Part of our complete guide to Agentic AI for Revenue Cycle Management: The Race to a Touchless Revenue Cycle.
If you are building software that touches the US healthcare revenue cycle, you will inevitably need to integrate with payers. Whether your product handles patient registration, billing, claims management, or care coordination, the ability to verify eligibility, submit claims, and process remittance data is foundational infrastructure, not an optional feature.
To see these integrations composed into a product, read our case study on the claims intelligence platform with a clearinghouse FHIR pipeline.
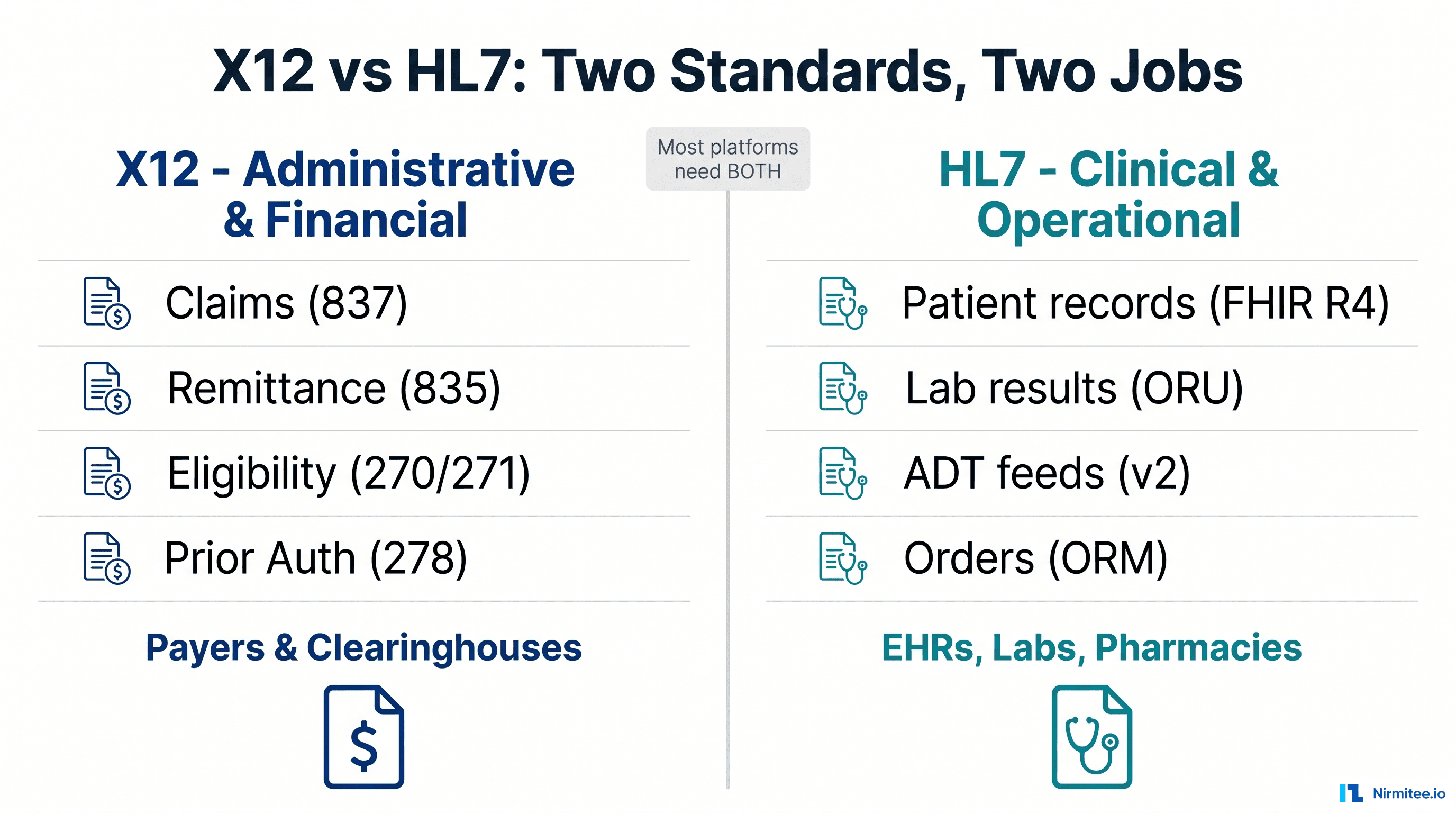
The US payer integration landscape is simultaneously one of the most standardized and most frustrating domains in healthtech. HIPAA mandates specific electronic transaction formats, but every payer interprets those standards differently. CMS is pushing FHIR-based APIs as the future, but X12 EDI transactions still carry over 95% of production payer traffic today. Understanding both worlds, and knowing when to use which, is essential for any healthcare developer.
