Part of our complete guide to Mirth Connect - Complete Guide for Healthcare Leaders.
Every year, health systems make million-dollar integration decisions based on assumptions about Mirth Connect that were never true, or stopped being true years ago. A CIO decides against Mirth because "it is free software with no support." A VP of IT rejects it because "it only handles HL7v2 and we need FHIR."
An integration architect dismisses it because "it cannot scale to our volume." Each of these decisions triggers a cascade: buying an enterprise platform at $500,000 per year, hiring additional staff to manage a more complex system, or building custom middleware that costs more to maintain than the platform it replaced.
The irony is that Mirth Connect, now officially NextGen Connect Integration Engine, powers approximately one-third of all US Health Information Exchanges and processes millions of clinical messages daily across thousands of hospital systems.
According to NextGen Healthcare, the platform supports over 1,700 healthcare organizations globally. The organizations running Mirth successfully are not doing so because they got lucky. They are doing it because they understood the platform's actual capabilities rather than the myths circulating in conference hallways and vendor sales pitches.
This article dismantles the five most persistent myths about Mirth Connect, explains where each myth originated, and provides the real data health system leaders need to make informed integration decisions in 2026.
Myth 1: "Mirth Connect Is Free"
Where This Myth Comes From
For over a decade, Mirth Connect was distributed under an open-source license. Organizations could download it, install it, and run it without paying a licensing fee. This led to an entire generation of healthcare IT leaders believing that Mirth was, and always would be, the "free" integration engine. Budget proposals routinely listed Mirth as a zero-cost line item for the integration platform layer.
The Reality
As of March 2025, Mirth Connect version 4.6 and above is no longer open source. NextGen Healthcare transitioned to a commercial licensing model, meaning new deployments require a paid license. The last open-source version, 4.5.2, was released in September 2024 and remains available, but receives no new features or security patches from NextGen.
But here is the more important point that most people miss: Mirth was never actually free. Even when the software license cost was zero, the total cost of ownership included:
- Staffing: Integration engineers specializing in Mirth Connect command salaries of $120,000 to $180,000 per year in the US market, according to Salary.com data for healthcare integration specialists. You need at least one, and most enterprise deployments need two to three.
- Infrastructure: Server hardware or cloud compute, database licensing (if using a commercial DB), monitoring tools, backup systems. A production Mirth environment with proper high availability typically costs $2,000 to $5,000 per month in cloud infrastructure.
- Training: Mirth has a learning curve. Channel design, JavaScript transformer scripting, MLLP configuration, database connector tuning, and performance optimization all require specialized knowledge that takes months to acquire.
- Opportunity cost: Every hour your integration team spends maintaining the platform is an hour not spent building new interfaces or improving existing ones.
A realistic three-year TCO for a self-hosted Mirth deployment with two integration engineers, proper infrastructure, and support coverage is $500,000 to $900,000. That is not free. It may still be the most cost-effective option compared to alternatives that charge $500 to $2,000 per connection per month, but calling it "free" leads to chronic under-resourcing that causes the very problems people blame on the platform.
What Decision-Makers Should Do
Budget for Mirth like you would any enterprise platform. Include staffing, infrastructure, training, and ongoing maintenance. If you are still running the open-source 4.5.2 version, plan for either upgrading to the commercial license or maintaining a fork, both of which have real costs. For guidance on commercial transition planning, see our analysis of migration strategies for open-source users.
Myth 2: "It Only Handles HL7v2"
Where This Myth Comes From
Mirth Connect was originally built as an HL7v2 interface engine. Its earliest marketing, documentation, and community discussions centered on HL7v2 message routing and transformation. Many people who evaluated Mirth in 2010 or 2015 remember it as "that HL7v2 tool" and never updated their mental model.
The persistent association is reinforced by the fact that 60 to 80 percent of US hospitals still run HL7v2 interfaces, making it the most visible use case.
The Reality
Modern Mirth Connect is a multi-protocol integration engine that supports a remarkably broad range of data formats and communication protocols:
- HL7v2: Full support for all message types, custom segments, Z-segments, and all HL7v2 versions from 2.1 through 2.8.
