This blog provides a technical deep-dive into how AI-powered contract management systems detect, quantify, and recover underpayments — with contract modeling techniques, variance detection algorithms, ERA/835 remittance analysis patterns, and integration architecture that goes far beyond the generic overviews published elsewhere.
How Payer Contracts Actually Work: The Complexity That Creates Underpayments
Before we can build systems to detect underpayments, we need to understand what makes payer contracts so difficult to monitor. A typical mid-size hospital manages 20 to 50 payer contracts, each containing thousands of line items with distinct reimbursement logic.
Base Fee Schedules
Every payer contract anchors reimbursement to a fee schedule — a lookup table mapping CPT/HCPCS codes to dollar amounts. The most common structures include:
- Percentage of Medicare: Reimbursement calculated as a multiplier of the CMS Medicare Physician Fee Schedule (MPFS). Example:
110% of Medicarefor E&M codes,95% of Medicarefor radiology. - Flat fee schedules: Fixed dollar amounts per CPT code, typically negotiated annually and stored in contract exhibits.
- DRG-based (inpatient): Payment per diagnosis-related group, often as a percentage of the CMS MS-DRG base rate with facility-specific adjustments.
- Per diem: Fixed daily rate for specific service categories (e.g., $2,800/day for med-surg, $4,500/day for ICU).
- Case rates: Bundled payments for specific procedures (e.g., $35,000 for a total knee replacement including all associated services).
The challenge: a single contract may use all of these payment methodologies simultaneously, with different rules applying to different service categories, places of service, and provider types.
Carve-Outs and Special Provisions
Carve-outs are exceptions to the base fee schedule — specific codes or service categories that are reimbursed at different rates. Common carve-out categories include:
- High-cost drugs: Specialty pharmaceuticals reimbursed at AWP minus a discount percentage (e.g.,
AWP - 15%) rather than the base fee schedule rate. - Implantable devices: Joint implants, cardiac devices, and surgical hardware are often reimbursed at
invoice cost + markup(typically 10-30%). - High-cost procedures: Transplants, NICU days, and complex surgical cases may have individually negotiated case rates or separate stop-loss provisions.
- Observation services: Often reimbursed differently than inpatient stays, with per-hour or per-diem rates distinct from the standard fee schedule.
Stop-Loss and Outlier Provisions
Stop-loss clauses protect both parties from catastrophic costs. They define a cost threshold above which the payer pays a higher rate — typically cost-to-charge ratio applied to charges exceeding the threshold. For hospitals, these clauses are critical for high-acuity cases where actual costs far exceed the DRG or case rate payment.
Rate Escalators
Multi-year contracts should include annual rate escalators of 3-5% to protect against inflation. Without escalators, a 3-year contract effectively delivers a pay cut each year as input costs (labor, supplies, pharmaceuticals) rise. According to the AHA, from 2022 to 2024, general inflation rose by 14.1% while Medicare inpatient payment rates increased by only 5.1% — an effective payment cut of $8.4 billion in lost hospital revenue.
Timely Filing Requirements
Every contract specifies a timely filing window — typically 90 to 365 days from the date of service — within which claims must be submitted. Miss this window, and the payer can deny the claim entirely with no appeal right. Most contracts also define timely filing requirements for appeals (usually 60-90 days from the initial denial).
Why Manual Contract Monitoring Fails at Scale
With each contract containing this level of complexity, manual monitoring becomes a mathematical impossibility. Consider the scale:
- A hospital with 30 payer contracts, each with 1,000+ line items, processes 50,000 to 200,000 claims per month.
- Each claim may have 5-15 service lines, each requiring a separate reimbursement calculation against the correct contract term.
- Payers update fee schedules quarterly, and contracts may contain retroactive rate adjustments that change the expected reimbursement for claims already processed.
- Modifier combinations (
-25,-59,-76,-77) affect reimbursement rates differently across payers — one payer may pay 50% for a-51modifier while another pays 75%.