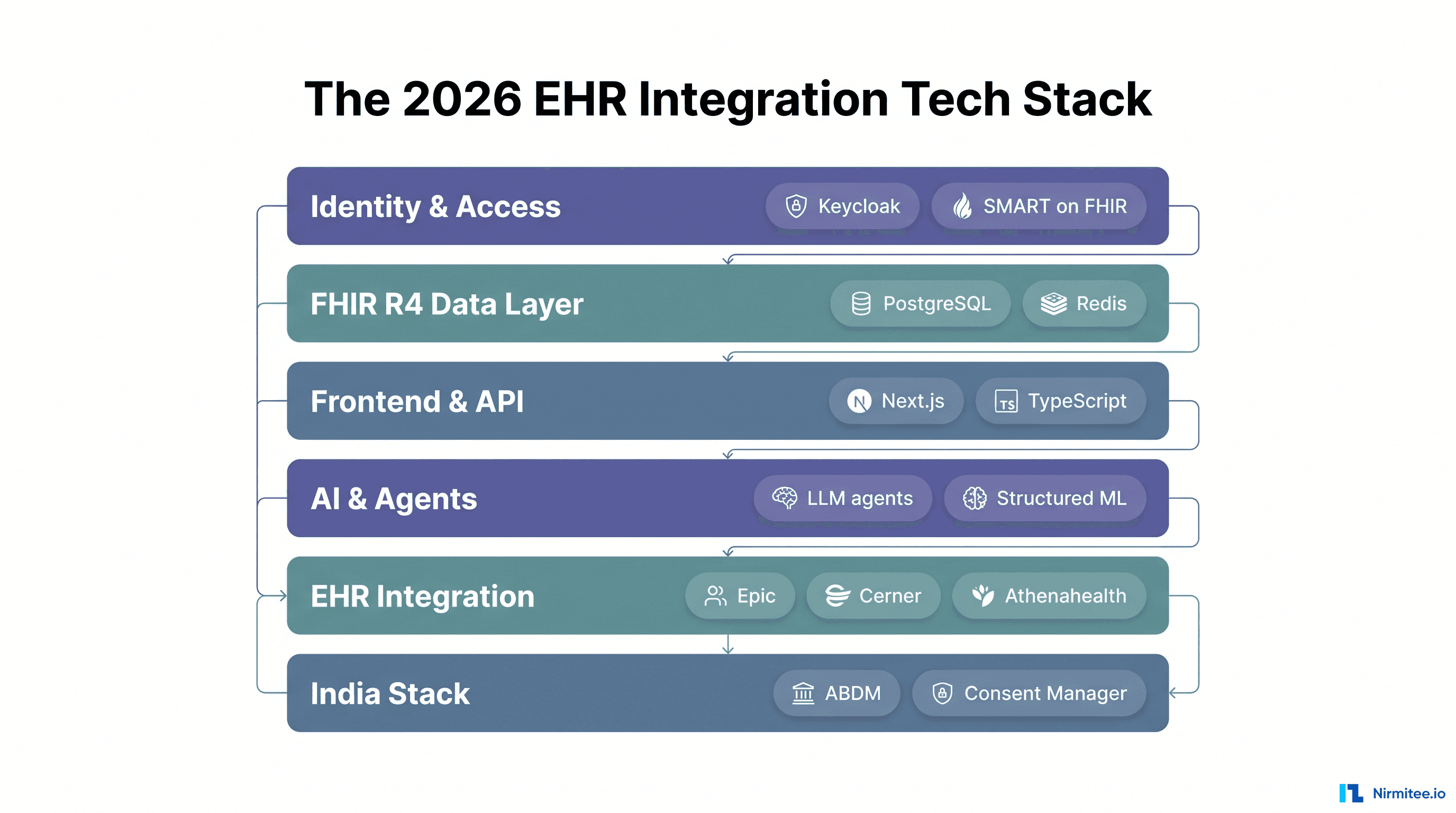
This guide covers the complete payer integration stack. We map the ecosystem of payers you will connect to, the X12 EDI transactions that power eligibility verification, claims, and remittance processing, and the clearinghouse integration patterns that make it practical. The emerging FHIR-based payer APIs mandated by CMS. We will go deep enough that you can architect a payer integration module, evaluate clearinghouse vendors, and avoid the common failures that delay production launches.