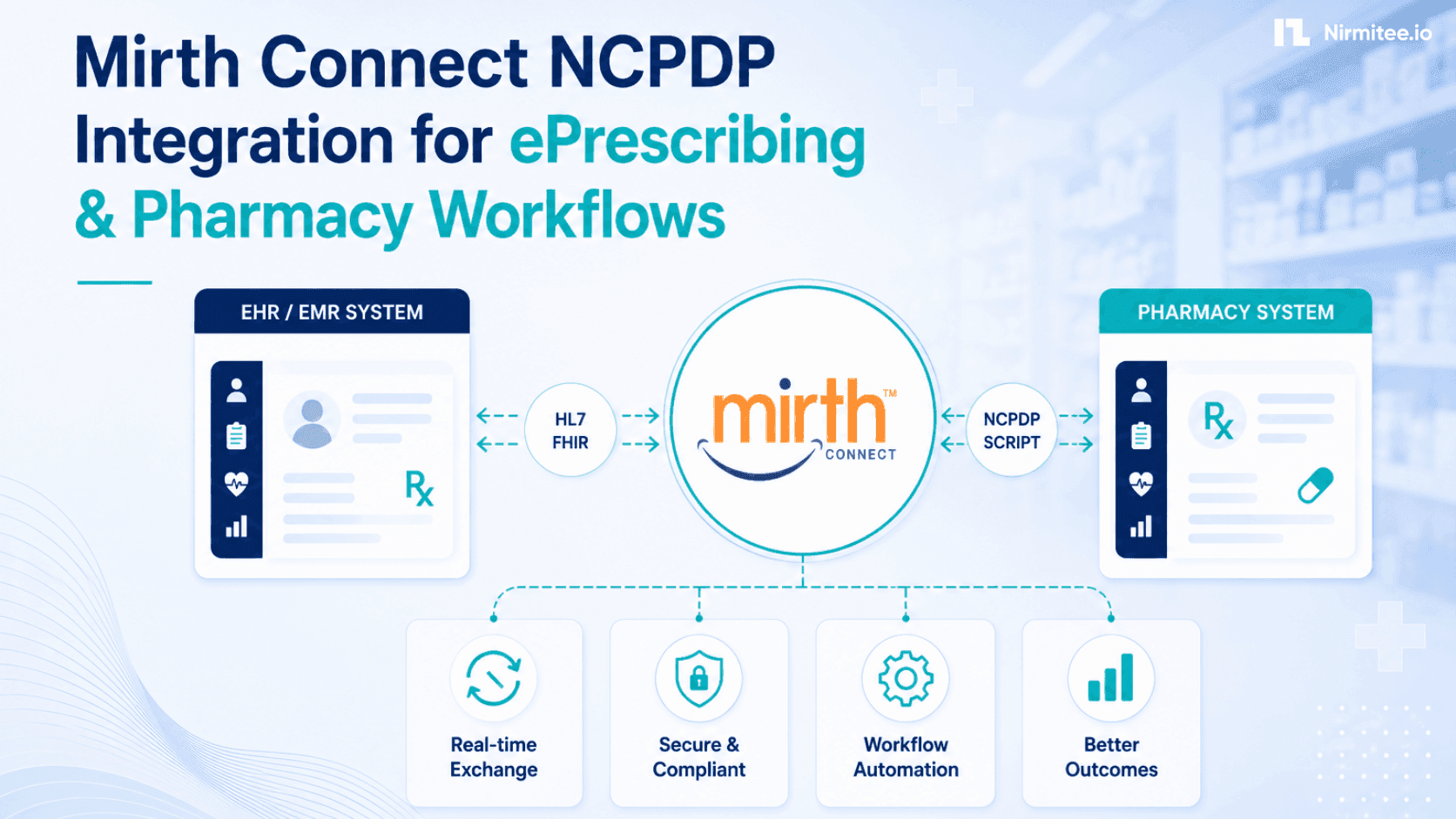
- FHIR R4 and R5: Native FHIR resource handling, FHIR REST client and listener connectors, Bundle processing, and SMART on FHIR authentication support. For a deep dive, see our guide on converting HL7v2 streams into FHIR APIs.
- DICOM: Medical imaging integration for receiving, transforming, and routing DICOM objects between PACS, VNA, and imaging AI systems.
- X12: Healthcare claims and eligibility transactions (835, 837, 270/271, 276/277), enabling payer-provider integration.
- CSV and flat files: Delimited file processing for lab instrument interfaces, registry submissions, and legacy system integration.
- JSON and XML: Full support for modern API payloads, webhook processing, and document-based exchange.
- Database connectors: Direct SQL read/write to PostgreSQL, MySQL, SQL Server, Oracle, and any JDBC-compatible database.
