The wrong printer is the most expensive cheap purchase a hospital makes
Most hospitals don't think of asset label printers as a strategic decision. They are. The printer determines whether your asset labels survive the next autoclave cycle or are unreadable in 12 months. It determines whether you can encode RFID tags during printing or have to retrofit. It determines whether your biomedical team prints labels at the speed of commissioning, or in fits and starts.
This primer walks through the four printer technologies hospitals deploy for asset labelling — and where each fits.
Direct Thermal (DT) printers
Direct thermal printers don't use ink or ribbons. They print by selectively heating a chemically-treated paper that turns black where heat is applied. The label has no protective layer, which means heat, light, and chemicals all degrade the print over time.
Strengths: very low cost per label, no consumables besides label stock, fast print speed, compact form factor.
Weaknesses: labels fade in 6-18 months under hospital cleaning chemicals (IPA, chlorhexidine) and direct light. They are not suitable for biomedical equipment that lives 5+ years.
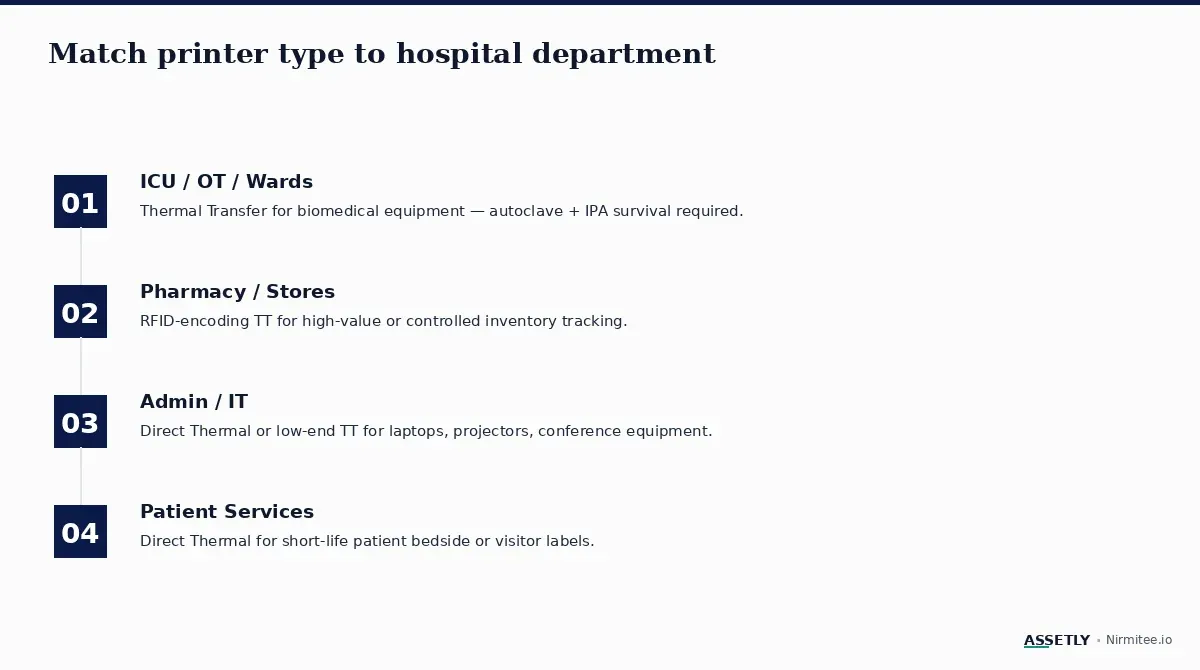
Where DT belongs in a hospital: patient bedside short-life labels, in-transit consumable tracking, admin assets like laptops or projectors with 2-3 year lifecycles, and any high-volume short-duration application.
Thermal Transfer (TT) printers
Thermal transfer printers use a wax, resin, or wax-resin ribbon. The print head melts the ribbon onto the label, transferring durable ink. Printed labels can survive autoclave cycles, isopropyl alcohol cleaning, chlorhexidine wipes, and 5-7 years of bedside wear when paired with the right label stock (polyester).
Strengths: long label life, chemical resistance, durability against abrasion, compatible with polyester and other hospital-grade label materials.
Weaknesses: higher cost per label (label + ribbon), slightly slower than DT, requires ribbon inventory management.
Where TT belongs in a hospital: ventilators, monitors, infusion pumps, OT instrument trays, biomedical equipment of any kind, and anywhere a label needs to survive longer than 18 months.