The US Payer Ecosystem: Who You Are Integrating With
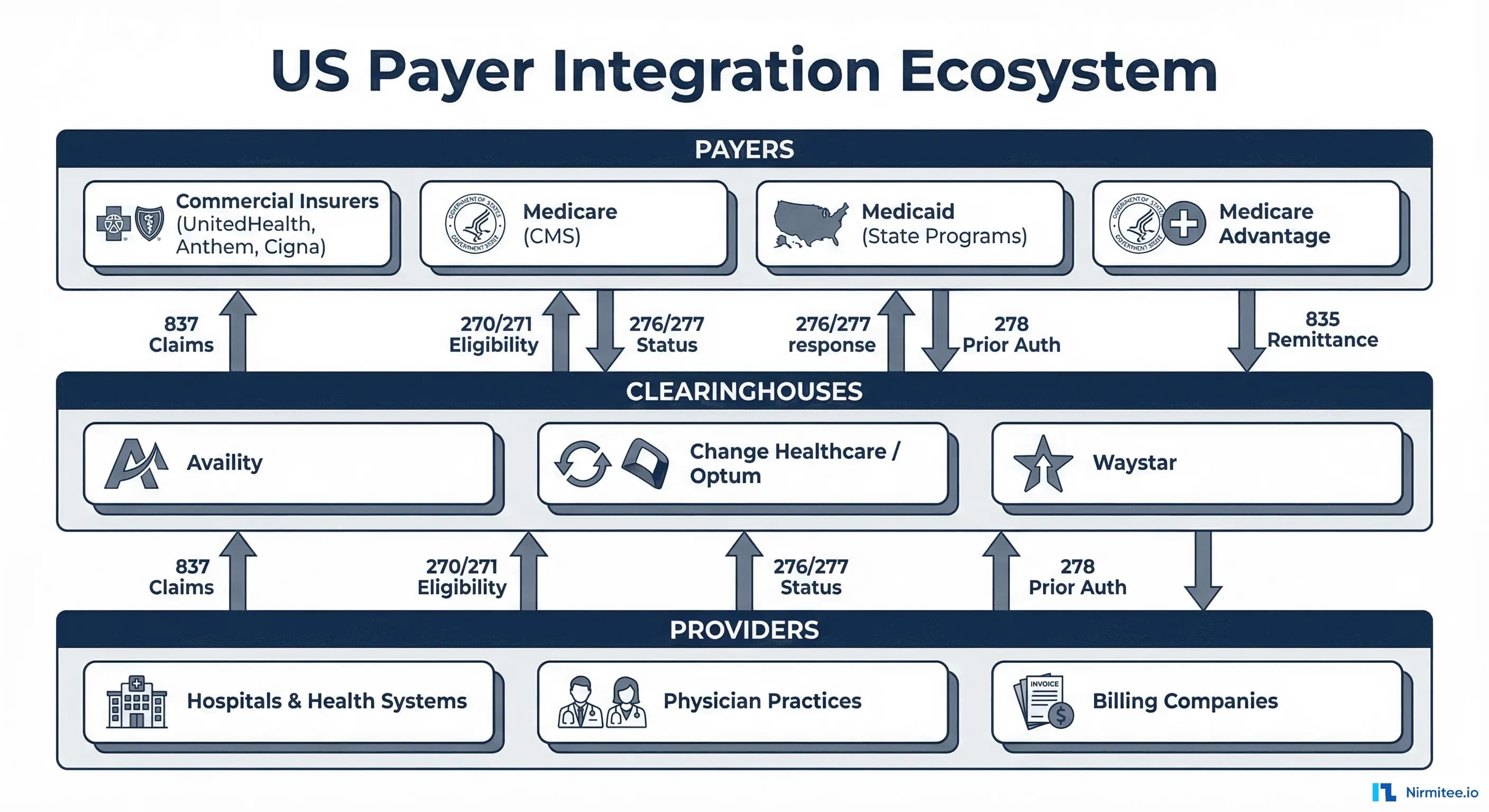
Before writing a single line of integration code, you need to understand who sits on the other side of every transaction. The US healthcare payer landscape has three primary categories, each with distinct integration characteristics.
Commercial Payers
Commercial health insurers cover about 177 million Americans through employer-sponsored plans, individual marketplace plans, and group policies. The five largest, UnitedHealthcare, Elevance Health (Anthem), CVS Health (Aetna), Cigna, and Humana, account for roughly 45% of the commercially insured population. But the long tail matters: there are over 900 commercial payers in the US, each with their own enrollment processes, companion guides, and adjudication rules.
For developers, the key challenge with commercial payers is fragmentation. The same insurer may have different Payer IDs for different products (commercial PPO vs. HMO vs. Medicare Advantage), different states, or different transaction types. UnitedHealthcare alone has dozens of Payer IDs depending on the plan and geography. Your payer routing logic needs to handle this complexity.
Medicare
Medicare covers 67 million beneficiaries, primarily adults over 65 and individuals with specific disabilities. Medicare claims are processed through Medicare Administrative Contractors (MACs), regional entities that adjudicate claims on behalf of CMS. There are currently 12 MACs covering different geographic jurisdictions. Part A (hospital) and Part B (physician) claims route to different MAC processing systems.
Related Reading
For more insights, explore our guides on AI Medicare Claims Processing: MACs, Appeals & Compliance and FHIR in Modern Healthcare.
You may also find value in EHR Software Development Guide and Building a Healthtech App.
Medicare is often the easiest payer to integrate with from a standards perspective, CMS enforces X12 compliance strictly, and the companion guides are well-documented. However, Medicare Advantage (Part C) plans are administered by commercial insurers, so they follow commercial payer integration patterns, not traditional Medicare.
Medicaid
Medicaid covers about 93 million individuals across 56 programs (50 states plus DC and territories). Each state administers its own Medicaid program with distinct rules, formularies, and integration requirements. Many states contract with managed care organizations (MCOs) to administer Medicaid benefits. That means your integration may route through a commercial payer's system rather than the state Medicaid agency directly.
Medicaid integration is the most variable. Some states have modern electronic claims submission portals, while others still rely on legacy systems with limited EDI support. If your application serves providers in multiple states, plan for state-by-state testing and enrollment.
X12 EDI Transactions: The Language of Payer Communication
The Health Insurance Portability and Accountability Act (HIPAA) mandates the use of ASC X12 standard electronic transactions for administrative healthcare data exchange. If you have never encountered X12 before, prepare for a format that predates the web, JSON, and XML. X12 transactions use delimited segments with positional elements, and the learning curve is steep. But mastering these transaction types is non-negotiable for payer integration.