- HTTP/REST and Web Services: RESTful API client and server, SOAP web services, and custom HTTP endpoint creation.
The platform's channel architecture treats message format and transport protocol as independent, configurable layers. You can receive an HL7v2 message over MLLP, transform it to a FHIR Bundle in the channel's transformer, and POST it to a FHIR server via HTTP. Or receive a CSV file via SFTP, parse it into individual records, and insert them into a database. The permutations are extensive.
What Decision-Makers Should Do
Evaluate Mirth against your actual protocol requirements, not your assumptions about what it supports. If your roadmap includes FHIR adoption alongside existing HL7v2 interfaces, Mirth is uniquely positioned to handle both in a single platform, which is exactly the reality most healthcare organizations face when they need both standards.
Myth 3: "It Doesn't Scale"
Where This Myth Comes From
Organizations that deploy Mirth with default settings on undersized hardware and then experience performance problems conclude that "Mirth doesn't scale." This is like installing a database server on a laptop, running out of memory, and concluding that PostgreSQL is not enterprise-grade. The scaling myth is almost always a configuration myth.
The Reality
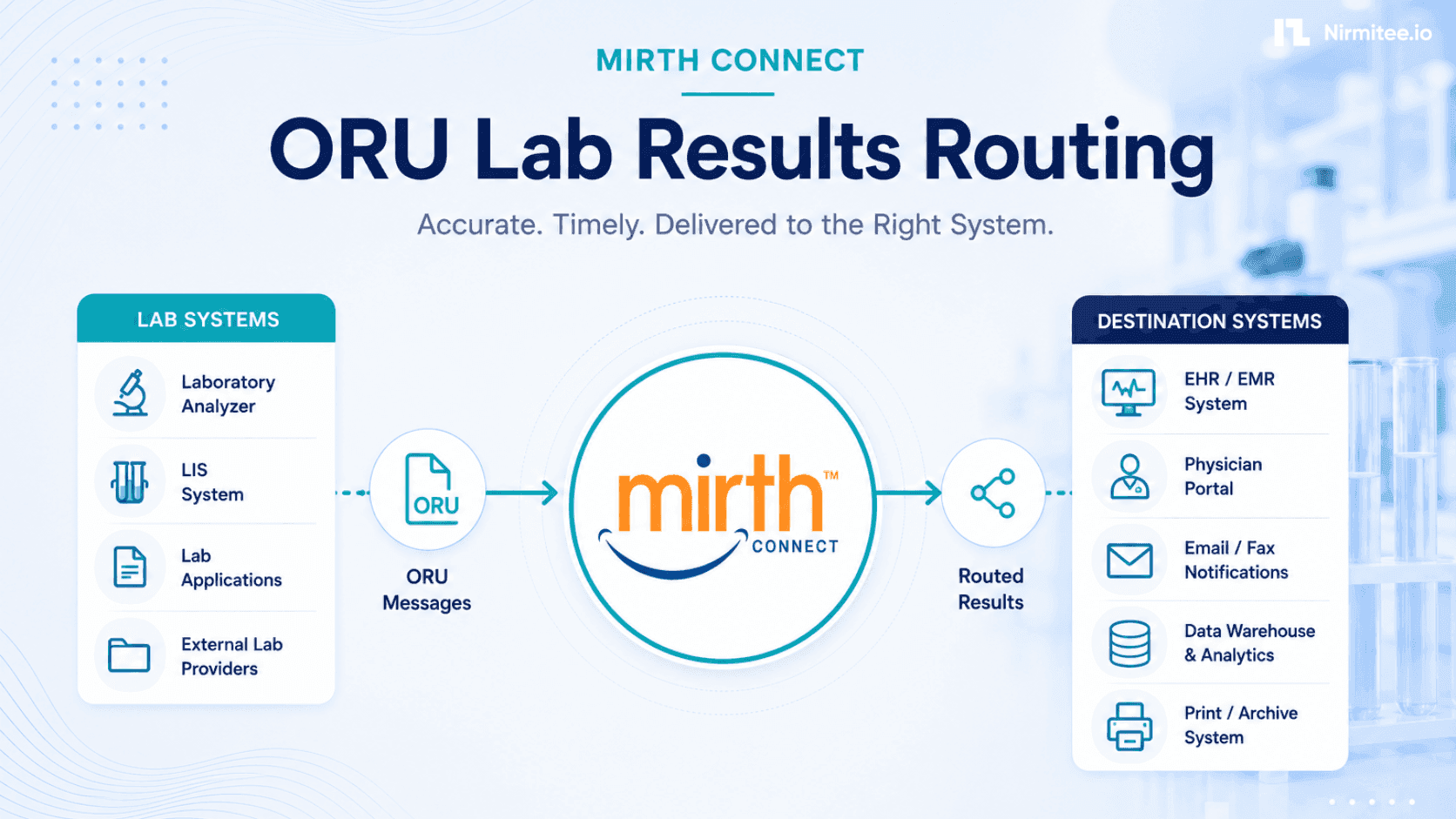
The numbers tell a clear story. Mirth Connect powers approximately one-third of US Health Information Exchanges, according to industry analyses. These are not small deployments. HIEs like the Indiana Health Information Exchange process millions of clinical messages per day, routing ADT notifications, lab results, clinical documents, and care summaries between hundreds of participating organizations.