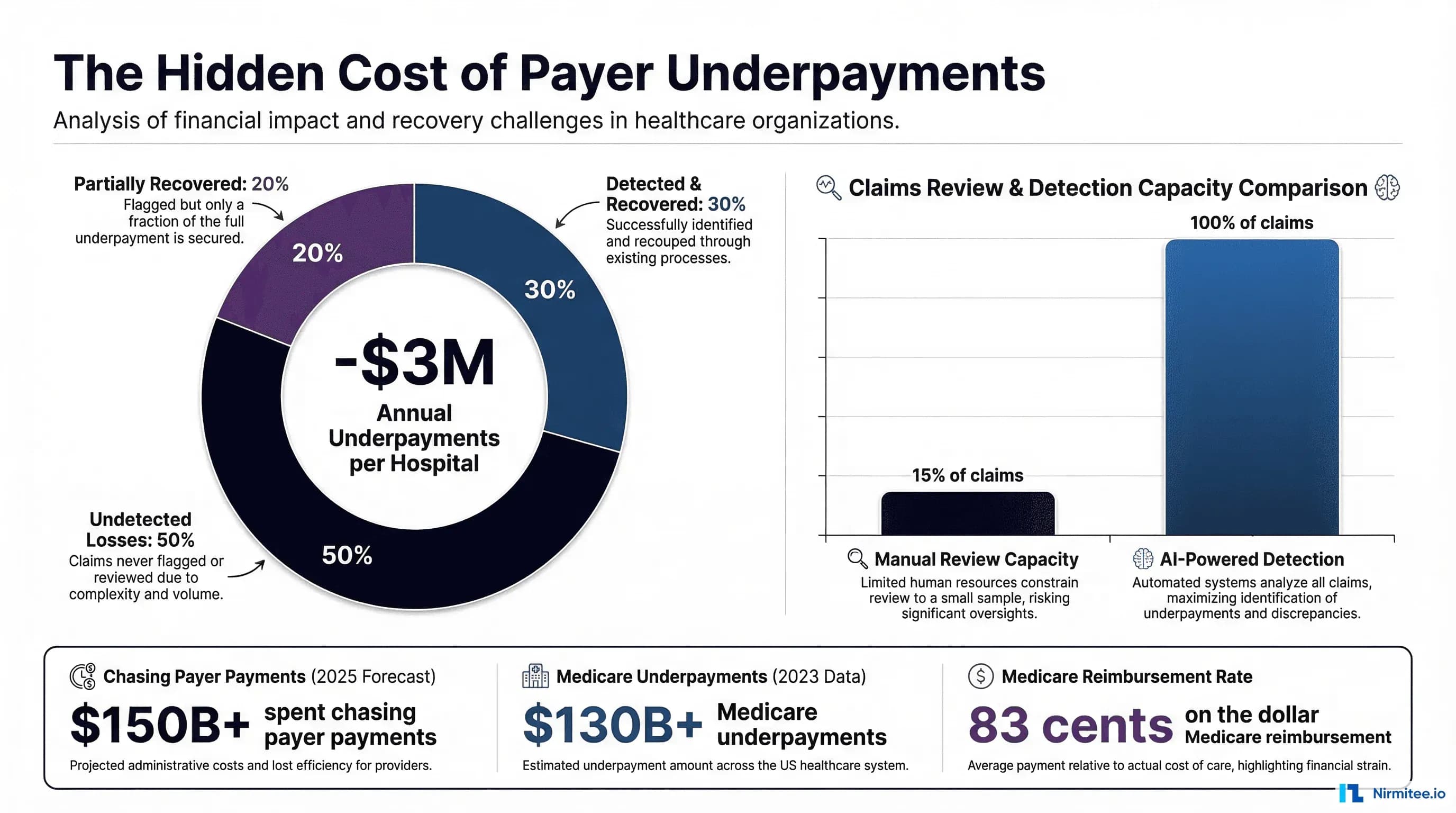
The result: revenue cycle teams typically review only 10-15% of paid claims for underpayment, focusing on high-dollar cases and known problem payers. The remaining 85-90% of claims flow through unexamined, with underpayments silently eroding margins.