270/271: Eligibility Verification
The 270 Health Care Eligibility Benefit Inquiry and 271 Health Care Eligibility Benefit Response are the most frequently executed payer transactions in healthcare. Every patient visit should trigger an eligibility check to verify active coverage, confirm benefit details, identify copay and deductible amounts, and determine whether prior authorization is required for planned services.
The 270 request requires minimal data: subscriber or member identification, the provider's NPI, and the date of service. Optionally, add a service type code indicating what category of benefits you are inquiring about (e.g., health benefit plan coverage, mental health, chiropractic). The 271 response returns a rich data set including:
- Coverage status: Active, inactive, or pending
- Benefit details: In-network vs. out-of-network, copay amounts, coinsurance percentages, deductible remaining
- Plan information: Group number, plan name, coverage dates
- Service-specific rules: Visit limits, prior authorization requirements, referral requirements
A typical 270/271 exchange looks like this in raw X12 format:
ISA*00* *00* *ZZ*SENDER_ID *ZZ*RECEIVER_ID *260319*1200*^*00501*000000001*0*T*:~
GS*HS*SENDER_CODE*RECEIVER_CODE*20260319*1200*1*X*005010X279A1~
ST*270*0001*005010X279A1~
BHT*0022*13*REF_NO_001*20260319*1200~
HL*1**20*1~
NM1*PR*2*UNITED HEALTHCARE*****PI*87726~
HL*2*1*21*1~
NM1*1P*1*SMITH*JOHN****XX*1234567890~
HL*3*2*22*0~
NM1*IL*1*DOE*JANE****MI*ABC123456~
DMG*D8*19850215*F~
DTP*291*D8*20260319~
EQ*30~
SE*13*0001~
GE*1*1~
IEA*1*000000001~The delimiters (* for element, ~ for segment, : for component) are defined in the ISA header. Each segment has a specific meaning: NM1*PR identifies the payer, NM1*1P identifies the provider, NM1*IL identifies the insured member, and EQ*30 requests health benefit plan coverage information.
837P and 837I: Claims Submission
The 837 Health Care Claim is the electronic equivalent of submitting a bill to the insurance company. The 837P (Professional) covers claims from individual providers and maps to the CMS-1500 form. The 837I (Institutional) covers facility claims and maps to the UB-04 form.
An 837 claim contains everything the payer needs for adjudication:
- Patient demographics: Name, date of birth, gender, address
- Subscriber information: Member ID, group number, relationship to patient
- Provider identifiers: Billing provider NPI, rendering provider NPI, service facility location
- Diagnosis codes: ICD-10-CM codes (required, up to 12 per claim)
- Procedure codes: CPT/HCPCS codes with modifiers, units, and charges
- Service dates: Date of service for each line item
- Prior authorization numbers: When applicable
- Coordination of benefits: Primary payer adjudication data when billing secondary
Claims can be submitted individually or in batches. Most clearinghouses accept batch files containing hundreds of claims in a single 837 transaction, which is the standard production pattern for billing systems processing high volumes.
835: Electronic Remittance Advice (ERA)
The 835 Health Care Claim Payment/Advice is the payer's response to a claim, explaining what was paid, what was denied, and why. The 835 is the electronic equivalent of the Explanation of Benefits (EOB) you receive as a patient, but structured for machine processing.
Each 835 transaction contains claim-level and line-level adjudication details:
- Payment amount: What the payer is paying for each service line
- Adjustment reason codes (CARCs): Standardized codes explaining why a charge was adjusted (e.g., CO-45 means "charges exceed the fee schedule")
- Remark codes (RARCs): Additional explanation codes providing context for adjustments
- Patient responsibility: Copay, coinsurance, and deductible amounts the patient owes
- Check/EFT information: Payment method and reference numbers
Parsing 835 files is one of the most complex tasks in payer integration. A single 835 file may contain payment information for hundreds of claims, and the adjustment logic requires mapping CARC/RARC codes to human-readable denial reasons. Automating 835 processing is where agentic AI for revenue cycle management delivers significant value.
276/277: Claim Status
The 276 Health Care Claim Status Request and 277 Health Care Claim Status Response allow providers to check on submitted claims. The 277 response returns a status category code (accepted, rejected, finalized, etc.) and status codes indicating the specific disposition. These transactions are useful for building claim tracking dashboards but are less commonly used in real-time workflows since payers also communicate status through clearinghouse portals.
278: Prior Authorization
The 278 Health Care Services Review transaction handles prior authorization requests and responses. The provider submits clinical justification for a planned service, and the payer responds with approval, denial, or a request for additional information. While the X12 278 transaction exists, adoption has been inconsistent. Many payers still require prior auth through their proprietary web portals, phone calls, or fax. The CMS-0057-F final rule is changing this by mandating FHIR-based prior authorization APIs by January 2027.
Real-Time Eligibility Verification: API Patterns and Platforms
While X12 270/271 transactions are the underlying standard, most healthcare applications do not build raw X12 parsers from scratch. Instead, they integrate with clearinghouses that provide modern API layers on top of the X12 infrastructure.