Scaling Mirth effectively requires attention to three areas:
- JVM tuning: Mirth runs on the Java Virtual Machine. Default heap settings of 256MB or 512MB are absurdly low for production workloads. Enterprise deployments typically allocate 4GB to 16GB of heap memory and configure garbage collection settings appropriate for their message volume and processing patterns. The difference between default settings and a properly tuned JVM can be a 10x improvement in throughput.
- Message storage optimization: Mirth's message storage strategy dramatically affects performance. Storing full raw and transformed message content for every message is necessary for compliance, but expensive at scale. Configuring message pruning schedules, using content storage policies that match your retention requirements, and choosing the right database backend are essential.
- Clustering and horizontal scaling: For the highest-volume deployments, Mirth supports clustering where multiple Mirth instances share a common database and distribute channel processing across nodes. Combined with load balancing for inbound connections, this architecture handles volumes that would overwhelm any single instance. See our guide on setting up Mirth for high availability.
A properly configured single Mirth instance on modern hardware can process 10,000 to 50,000 messages per hour, depending on transformation complexity. A clustered deployment can handle hundreds of thousands. The ceiling is infrastructure and configuration, not platform capability.
What Decision-Makers Should Do
If someone tells you "Mirth doesn't scale," ask them about their JVM heap size, their garbage collection configuration, and their message storage settings. If the answer is "I don't know" or "we used the defaults," the problem is not the platform. Invest in a proper configuration before concluding that you need a more expensive alternative.
Myth 4: "You Need a Huge Team"
Where This Myth Comes From
Organizations that treated Mirth like a legacy enterprise platform, with separate teams for development, testing, deployment, and monitoring, naturally ended up with large teams. The myth is reinforced by consulting firms that staff Mirth projects with five to ten people because that is how they make money, not because the platform requires it.
The Reality
One to two skilled integration engineers can manage 50 or more channels with proper governance, templates, and monitoring. The keyword is "skilled." A skilled Mirth engineer with three or more years of experience, solid JavaScript knowledge, and understanding of healthcare data standards is worth more than a team of five generalists who are learning on the job.
The practices that make small teams effective:
- Channel design patterns: Using standardized channel design patterns means each new interface follows a proven template rather than being built from scratch. A well-designed channel template for ADT processing can be adapted to a new source system in hours rather than days.
- Code template libraries: Shared JavaScript functions for common operations (date formatting, code translation, patient matching) eliminate duplication and reduce errors. When you fix a bug in the shared library, every channel that uses it benefits automatically.
- Automated monitoring: Reliable production monitoring with alerting means engineers are only engaged when something actually needs attention, rather than manually checking channel status throughout the day.
- Self-service interfaces: Well-documented standard interfaces that clinical teams can request through a catalog, rather than requiring custom development for every new connection.
A 2023 survey by HIMSS found that organizations with mature integration practices spent 40 percent less engineering time per interface than those with ad-hoc approaches. The differentiator was not team size but process maturity.
What Decision-Makers Should Do
Invest in hiring one or two excellent integration engineers rather than staffing a mediocre team of five. Pay for Mirth-specific training and certification. Establish governance practices and channel templates from day one. The return on investment in skill and process dramatically exceeds the return on investment in headcount.
Myth 5: "Mirth Is Being Abandoned"
Where This Myth Comes From
When NextGen Healthcare announced the transition from open-source to commercial licensing for Mirth Connect 4.6 and above, many in the healthcare IT community interpreted this as "the beginning of the end." Open-source advocates saw it as a betrayal. Competing vendors seized the narrative, telling prospects that Mirth's best days were behind it and that organizations should migrate to their platform before it was "too late."