A study by MD Clarity found that organizations using manual contract management processes miss an average of 1-3% of net revenue in recoverable underpayments annually. For a $500 million hospital system, that represents $5-15 million in lost revenue — every year.
AI-Powered Contract Modeling: Digitizing the Rules Engine
The foundation of automated underpayment detection is contract digitization — converting the narrative language of payer contracts into executable rules that a system can apply to every claim, every time. This is where AI transforms contract management from a reactive, sample-based process into a comprehensive, real-time compliance engine.
Contract Term Extraction with NLP
Modern contract management platforms use Natural Language Processing (NLP) to parse contract documents and extract reimbursement terms programmatically. The extraction pipeline typically operates in three stages:
- Document ingestion: PDF contracts, amendment letters, and fee schedule exhibits are OCR-processed and converted to structured text.
- Entity extraction: NLP models identify key contract elements — CPT code ranges, payment percentages, effective dates, modifier rules, carve-out categories, and escalator terms.
- Rule compilation: Extracted terms are compiled into a formal rules engine — essentially a decision tree that maps any combination of (CPT code + place of service + modifier + date of service) to an expected reimbursement amount.
The Contract Rules Engine
A well-designed contract rules engine must handle the layered complexity of real payer contracts. Here is a simplified representation of the rule hierarchy:
class ContractRulesEngine:
def calculate_expected_payment(self, claim_line):
payer_id = claim_line.payer_id
cpt_code = claim_line.cpt_code
dos = claim_line.date_of_service
modifiers = claim_line.modifiers
billed_amount = claim_line.billed_amount
# 1. Check carve-outs first (highest priority)
carveout = self.get_carveout(payer_id, cpt_code, dos)
if carveout:
return carveout.calculate(billed_amount, claim_line)
# 2. Check case rate / DRG bundled payment
if claim_line.is_inpatient:
drg_rate = self.get_drg_rate(payer_id, claim_line.drg_code, dos)
if drg_rate:
return self.apply_stop_loss(drg_rate, claim_line)
# 3. Apply base fee schedule
fee = self.get_fee_schedule_rate(payer_id, cpt_code, dos)
if not fee:
# Fallback: percentage of Medicare
medicare_rate = self.get_medicare_rate(cpt_code, dos)
fee = medicare_rate * self.get_medicare_multiplier(payer_id, dos)
# 4. Apply modifier adjustments
for mod in modifiers:
fee = self.apply_modifier_reduction(payer_id, mod, fee)
# 5. Apply multiple procedure discounting
if claim_line.procedure_sequence > 1:
fee = fee * self.get_multi_proc_discount(payer_id)
return min(fee, billed_amount) # Never expect more than billed
This rules engine runs against every claim line at the moment the ERA/835 remittance is posted, comparing the expected payment to the actual payment received.
Handling Contract Amendments and Version Control
Payer contracts are living documents. Rate amendments, fee schedule updates, and retroactive adjustments arrive throughout the contract term. A production-grade contract management system must maintain versioned contract terms with effective date ranges, allowing the rules engine to apply the correct rates based on the date of service — not the date of payment.
Automated Variance Detection: Expected vs. Actual Reimbursement
With contracts digitized into executable rules, the next layer is automated variance detection — the real-time comparison of expected reimbursement against actual payment received. This is where underpayments surface.
The Variance Detection Pipeline
Every time an ERA/835 remittance is posted to the practice management system, the variance detection engine fires:
- Parse the 835 transaction: Extract payment details at the claim and service-line level, including paid amount, adjustment reason codes (CARCs), and remark codes (RARCs).
- Match to original claim: Link the remittance to the submitted 837 claim using claim control numbers (CLM01) and service line identifiers.