Availity
Availity is the largest health information network in the US, connecting to over 5,000 payers. Their real-time eligibility API accepts structured JSON requests and translates them to X12 270 transactions, routing to the appropriate payer and returning parsed 271 responses. Key developer features include:
- RESTful API with JSON payloads (no raw X12 handling required)
- Batch eligibility for high-volume verification
- Multi-payer connectivity through a single integration
- Sandbox environment for testing with simulated payer responses
- Webhook notifications for asynchronous transaction completion
Availity's developer portal (developer.availity.com) provides complete API documentation, Postman collections, and test credentials. Integration typically takes 4-6 weeks from API key provisioning to production go-live.
Change Healthcare (Optum)
Now part of Optum (UnitedHealth Group), Change Healthcare operates the Intelligent Healthcare Network, processing over 15 billion transactions annually. Their eligibility API supports real-time and batch modes, with enhanced features like:
- Predicted eligibility when a payer is temporarily unavailable
- Benefits parsing that normalizes payer-specific response formats
- Cost estimation combining eligibility data with contracted rates
- Direct connectivity to UnitedHealthcare systems (parent company advantage)
Change Healthcare's API is particularly strong for organizations that need deep integration with UnitedHealthcare plans, given the parent company relationship.
Waystar
Waystar focuses on revenue cycle intelligence, combining eligibility verification with AI-powered denial prediction. Their platform goes beyond basic 270/271 processing to provide:
- Predictive denial scoring at the point of eligibility check
- Automated prior authorization determination based on eligibility response
- Patient financial responsibility estimation
- Multi-payer claim status aggregation
Waystar's approach is compelling for organizations building revenue cycle management software that needs to combine eligibility data with predictive analytics.
Building Your Eligibility Integration
Regardless of which clearinghouse you choose, the integration pattern is consistent:
// Eligibility verification pseudocode
async function verifyEligibility(patient, provider, serviceDate) {
// Step 1: Build the eligibility request
const request = {
subscriber: {
memberId: patient.insuranceMemberId,
firstName: patient.firstName,
lastName: patient.lastName,
dateOfBirth: patient.dob,
gender: patient.gender
},
provider: {
npi: provider.npi,
taxonomyCode: provider.taxonomy
},
payer: {
payerId: patient.payerId // Clearinghouse-specific
},
encounter: {
dateOfService: serviceDate,
serviceTypeCodes: ['30'] // Health benefit plan coverage
}
};
// Step 2: Submit to clearinghouse
const response = await clearinghouse.eligibility.verify(request);
// Step 3: Parse and normalize response
return {
isActive: response.coverageStatus === 'ACTIVE',
copay: response.benefits.copay?.amount,
deductibleRemaining: response.benefits.deductible?.remaining,
coinsurance: response.benefits.coinsurance?.percentage,
priorAuthRequired: response.benefits.priorAuthRequired,
planName: response.planInformation?.name,
effectiveDate: response.planInformation?.effectiveDate,
terminationDate: response.planInformation?.terminationDate
};
}The response normalization step is critical. Every payer returns 271 data slightly differently, and clearinghouses handle varying degrees of this normalization. Budget time for payer-specific response parsing logic, especially for benefit details where data formats vary widely.
Claims Submission Workflow: End-to-End
Claims submission is the financial backbone of healthcare provider operations. A clean, automated claims workflow directly impacts days in accounts receivable, denial rates, and ultimately revenue. Here is the end-to-end process from service delivery to payment posting.
Step 1: Claim Generation
After a patient encounter, the billing system generates a claim from the encounter data. This requires mapping clinical documentation to billing codes:
- Diagnosis coding: Map provider documentation to ICD-10-CM codes. The primary diagnosis must support medical necessity for the billed services.
- Procedure coding: Map services rendered to CPT (Current Procedural Terminology) or HCPCS (Healthcare Common Procedure Coding System) codes with appropriate modifiers.
- Charge capture: Apply the provider's fee schedule to generate line-item charges.
- Supporting data: Attach prior authorization numbers, referring provider information, and accident/onset dates when applicable.
Step 2: Claim Scrubbing
Before submission, claims must pass through edit checks that catch errors before they reach the payer. Effective claim scrubbing reduces denial rates by 20-30%:
- NPI validation: Verify billing and rendering provider NPIs are active in NPPES
- Code validation: Check ICD-10 and CPT codes for validity, gender/age consistency, and code-to-code compatibility
- Payer-specific edits: Apply rules from the payer's companion guide (e.g., specific modifier requirements, bundling rules)
- Timely filing checks: Verify the claim is within the payer's filing deadline (typically 90-365 days from date of service)
- Duplicate detection: Prevent resubmission of already-adjudicated claims
Step 3: Clearinghouse Submission
The scrubbed claim is formatted as an X12 837P or 837I transaction and submitted to the clearinghouse. The clearinghouse performs additional format validation, resolves the Payer ID to the correct payer endpoint, and routes the claim. Most clearinghouses return an acknowledgment (999 transaction) within minutes confirming the claim was accepted for processing or rejected for format errors.
Step 4: Payer Adjudication
The payer's adjudication engine processes the claim through multiple validation stages. It checks member eligibility at date of service, benefit plan coverage for the billed services, and medical policy rules. Then it applies contracted rates and handles coordination of benefits with other payers. Adjudication typically takes 14-30 days for clean claims, though some payers process within 5-7 days.
