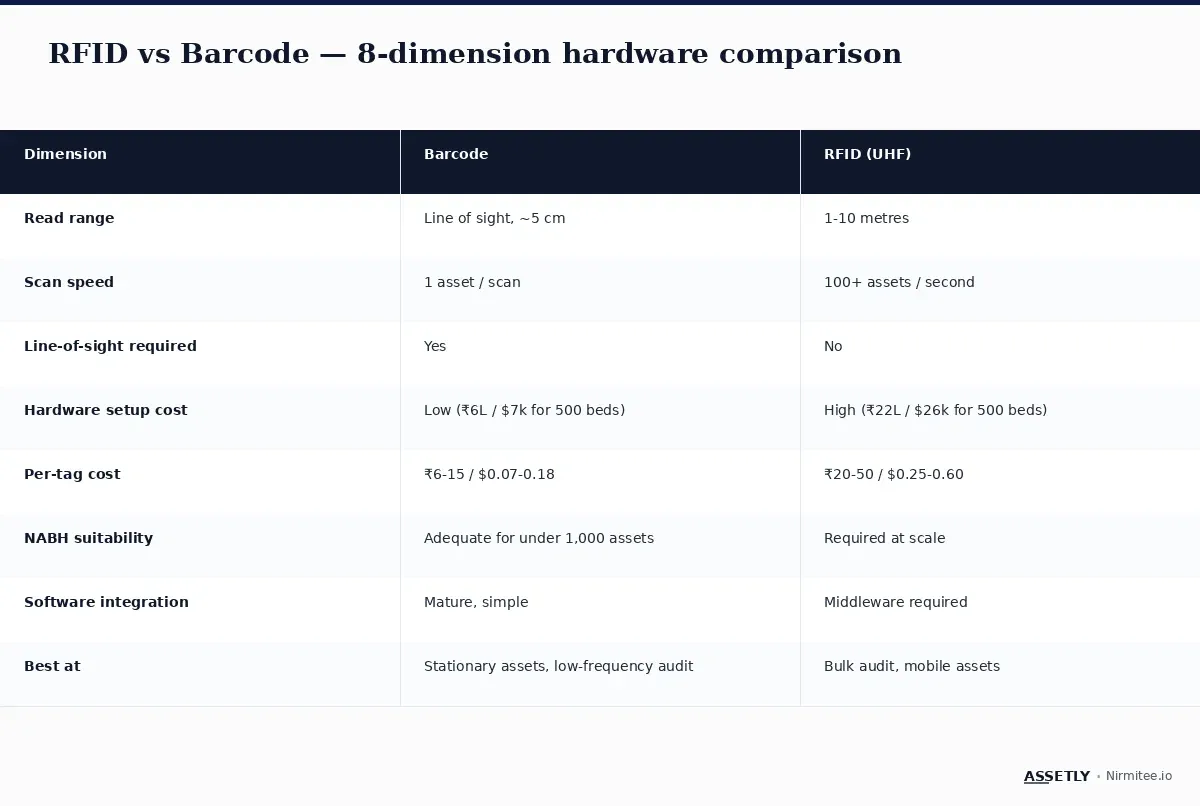
This guide compares barcode and RFID on 8 hardware-level dimensions, then offers a decision rule based on asset count and audit frequency.
Dimension 1: Read range
Barcode requires line-of-sight at very short range — typically 5 centimetres. The scanner must see the printed code. RFID (UHF) reads at 1-10 metres without line-of-sight; the tag and reader can be separated by walls, equipment, or fabric. This is the single biggest operational difference.
Dimension 2: Scan speed
Barcode is sequential — one asset per scan. A biomedical staff member auditing 500 assets manually scans 500 times. RFID is parallel — a portal reader can scan 100+ tags per second as a cart of equipment passes through. For a 5,000-asset hospital running monthly audits, this is a 50-100× time-saving.
Dimension 3: Line-of-sight requirement
Barcode fails when the label is dirty, scratched, partially covered, or facing the wrong way. Real-world barcode scan accuracy in production hospitals is typically 92-97%. RFID has no line-of-sight requirement; even a tag inside a metal-walled cart can be read from outside (with on-metal tag variants).
Dimension 4: Hardware setup cost
For a 500-bed hospital: barcode-only setup runs ₹6 lakh ($7,400) in year 1 (printer + labels + software). Hybrid barcode + UHF RFID runs ₹21-22 lakh ($26,000) — roughly 3.5× more, driven by RFID readers, antennas, and tag cost.
Dimension 5: Per-tag cost
Barcode labels: ₹6-15 ($0.07-0.18) per polyester label. UHF RFID tags: ₹20-50 ($0.25-0.60) per tag — 2-4× the cost. At scale (5,000+ assets), tag cost becomes a meaningful budget line.
Dimension 6: NABH / Joint Commission suitability
Both technologies satisfy NABH HCO 5th Ed and Joint Commission EC.02.04 standards as long as the asset register is reconcilable to physical inventory. The difference is operational: barcode programs achieve reconciliation through manual audits; RFID programs achieve it through automated portal reads. For hospitals above 2,000 assets, RFID is the only practical way to maintain monthly audit cadence.
Dimension 7: Software integration complexity
Barcode integrates with asset management software through standard scanner input — keystrokes or USB / Bluetooth scanner events. Mature, simple. RFID requires middleware to translate reader events into asset records — Assetly and most modern platforms include this middleware out of the box, but legacy systems may require custom integration work.
Dimension 8: Best-fit operational profile
Barcode is right for stationary assets with annual or semi-annual audit cadence. RFID is right for mobile assets, bulk-read zones, and monthly or daily audit cadence.
The decision rule

The defensible decision rule:
- Under 1,000 assets, annual audit: Barcode-only. Don't over-engineer.
- 1,000-2,000 assets, semi-annual audit: Barcode-only, plan for hybrid in year 2-3.
- Above 2,000 assets or monthly audit: Hybrid barcode + UHF RFID — barcode for stationary, RFID for mobile and bulk-read zones.
- Real-time ICU location requirement: Add BLE on top of barcode + UHF RFID.
Real-world: a hospital that started barcode and added RFID at year 2
A 450-bed hospital in Bangalore launched in 2024 with barcode-only across 1,800 biomedical assets. Manual quarterly audits ran reliably for 18 months. By the second year, growth pushed the asset count past 2,400 — manual audits began consuming 200+ staff-hours per quarter. The hospital added a UHF RFID layer in 2026 — Zebra ZT411 with RFID encoder, 8 portal readers at zone exits, 1,200 RFID smart labels on mobile and OT assets. Barcode remained on stationary equipment. The result: monthly audit cadence with under 30 staff-hours per audit. Total addition was ₹14 lakh ($17,000), payback in 11 months on staff time alone.
Key takeaways
- RFID is not always better than barcode. The fit is workflow- and scale-driven.
- Below 1,000 assets and annual audit — barcode-only is the right answer.
- Above 2,000 assets or monthly audit — hybrid barcode + UHF RFID earns its premium.
- RFID hardware setup is roughly 3-4× barcode for a 500-bed hospital.
- Most large hospitals end up hybrid: barcode on stationary, RFID on mobile and bulk-read zones, BLE on ICU mobile.
Choosing barcode, RFID or hybrid for your hospital?
Read our pillar guide on healthcare asset management, or talk to the Assetly team for a barcode vs RFID decision review for your hospital's asset profile.