A physician submits a prior authorization request for a cardiac MRI. The payer's portal times out. The fax goes unanswered. Four days later, a denial arrives citing "insufficient clinical documentation" — despite the patient's ejection fraction of 25% being clearly documented in the EHR. The physician's staff spends another 90 minutes on a peer-to-peer review call. The patient waits 11 more days. This is not an edge case. This is Tuesday.
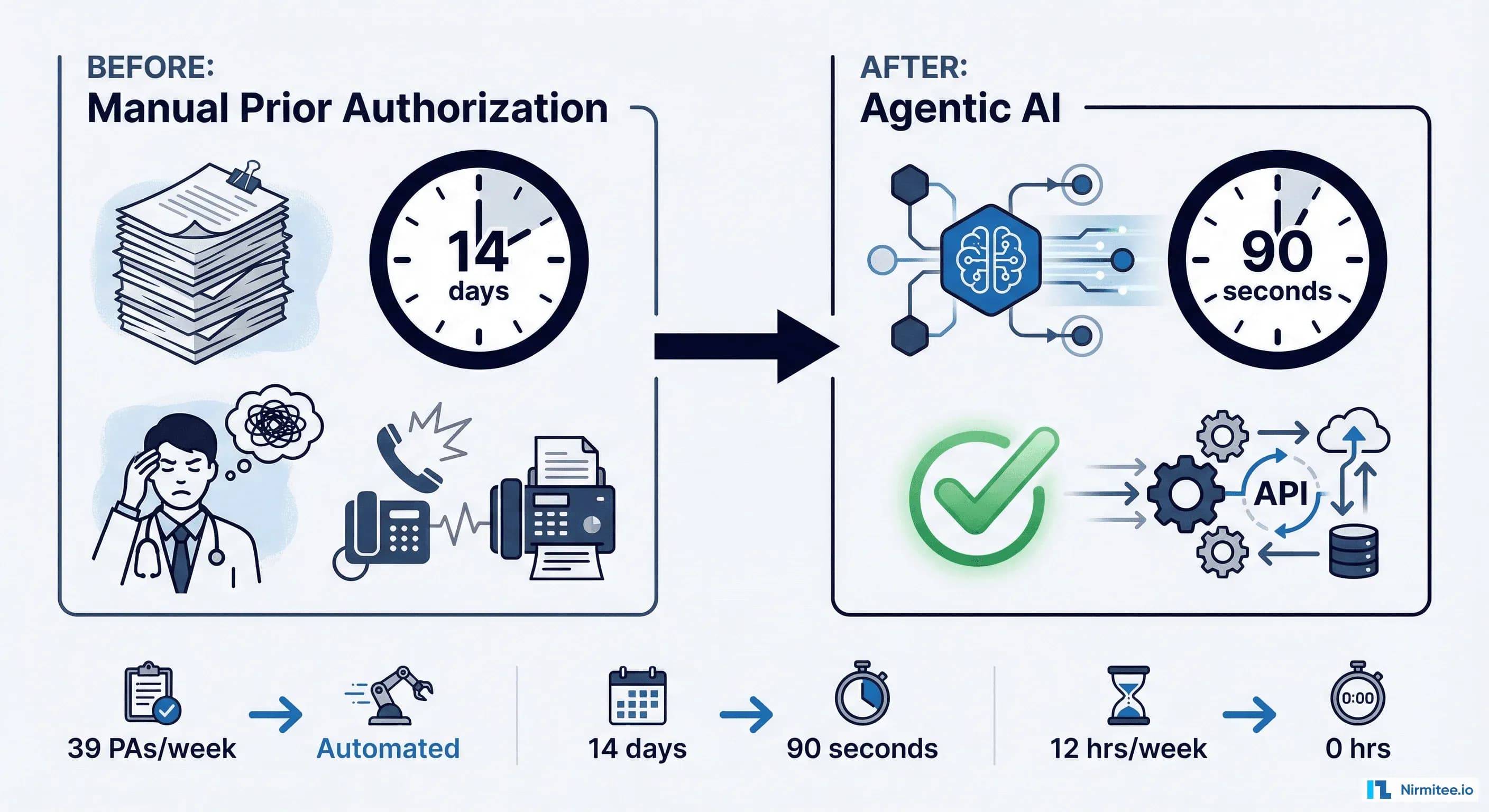
The American Medical Association's 2024 Prior Authorization Survey reports that physicians complete an average of 39 prior authorizations per week, consuming 12-13 hours of staff time — nearly two full working days dedicated entirely to paperwork that rarely changes clinical outcomes. Meanwhile, the CAQH Index estimates that full automation of prior authorization, eligibility verification, and claims status inquiries could unlock $20 billion in annual savings across the US healthcare system.
The math is simple: prior authorization is the single highest-ROI target for agentic AI in healthcare. And with CMS mandates that took effect on March 31, 2026, the regulatory window for incremental improvement has closed. Health plans and providers that haven't automated PA workflows are now operating in violation of federal reporting requirements.