Step 5: ERA/EOB Processing
The payer generates an 835 ERA file with the adjudication results. Your system must parse this file, match payment/denial information to the original claim, post payments to patient accounts, identify and categorize denials for follow-up, and calculate patient responsibility balances. This is where robust healthcare integration platform selection matters, as the volume and complexity of 835 processing scales with your provider base.
Step 6: Denial Management
Denied claims require investigation, correction, and resubmission or appeal. The most common denial reasons developers need to handle programmatically are:
- CO-4: The procedure code is inconsistent with the modifier or a required modifier is missing
- CO-16: Claim lacks information or has submission errors
- CO-29: The time limit for filing has expired
- CO-45: Charges exceed the fee schedule or maximum allowable amount
- CO-50: Non-covered service (not a benefit under the plan)
- CO-197: Prior authorization or precertification was not obtained
Clearinghouse Integration Patterns
For production healthcare applications, a clearinghouse is the standard integration pattern. Direct payer connectivity is impractical for most applications, the enrollment, testing, and maintenance overhead for even a single payer relationship is substantial. You would need to repeat it for every payer your providers bill.
API-First Integration
Modern clearinghouses provide RESTful APIs that abstract the X12 complexity. Your application sends JSON requests for eligibility checks, claim submissions, and status inquiries. The clearinghouse handles X12 translation, payer routing, and response parsing. This is the recommended pattern for new applications.
// Example: Clearinghouse API claim submission
POST /api/v1/claims
Content-Type: application/json
Authorization: Bearer {api_token}
{
"claimType": "professional",
"billingProvider": {
"npi": "1234567890",
"taxId": "12-3456789",
"name": "Dr. Jane Smith",
"address": { ... }
},
"subscriber": {
"memberId": "ABC123456",
"payerId": "87726",
"relationship": "self"
},
"patient": { ... },
"diagnoses": [
{ "code": "M54.5", "qualifier": "ABK", "order": 1 }
],
"serviceLines": [
{
"procedureCode": "99213",
"modifiers": [],
"chargeAmount": 150.00,
"units": 1,
"dateOfService": "2026-03-19",
"placeOfService": "11"
}
]
}SFTP Batch Integration
For high-volume operations (large hospital billing departments, billing companies), SFTP-based batch processing remains common. Your system generates X12 837 files, drops them in an SFTP directory, and the clearinghouse picks them up on a scheduled basis. Response files (999 acknowledgments, 835 ERAs, 277 claim status) are deposited back for your system to process. This pattern handles millions of claims efficiently but introduces latency.
Hybrid Architecture
Many production systems use a hybrid approach: real-time APIs for eligibility verification and claim status (where immediate response matters) and SFTP batch processing for claims submission and ERA retrieval (where volume efficiency matters). This balances user experience with throughput.
FHIR-Based Payer APIs: The Regulatory Future
While X12 EDI carries the vast majority of payer transactions today, the regulatory trajectory is clear: CMS is mandating FHIR-based APIs for payer data exchange. Understanding these requirements is essential for developers building systems that need to remain compliant through 2027 and beyond.
CMS Patient Access API
Mandated since July 2021 and expanded under CMS-0057-F, the Patient Access API requires payers to make claims, encounter, and clinical data available to members through a FHIR R4 API. This uses the CARIN Blue Button framework (HL7 C4BB IG) for claims data and US Core profiles for clinical data. As a developer, if you are building a patient-facing application, you can connect to payer Patient Access APIs to retrieve:
- ExplanationOfBenefit resources (claims history)
- Coverage resources (insurance plan details)
- Patient demographics
- Clinical data the payer has received from providers
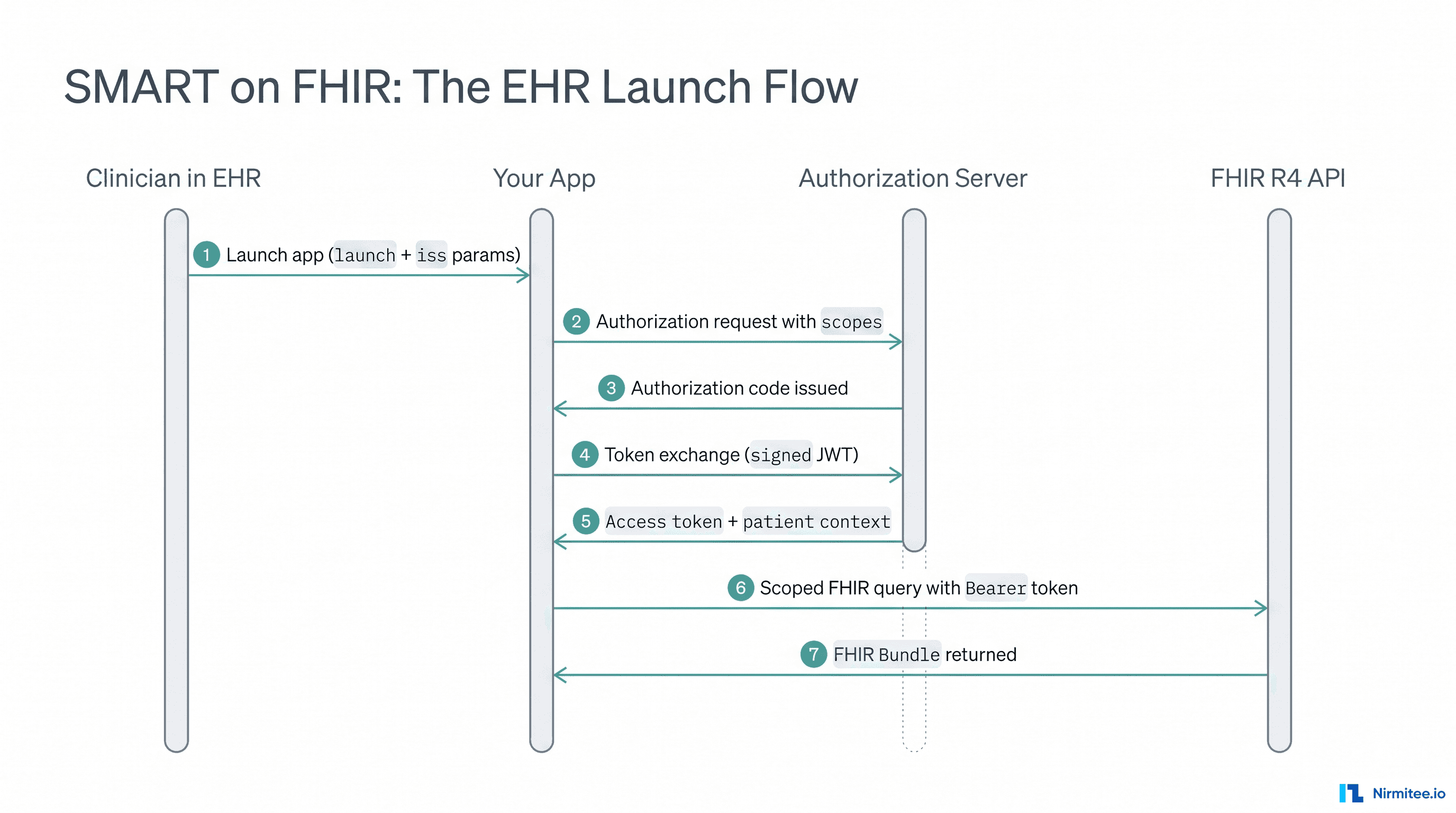
Authentication uses SMART on FHIR (OAuth 2.0) with patient-directed authorization. The patient grants your application access to their payer data through a standard OAuth flow.
Provider Access API
Effective January 1, 2027, payers must offer a Provider Access API enabling in-network providers to retrieve data about their attributed patients. This is significant for care coordination use cases: a primary care provider could query a patient's health plan to see specialist visits, medications dispensed, and hospital admissions recorded by the payer. The API uses Da Vinci PDex profiles and supports bulk FHIR operations for retrieving data about multiple patients.
Payer-to-Payer API
When a patient switches health plans, the new payer must be able to retrieve the patient's historical data from the previous payer (with patient consent). This API enables continuity of care during coverage transitions and reduces redundant testing and procedures. Implementation uses the Da Vinci PDex Payer-to-Payer exchange patterns with bulk FHIR for efficient data transfer.
Prior Authorization API
Perhaps the most impactful requirement, by January 2027 payers must accept prior authorization requests via a FHIR-based API and respond within 72 hours for standard requests and 24 hours for urgent requests. The Da Vinci Prior Authorization Support (PAS) IG defines the FHIR operations for submitting, querying, updating, and canceling prior auth requests. This will fundamentally change prior authorization workflows that currently rely on phone, fax, and proprietary payer portals.
For Developers: Practical FHIR Payer Integration
If you are building a system that needs to consume FHIR payer APIs, here is what to expect:
// FHIR Patient Access API - Retrieve claims history
GET https://payer-fhir.example.com/fhir/ExplanationOfBenefit
?patient=Patient/12345
&_lastUpdated=gt2025-01-01
Accept: application/fhir+json
Authorization: Bearer {smart_access_token}
// Response: Bundle of ExplanationOfBenefit resources
{
"resourceType": "Bundle",
"type": "searchset",
"entry": [
{
"resource": {
"resourceType": "ExplanationOfBenefit",
"status": "active",
"type": {
"coding": [{
"system": "http://terminology.hl7.org/CodeSystem/claim-type",
"code": "professional"
}]
},
"patient": { "reference": "Patient/12345" },
"billablePeriod": {
"start": "2026-02-15",
"end": "2026-02-15"
},
"payment": {
"amount": { "value": 125.00, "currency": "USD" }
}
}
}
]
}The learning curve for FHIR-based payer APIs is greatly lower than X12 EDI, standard JSON over HTTPS, well-documented profiles, and open-source reference implementations. However, payer adoption is still ramping up, and you should expect inconsistencies in implementation quality across payers through 2027. For a complete approach to navigating healthcare interoperability solutions, understanding both the EDI present and FHIR future is essential.
Common Integration Failures and How to Avoid Them
Payer integration has a long list of failure modes that can delay your production launch by weeks or months. Here are the most common issues we see across healthcare development teams.
Wrong Payer ID
The number one cause of claim rejections is routing to the wrong payer. A single insurance company may have 10 or more Payer IDs across different products, states, and transaction types. The patient's insurance card often does not list the correct electronic Payer ID. Solution: use your clearinghouse's payer lookup API to resolve the correct Payer ID from the payer name and plan type. Implement payer ID validation as part of your patient registration workflow.