- Calculate expected payment: Run the claim through the contract rules engine using the date-of-service-effective contract terms.
- Compute variance:
Variance = Expected Payment - Actual Payment. Flag any variance exceeding a configurable threshold (typically $5-25 per service line or 2-5% of expected payment). - Classify the variance: Use AI to categorize the root cause — contract term mismatch, modifier-based reduction, bundling/unbundling issue, timely filing denial, or legitimate adjustment.
Variance Classification with Machine Learning
Not every variance is an underpayment worth pursuing. ML models trained on historical variance data learn to distinguish between:
- Recoverable underpayments: Genuine contract violations where the payer paid less than the contracted rate. These have the highest ROI for appeal efforts.
- Documentation-driven denials: Variances caused by missing or insufficient clinical documentation. These require chart review, not contract disputes.
- Legitimate adjustments: Contractually valid payment reductions (coordination of benefits, deductible application, non-covered services). Appealing these wastes resources.
- Systemic configuration errors: Recurring variances caused by incorrect fee schedule loading in the PMS/EMR. Fixing the root cause is more valuable than appealing individual claims.
By scoring each variance for recovery probability and expected dollar value, ML models prioritize the appeal queue — ensuring that revenue cycle staff focus on the variances most likely to result in additional payment.
ERA/835 Analysis for Underpayment Identification
The HIPAA 835 Electronic Remittance Advice is the primary data source for underpayment detection. Understanding its structure at the service-line level is essential for building effective detection systems.
Key 835 Data Elements for Variance Analysis
The 835 transaction contains hierarchical payment information that maps directly to underpayment detection logic:
ISA/GS/ST - Transaction envelope (payer identification)
1000A - Payer identification segment
1000B - Payee (provider) identification
2000 - Claim-level payment info
CLP01 - Patient control number (links to 837)
CLP02 - Claim status (1=Processed, 2=Denied, 4=Denied with appeal)
CLP03 - Total charge amount
CLP04 - Total payment amount ← ACTUAL PAYMENT
2100 - Patient identification
2110 - Service line detail
SVC01 - CPT/HCPCS procedure code
SVC02 - Line-item charge amount
SVC03 - Line-item payment amount ← COMPARE TO EXPECTED
SVC04 - Revenue code
CAS segment - Adjustment reason codes (CARC)
CAS01 - Adjustment group (CO, PR, OA, PI, CR)
CAS02 - CARC code (e.g., 45=Exceeds fee schedule)
CAS03 - Adjustment amount
DTM segment - Service dates
Critical CARC Codes That Signal Underpayments
Certain Claim Adjustment Reason Codes in the CAS segment are strong indicators of potential underpayments:
- CARC 45 — "Charge exceeds fee schedule/maximum allowable": The payer paid their fee schedule rate, which may be lower than the contracted rate.
- CARC 16 — "Claim/service lacks information needed for adjudication": Often used to reduce payment when documentation was deemed insufficient.
- CARC 59 — "Processed based on multiple or concurrent procedure rules": The payer applied multiple procedure discounting that may exceed contractual terms.
- CARC 97 — "Payment adjusted because the benefit for this service is included in the payment for another service": Bundling decision that may conflict with contract carve-outs.
- CARC 197 — "Precertification/authorization absent": Sometimes applied retroactively to reduce payment on services that were pre-authorized.
- CARC 253 — "Sequestration - Loss in payment due to federal government": Applies to Medicare, but should not appear on commercial claims.