This post breaks down the technical architecture, real-world performance data, and implementation roadmap for deploying agentic AI systems that reduce prior authorization turnaround from 14 days to under 90 seconds.
The Prior Authorization Crisis: Why It's Worse Than You Think
Prior authorization was designed as a utilization management tool — a check against unnecessary procedures. In practice, it has metastasized into a $35 billion administrative burden that delays care, burns out clinicians, and kills patients.
The Cost Arithmetic
Consider the fully loaded cost of a single prior authorization:
- Provider side: 20-45 minutes of staff time per PA (physician + coordinator), at blended rates of $80-120/hour = $27-90 per transaction
- Payer side: Clinical review, nurse reviewer time, medical director escalations = $15-50 per transaction
- System-wide: With an estimated 250-300 million PA transactions annually in the US, total administrative spend exceeds $35 billion
The CAQH Index calculates that the medical industry could save $449 million annually by converting just PA transactions from manual to fully electronic — and that figure assumes basic automation, not intelligent automation.
Clinical Harm Is Documented
The AMA's survey data is unambiguous:
- 93% of physicians report care delays due to PA
- 33% report that PA has led to a serious adverse event for a patient
- 82% say PA sometimes leads to treatment abandonment
- One in four physicians report that PA has led to patient hospitalization
These are not marginal inefficiencies. PA-related delays in cancer treatment, cardiovascular interventions, and behavioral health access represent a measurable mortality signal that health systems can no longer justify.
Physician Burnout Accelerator
The AMA survey found that 35% of physicians have staff who work exclusively on PA. In specialty practices — oncology, cardiology, rheumatology — that figure exceeds 50%. This is skilled clinical labor redirected from patient care to form completion, fax transmission, and hold queues. The downstream effect on burnout, recruitment, and retention is well-documented in Annals of Internal Medicine research linking administrative burden directly to clinician attrition.
What Changed in 2026: CMS Mandates and the Regulatory Push
On March 31, 2026, the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) entered its enforcement phase. This is the most significant regulatory shift in PA since the ACA. Here is what it requires:
Mandatory Public Reporting
Health plans operating in Medicare Advantage, Medicaid, CHIP, and federal exchange programs must now publicly report:
- PA approval and denial rates, broken down by item and service
- Average turnaround times for standard and expedited decisions
- Appeal overturn rates
- Top reasons for denial
This transparency mandate is the regulatory equivalent of turning on stadium lights. Plans that have been denying 30-40% of PAs for common procedures will now face public scrutiny, CMS audit risk, and competitive pressure from plans with cleaner metrics.
Compressed Decision Timelines
The final rule mandates:
| Decision Type | Previous Standard | New CMS Mandate (2026) |
|---|---|---|
| Standard PA decisions | 14 calendar days | 7 calendar days |
| Expedited/urgent PA decisions | 72 hours | 72 hours (unchanged but now enforced with reporting) |
| Specific reason for denial | Not required | Mandatory with each denial |
The compression from 14 to 7 days for standard decisions — combined with mandatory denial reason specificity — means health plans cannot sustain current manual review processes. The IDC's 2026 report, "The U.S. Healthcare Prior Authorization Crisis: Will Agentic AI Come to the Rescue?", identifies this regulatory compression as the primary catalyst driving payer investment in AI-powered PA systems.
PARDD API and FHIR-Based Exchange
CMS also mandates that impacted payers implement a Prior Authorization Requirements, Documentation, and Decision (PARDD) API built on HL7 FHIR standards. This API must:
- Return PA requirements to providers in a structured, queryable format
- Accept PA submissions electronically via FHIR resources
- Communicate decisions and status updates through standardized FHIR endpoints
This is the regulatory foundation that makes agentic AI architectures viable. Without standardized, machine-readable PA rules and FHIR-based submission channels, AI agents would have nothing to act on. The PARDD API gives them a structured operating surface.
How Agentic AI Solves Prior Authorization
Most "AI for PA" solutions on the market are glorified form-fillers: they pre-populate fields from the EHR, suggest ICD-10 codes, and maybe flag missing documentation. That is automation. It is not agentic AI.
Agentic AI is fundamentally different. An AI agent for prior authorization is a system that can autonomously reason through multi-step workflows, make decisions under uncertainty, interact with external systems, and escalate to humans only when its confidence drops below a defined threshold.
The Five Capabilities That Make PA Agents "Agentic"
- Autonomous clinical data gathering: The agent reads the patient's EHR — problem list, medications, lab results, imaging reports, prior treatments — and assembles the clinical narrative without human direction. It knows which data points each payer requires for each procedure because it has ingested the payer's medical policy documents.