RFID-encoding thermal transfer printers
RFID printers are TT printers with an additional encoding head that writes data to UHF Class 1 Gen 2 RFID inlays embedded in the label stock. The printer prints the human-readable barcode and encodes the RFID chip in a single pass.
Strengths: single-pass label + tag production, no separate encoding step, supports asset programs that scale to 2,000+ items.
Weaknesses: highest cost in the printer family, requires RFID-compatible label stock, RFID inlay verification adds calibration steps.
Where RFID printers belong: hospitals running 2,000+ asset RFID programs, OT instrument tray tracking, central stores with high inventory turnover, and any workflow where assets are scanned in bulk (portal readers).
Inkjet printers
Inkjet printers are common in offices and have minimal role in hospital asset management. The output is not chemical-resistant or autoclave-safe. Label adhesion is unreliable on industrial label stocks. They are inexpensive but unsuitable for biomedical labelling.
Where inkjet belongs: low-volume admin labelling — visitor passes, conference room signage, internal mail labels — not asset tracking.
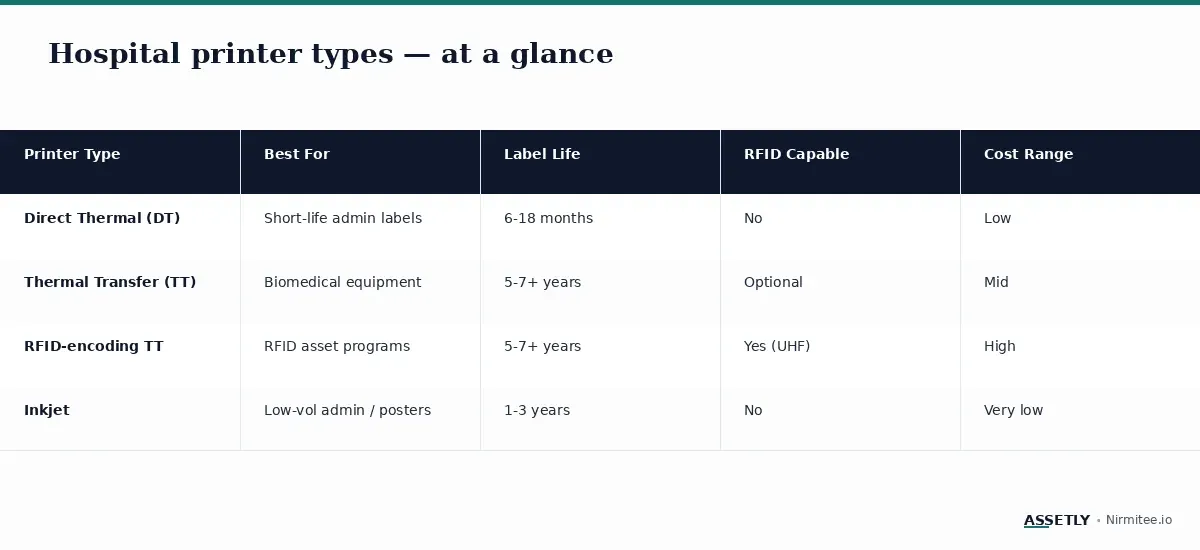
Decision matrix: which printer for which hospital scenario
Real-world: a printer-mismatch cautionary tale
A 250-bed hospital in Chennai standardised on direct thermal printers in 2023, citing the low cost. Within 14 months, biomedical staff reported 23% of labels were illegible — they had faded under repeated alcohol cleaning. Re-labelling consumed 180 staff-hours and the asset register lost integrity for the period.
The hospital re-tendered for thermal transfer printers (Zebra ZD421 + Z-Ultimate label stock) at roughly 2.4× the per-label cost. After 18 months on the new stack, label survival was 99.6%. The total cost-of-ownership at year 3 was lower with TT than DT, once re-labelling and audit gap costs were factored in.
Key takeaways
- Direct thermal is right for short-life admin labels and patient bedside use. Wrong for biomedical.
- Thermal transfer is the standard for any biomedical equipment with a 5+ year lifecycle.
- RFID-encoding TT printers are essential for asset programs above 2,000 assets or with daily audit cadence.
- Inkjet has minimal role in hospital asset labelling.
- Cheapest per-label cost is usually most expensive at year 3 once you include re-labelling and audit gaps.
Choosing your hospital's printer stack?
The right printer is one of three decisions — printer + label + software — that determine whether your asset program scales. Read our pillar guide or talk to the Assetly team for a printer specification review.