Automated ERA Analysis Pattern
Here is a pattern for systematically analyzing 835 data for underpayment indicators:
class ERAUnderpaymentAnalyzer:
UNDERPAYMENT_CARC_CODES = {45, 59, 97, 16, 197, 253}
CONTRACTUAL_ADJUSTMENT_GROUP = 'CO'
PATIENT_RESPONSIBILITY_GROUP = 'PR'
def analyze_remittance(self, era_835):
variances = []
for claim in era_835.claims:
for service_line in claim.service_lines:
expected = self.rules_engine.calculate_expected(
payer_id=era_835.payer_id,
cpt=service_line.procedure_code,
dos=service_line.service_date,
modifiers=service_line.modifiers,
billed=service_line.charge_amount
)
actual = service_line.payment_amount
variance = expected - actual
if variance > self.threshold:
# Check adjustment reason codes
carc_codes = [
adj.reason_code
for adj in service_line.adjustments
if adj.group_code == self.CONTRACTUAL_ADJUSTMENT_GROUP
]
# Flag underpayment signals
underpayment_signals = (
self.UNDERPAYMENT_CARC_CODES
& set(carc_codes)
)
variances.append({
'claim_id': claim.patient_control_number,
'cpt': service_line.procedure_code,
'expected': expected,
'actual': actual,
'variance': variance,
'carc_codes': carc_codes,
'underpayment_signals': list(underpayment_signals),
'recovery_probability': self.ml_model.predict(
service_line, variance, carc_codes
)
})
return sorted(variances, key=lambda v: v['variance'], reverse=True)
This pattern processes every remittance in real time, flagging variances with their root cause indicators and ML-predicted recovery probability. For a deeper look at how ERA processing fits into the broader payment posting workflow, see our guide on Healthcare Payment Posting Automation with ERA, AI, and FHIR Integration.
Appeal Automation for Detected Underpayments
Detecting underpayments is only half the battle — recovering the money requires a systematic appeal process. AI-powered appeal automation transforms what was traditionally a manual, labor-intensive task into a streamlined workflow.
The Automated Appeal Pipeline
- Variance triage: ML model scores each underpayment for recovery probability and expected value. Only variances above the ROI threshold enter the appeal queue.
- Evidence assembly: The system automatically pulls the relevant contract terms, original claim data, remittance details, and any supporting clinical documentation.
- Appeal letter generation: AI generates payer-specific appeal letters that reference exact contract language, cite the specific clause being violated, and include supporting calculations showing the expected vs. actual payment.
- Submission routing: Appeals are routed through the appropriate channel — payer portal, EDI submission, fax, or mail — based on payer-specific requirements and timely filing deadlines.
- Tracking and escalation: Automated follow-up at 30, 60, and 90-day intervals, with escalation to second-level appeals when initial appeals are denied.
- Outcome capture: Appeal results feed back into the ML model, continuously improving recovery predictions and appeal strategy.
Appeal Letter Intelligence
The most effective appeal letters are not generic templates — they are evidence-based arguments that cite specific contract provisions. An AI-generated appeal for a CARC 45 (fee schedule) underpayment might include:
- The specific contract section and paragraph number defining the reimbursement rate for the CPT code in question
- The effective date of the current fee schedule, confirming the rate was in effect on the date of service
- A calculation showing the contractual rate vs. the paid rate, with the specific dollar variance
- Reference to previous successful appeals on the same issue with the same payer, establishing precedent
This approach aligns with the broader trend toward agentic AI in revenue cycle management, where autonomous AI agents handle end-to-end workflows from detection through resolution.
Contract Negotiation Intelligence: Using Data to Win Better Rates
Beyond underpayment recovery, AI-powered contract analysis provides a strategic advantage during contract renewal negotiations. The same data used to detect variances becomes powerful leverage for negotiating better terms.
Benchmark Data and Rate Comparison
Effective negotiation requires knowing where your rates stand relative to the market. AI systems can aggregate and analyze:
- Internal rate comparison: How does Payer A's rate for CPT 99214 compare to Payers B, C, and D? Identify below-market rates for specific code families.
- Medicare benchmark: Express all payer rates as a percentage of Medicare, enabling apples-to-apples comparison across payers and service categories.
- Volume-weighted analysis: Prioritize negotiation efforts on codes that represent the highest revenue volume. A 5% increase on your top 50 CPT codes may be worth more than a 15% increase on codes you rarely bill.