NPI Issues
Provider NPIs must be active in the NPPES registry, enrolled with the specific payer, and correctly associated with the billing taxonomy code. Common failures include using an individual NPI where an organizational NPI is required (or vice versa). Others: using an NPI that has not completed payer enrollment, and taxonomy code mismatches between NPPES and the payer's provider file.
Timely Filing
Every payer has a claim filing deadline measured from the date of service. Miss it, and the claim is denied with no appeal. Medicare allows 365 days. Most commercial payers allow 90-180 days. Some Medicaid programs allow as few as 60 days. Your system must track filing deadlines by payer and flag claims approaching the limit.
Coordination of Benefits (COB) Errors
When a patient has multiple insurance plans, claims must be submitted to the primary payer first. Only after the primary payer adjudicates can you bill the secondary payer, including the primary's adjudication data in the 837. Getting the primary/secondary determination wrong results in rejections from both payers. Medicare Secondary Payer (MSP) rules add additional complexity when Medicare is involved.
Companion Guide Deviations
While X12 defines the standard, each payer publishes a companion guide specifying their specific requirements within the standard. Some payers require specific loop qualifiers that are optional in the base X12 spec, reject claims with certain modifiers that other payers accept, or have unique requirements for coordination of benefits data. Budget time for reading and implementing companion guide requirements for your top-volume payers.
Testing in Payer Sandboxes
Production payer integration requires rigorous testing across multiple environments. Here is a practical testing strategy:
Phase 1: Format Validation (Week 1-2)
Use your clearinghouse's sandbox to validate X12 format compliance. Submit test 837 claims and 270 eligibility requests, verify that your X12 output passes structural validation (correct segment counts, valid delimiters, required loops present). Most clearinghouses return detailed error reports identifying the exact segment and element with issues.
Phase 2: Payer Test Environments (Week 3-5)
Submit test claims through your clearinghouse to payer-specific test endpoints. These return simulated adjudication results that exercise your 835 parsing logic. Test with multiple scenarios: clean claim payment, partial denial, full denial, patient responsibility, and coordination of benefits.
Phase 3: Production Pilot (Week 6-8)
Submit a small batch of real claims (5-10) with known-good data through production. Verify end-to-end processing including payment posting. Monitor for payer-specific rejections that did not surface in testing. This phase often reveals companion guide requirements that only enforce in production.
Phase 4: Volume Testing (Week 8+)
Gradually increase claim volume while monitoring acceptance rates, rejection patterns, and processing times. Establish baseline metrics for first-pass clean claim rate (target: >95%), average days to payment, and denial rate by category.
Architectural Recommendations for Healthcare Developers
Based on production integration experience across dozens of healthcare applications, here are architectural patterns that scale:
Abstract the Clearinghouse Layer
Design your payer integration as an abstraction layer that can swap clearinghouse vendors without application changes. Define interfaces for eligibility verification, claim submission, claim status, and ERA retrieval. Implement vendor-specific adapters behind these interfaces. This protects you from vendor lock-in and enables multi-clearinghouse strategies for redundancy.
Build a Payer Configuration Database
Maintain a database of payer-specific configuration: Payer IDs per clearinghouse, timely filing deadlines, companion guide rules, enrollment status per provider, and known quirks. This data drives routing decisions, validation rules, and deadline monitoring. Keep it updated, payers change IDs, merge, and update rules regularly.
Implement Idempotent Claim Submission
Claims must be submittable exactly once. Duplicate claims trigger denials and payer audit flags. Use claim-level idempotency keys (combination of patient, provider, date of service, and procedure codes) to prevent accidental resubmission. Maintain a state machine for each claim lifecycle: generated, scrubbed, submitted, acknowledged, adjudicated, posted.
Plan for the FHIR Transition
Even if your current integration is 100% X12 EDI through a clearinghouse, architect your data models to accommodate FHIR resources. Use FHIR resource types (ExplanationOfBenefit, Coverage, Claim) as your internal data models where possible. This reduces the translation effort when FHIR payer APIs become your primary integration path.
What Comes Next
The US payer integration landscape is in a transitional period. X12 EDI remains the production standard and will continue to carry the majority of transactions for years. But the CMS mandates for FHIR-based payer APIs (Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization) are creating a parallel path that will increasingly become the primary integration model.
For healthcare developers starting new projects in 2026, the pragmatic approach is simple. Integrate with a clearinghouse for X12 EDI transactions today (eligibility, claims, remittance), while designing your architecture to support FHIR payer APIs as they mature. The clearinghouses themselves are building FHIR translation layers, so your clearinghouse relationship will likely evolve to support both models.
The complexity is real, but it is manageable with the right architectural patterns, a clear understanding of the transaction types, and a systematic approach to testing. Every claim denied because of a wrong Payer ID, every prior auth delayed because of a missing attachment. Every payment posting error from an 835 parsing bug represents revenue leakage. Getting payer integration right is not just a technical exercise, it is a direct contributor to the financial health of every provider your software serves.
Struggling with healthcare data exchange? Our Healthcare Interoperability Solutions practice helps organizations connect clinical systems at scale. We also offer specialized Healthcare Software Product Development services. Talk to our team to get started.