The Reality
The commercial transition signals the exact opposite of abandonment. NextGen Healthcare invested in converting Mirth to a commercial product because they see long-term revenue potential, which means long-term development investment. Companies do not invest in commercializing dying products.
The evidence of continued investment:
- Active development: Mirth Connect continues to receive regular updates with new features, security patches, and performance improvements. The commercial model funds a dedicated engineering team larger than what the open-source community contribution model ever supported.
- Mirth Fully Managed: NextGen launched a fully managed cloud service for Mirth Connect, eliminating the infrastructure management burden. This is a significant product investment that would not exist if the platform were being abandoned.
- Ecosystem growth: The Mirth Connect partner ecosystem continues to expand, with certified consulting firms, training providers, and complementary tool vendors building businesses around the platform.
The real risk is not that Mirth will be abandoned. The real risk is that organizations running the last open-source version (4.5.2) will fall behind on security patches and new capabilities. That is a legitimate planning concern, but it is fundamentally different from platform abandonment.
What Decision-Makers Should Do
Evaluate the commercial licensing terms against your budget and needs. If the cost is justified, upgrade to the commercial version and benefit from active support and development.
If the budget is constrained, evaluate the open-source 4.5.2 fork community and plan accordingly. Either way, build your integration strategy on the assumption that Mirth Connect will continue to be a major player in healthcare integration for years to come.
Why These Myths Persist
Healthcare IT myths persist because the industry has structural incentives to maintain them:
- Vendor competition: Every competing integration platform vendor benefits when prospects believe Mirth is limited, difficult, or dying. Sales teams amplify myths because myths drive revenue.
- Consulting incentives: Consulting firms that staff large integration teams benefit from the myth that you need a huge team. Firms that sell expensive platforms benefit from the myth that Mirth is hard to use.
- Outdated experience: Decision-makers who last touched Mirth in 2015 genuinely believe their outdated experience reflects the current state. They are not lying; they are just wrong.
- Confirmation bias: Organizations that had a bad experience with Mirth due to under-resourcing or poor configuration attribute the failure to the platform rather than the implementation. Their stories become cautionary tales that other organizations take at face value.
How to Make Informed Decisions
If you are evaluating integration platforms in 2026, here is how to cut through the myths:
- Run a proof of concept. Install Mirth Connect in a test environment and build one representative interface. This takes one to two weeks with a skilled engineer and answers more questions than six months of vendor demos.
- Talk to current users, not former users. Find organizations currently running Mirth at scale, ideally with a similar volume and complexity to yours. Ask about their team size, their challenges, and their TCO. The Mirth community forums are a good starting point.
- Calculate real TCO for all options. Include staffing, infrastructure, licensing, training, and migration costs for every platform you are evaluating. The cheapest license is not always the cheapest solution, and the most expensive license is not always the best value.
- Evaluate against your roadmap, not today's needs. If you need HL7v2 today but will need FHIR in two years, evaluate whether each platform handles both. If you have 10 interfaces today but will have 50 in three years, evaluate scaling capabilities. For a comprehensive view of interoperability standards, see our detailed guide.
- Separate platform problems from implementation problems. If someone says, "We tried Mirth, and it didn't work," dig deeper. Was the platform actually incapable, or was the implementation under-resourced, poorly designed, or mismanaged? The answer is almost always the latter.
The Bottom Line
Mirth Connect is not free, not limited to HL7v2, not unable to scale, not requiring a huge team, and not being abandoned. It is a commercial, multi-protocol integration engine that powers a significant portion of the US healthcare data exchange infrastructure. Whether it is the right choice for your organization depends on your specific requirements, budget, team capabilities, and integration roadmap.
The millions that these myths cost health systems are not spent on Mirth itself. They are spent on alternatives chosen because of false assumptions, on over-staffed teams because of incorrect complexity estimates, and on delayed projects because of unfounded scaling concerns. The most expensive integration decision is one made on myths instead of data.
Related guides
This article is part of our complete guide to Mirth Connect: What Is Mirth Connect? Complete 2026 Guide for Healthcare Leaders. Related deep-dives:
- What Is Mirth Connect? Complete 2026 Guide for Healthcare Leaders
- Mirth Connect Guide: Architecture, Channels, Deployment, and Performance Tuning
Need production-grade Mirth Connect help? See our Mirth Connect integration services.