- Denial and underpayment patterns: If a specific payer consistently underpays on modifier
-25claims, that pattern becomes a negotiation point — either clarify the contract language or negotiate an explicit modifier payment policy.
Leverage Points in Contract Negotiations
AI-generated negotiation intelligence reports identify specific leverage points:
- Payer compliance rate: If a payer only pays at the contracted rate 87% of the time, that compliance gap is a negotiation lever — either improve compliance or increase base rates to compensate.
- Effective reimbursement vs. contracted rate: After accounting for denials, underpayments, and appeal costs, what is the true effective rate? This "real rate" often differs significantly from the contracted rate.
- Administrative cost burden: Quantify the cost of managing a specific payer — appeal volume, phone time, portal complexity, timely filing pressure. Contracts with high administrative burden need higher rates to compensate.
- Patient volume leverage: For payers that represent significant patient volume, the provider has negotiating power. Data showing the exact volume and revenue contribution strengthens the position.
Integration with Payment Posting Workflows
Contract management does not exist in isolation — it must integrate tightly with the broader revenue cycle. The most effective implementations embed variance detection directly into the payment posting workflow, catching underpayments at the moment of ERA receipt rather than in retrospective audits.
Real-Time Integration Architecture
The integration pattern for embedding contract variance detection into existing RCM workflows:
ERA/835 Received (Clearinghouse or Direct)
|
Payment Posting Engine (PMS/EMR)
| (parallel)
Contract Variance Detection Engine
+-- Parse 835 service lines
+-- Match to contract rules
+-- Calculate expected vs. actual
+-- Score variance (ML model)
+-- Route to appropriate queue
+-- AUTO-ACCEPT: Variance < threshold -> post payment, no action
+-- REVIEW QUEUE: Moderate variance -> staff review
+-- AUTO-APPEAL: High-confidence underpayment -> generate appeal
+-- ESCALATE: Complex variance -> senior analyst
This architecture ensures that 100% of claims are evaluated against contract terms, not the 10-15% that manual sampling achieves. For organizations managing complex payer relationships including EDI eligibility verification and claims processing, this integration becomes even more critical.
Key Integration Points
- Clearinghouse/EDI gateway: Receive 835 files via SFTP, AS2, or API from clearinghouses (Availity, Change Healthcare, Waystar). Parse and normalize before passing to the variance engine.
- Practice management system: Push variance flags and appeal tasks into existing PMS worklists, so staff see underpayments in their normal workflow — not a separate tool.
- Contract repository: Maintain a centralized, versioned store of all payer contracts with effective dates, enabling the rules engine to always reference the correct terms.
- Reporting and analytics: Feed variance data into BI dashboards for executive-level visibility into underpayment trends, payer performance, and recovery metrics.
Vendor Comparison: Payer Contract Management Platforms
The contract management software market has matured significantly, with several established vendors offering varying levels of automation and AI capability. Here is how the major platforms compare:
MD Clarity (RevFind)
Best for: Mid-size practices and hospitals seeking a purpose-built contract management point solution.
- Strengths: Automated underpayment detection (RevFind product), contract modeling, patient cost estimation. Specializes exclusively in contract management — not a general RCM platform.
- Limitations: Less suited for complex multi-entity health systems. ML capabilities are more limited compared to custom solutions. Appeal automation is basic — generates alerts but limited letter generation.
- Pricing: SaaS model, typically based on claim volume. Competitive for single-facility deployments.
PMMC
Best for: Large health systems and academic medical centers needing enterprise-scale contract management.
- Strengths: Established since 1986 with deep healthcare contract management expertise. Comprehensive platform covering contract modeling, underpayment recovery, A/R collections, and population health analytics. Recognized as a KLAS-rated contract management leader.
- Limitations: Enterprise pricing may be prohibitive for smaller organizations. Implementation timelines can extend 6-12 months. Legacy architecture may limit API-based integration flexibility.
- Pricing: Enterprise license model with implementation fees. Often requires a dedicated internal team for ongoing management.
Waystar Contract Manager
Best for: Organizations already using Waystar for claims management or denial management who want to add contract management to their existing platform.
- Strengths: Tight integration with Waystar's full RCM suite (claims, denials, patient payments). Leverages Waystar's AI and analytics infrastructure. Single-vendor convenience for organizations standardizing on the Waystar platform.
- Limitations: Contract management is one module among many — less depth than purpose-built solutions. ML-based negotiation intelligence is still developing. Less flexible for organizations using non-Waystar RCM components.
- Pricing: Module-based pricing within the broader Waystar platform. Cost-effective as an add-on, more expensive as a standalone.
Custom AI Solutions
Best for: Health systems with complex contract structures, unique payer relationships, or regulatory requirements that off-the-shelf solutions cannot accommodate.
- Strengths: Maximum flexibility in rules engine design, ML model training, and integration architecture. Can incorporate proprietary data sources and custom analytics. Full ownership of the variance detection logic and appeal workflows.
- Limitations: Higher upfront investment in development and data engineering. Requires ongoing ML model maintenance and contract rule updates. Longer time-to-value compared to SaaS platforms.
- Pricing: Development cost varies widely ($200K-$1M+ depending on scope), with ongoing maintenance representing 15-25% of initial build cost annually.
Evaluation Framework
When evaluating contract management solutions, prioritize these criteria:
| Criterion | Why It Matters | What to Look For |
|---|---|---|
| Contract modeling depth | Simple systems cannot handle multi-methodology contracts | Support for % of Medicare, flat fee, DRG, per diem, case rate, and hybrid models |
| Variance detection speed | Retrospective detection delays recovery | Real-time or same-day detection at ERA posting |
| ML classification accuracy | False positives waste staff time | >90% accuracy in distinguishing recoverable underpayments from legitimate adjustments |
| Integration flexibility | The tool must work with your existing PMS/EMR | HL7, FHIR, API, and file-based integration options |
| Appeal automation depth | Detection without recovery is incomplete | Auto-generated appeal letters with contract citations, not just alerts |
| Negotiation intelligence | Underpayment recovery is reactive; better rates are proactive | Benchmark reports, rate comparisons, volume-weighted analysis |
Implementation Roadmap: From Zero to Full Contract Intelligence
Implementing AI-powered contract management is not a single project — it is a phased journey. Here is a practical 12-month roadmap:
Phase 1: Foundation (Months 1-3)
- Digitize the top 10 payer contracts (by revenue volume) into the rules engine
- Establish 835/ERA parsing pipeline with clearinghouse integration
- Implement basic variance detection with configurable thresholds
- Create baseline metrics: current underpayment rate, recovery rate, days to appeal
Phase 2: Intelligence (Months 4-6)
- Train ML model on 6+ months of historical variance data for classification
- Implement appeal letter generation with contract citation logic
- Build payer performance dashboards with rate benchmarking
- Expand to remaining payer contracts (full portfolio coverage)
Phase 3: Optimization (Months 7-12)
- Deploy real-time variance detection embedded in the payment posting workflow
- Implement negotiation intelligence reporting for upcoming contract renewals
- Automate appeal submission and tracking through payer portals and EDI
- Establish a continuous model retraining pipeline using appeal outcome data
Organizations following this roadmap typically see positive ROI within the first 3-6 months as the initial variance detection phase surfaces previously undetected underpayments.
Key Takeaways
Payer underpayments are not an unavoidable cost of doing business — they are a solvable problem. The technology exists today to digitize contract terms, detect variances in real time, classify underpayments with machine learning, and automate the appeal process from detection through recovery.
The hospitals and health systems that invest in contract intelligence now will compound their advantage: every dollar recovered improves margins, every pattern identified strengthens negotiating position, and every automated workflow frees staff for higher-value work.
The $1-3 million question is not whether your organization has underpayments — it is whether you have the systems to find them before they cost you millions.