- Multi-step reasoning over payer rules: Rather than pattern-matching against a static rules table, the agent performs chain-of-thought reasoning: "This patient needs a cardiac MRI. Payer X requires documentation of two prior non-invasive tests AND an ejection fraction below 35% OR symptoms of heart failure with preserved EF. The patient has an EF of 25% and a prior stress test from January. Criteria met on pathway A." This is the reasoning layer that distinguishes agents from RPA bots.
- Proactive gap identification and resolution: If clinical documentation is insufficient, the agent does not simply flag "missing data." It identifies specifically what is needed ("HbA1c within last 90 days"), checks if the data exists elsewhere in the EHR (e.g., a recent lab import), and if not, drafts a clinical query to the ordering physician with the exact gap identified.
- Submission and follow-up orchestration: The agent submits the PA through the appropriate channel — PARDD API, payer portal, or X12 278 transaction — and monitors for responses. If a request is pended, the agent identifies the pend reason and initiates the appropriate response workflow without human intervention.
- Continuous learning from outcomes: Every approval, denial, and appeal outcome feeds back into the agent's understanding of payer behavior. Over time, the agent learns that Payer X denies lumbar MRIs unless conservative treatment is documented for 6+ weeks, while Payer Y accepts 4 weeks. This institutional knowledge — currently locked in the heads of experienced PA coordinators — becomes a durable, scalable system asset.
This architecture aligns with what we've described as bounded autonomy — the agent operates independently within well-defined clinical and regulatory guardrails, with human oversight for edge cases and high-risk decisions.
Technical Architecture: Building a FHIR-Native PA Agent
A production-grade PA agent requires four integrated layers: data ingestion, clinical reasoning, transaction execution, and feedback. Here is the reference architecture we use when building these systems with FHIR-native infrastructure.
Layer 1: FHIR Data Ingestion
The agent authenticates to the EHR via SMART on FHIR and retrieves the clinical context needed for the PA request. The relevant FHIR R4 resources include:
- Patient — demographics, identifiers, insurance coverage
- Coverage — active insurance plans, member IDs, payer endpoints
- Condition — active problem list with ICD-10 codes
- MedicationRequest / ServiceRequest — the item requiring authorization
- Observation — lab results, vitals relevant to medical necessity
- DiagnosticReport — imaging and pathology results
- DocumentReference — clinical notes, letters of medical necessity
Layer 2: CoverageEligibilityRequest — Checking PA Requirements
Before submitting a PA, the agent first checks whether authorization is required and what documentation the payer needs. The FHIR CoverageEligibilityRequest resource is the starting point:
{
"resourceType": "CoverageEligibilityRequest",
"id": "pa-check-cardiac-mri-001",
"status": "active",
"purpose": ["auth-requirements"],
"patient": {
"reference": "Patient/patient-john-smith"
},
"created": "2026-04-01",
"provider": {
"reference": "Organization/nirmitee-cardiology-group"
},
"insurer": {
"reference": "Organization/payer-anthem-medicaid"
},
"insurance": [
{
"coverage": {
"reference": "Coverage/coverage-anthem-ma-0042"
}
}
],
"item": [
{
"category": {
"coding": [
{
"system": "https://x12.org/codes/service-type-codes",
"code": "3",
"display": "Consultation"
}
]
},
"productOrService": {
"coding": [
{
"system": "http://www.ama-assn.org/go/cpt",
"code": "75561",
"display": "Cardiac MRI with contrast"
}
]
},
"provider": {
"reference": "Practitioner/dr-sarah-chen"
},
"facility": {
"reference": "Location/nirmitee-imaging-center"
},
"diagnosis": [
{
"diagnosisCodeableConcept": {
"coding": [
{
"system": "http://hl7.org/fhir/sid/icd-10-cm",
"code": "I50.9",
"display": "Heart failure, unspecified"
}
]
}
}
]
}
]
}The payer's PARDD API responds with a CoverageEligibilityResponse indicating whether PA is required, what documentation is needed, and the applicable questionnaire (Da Vinci DTR). The agent parses this response and maps the requirements to available clinical data.
Layer 3: Claim (Pre-Authorization) Submission
Once the agent has assembled the required documentation, it submits the PA using the FHIR Claim resource with use: "preauthorization":
{
"resourceType": "Claim",
"id": "pa-submit-cardiac-mri-001",
"status": "active",
"type": {
"coding": [
{
"system": "http://terminology.hl7.org/CodeSystem/claim-type",
"code": "professional"
}
]
},
"use": "preauthorization",
"patient": {
"reference": "Patient/patient-john-smith"
},
"created": "2026-04-01T10:30:00Z",
"provider": {
"reference": "Practitioner/dr-sarah-chen"
},
"insurer": {
"reference": "Organization/payer-anthem-medicaid"
},
"priority": {
"coding": [
{
"system": "http://terminology.hl7.org/CodeSystem/processpriority",
"code": "normal"
}
]
},
"insurance": [
{
"sequence": 1,
"focal": true,
"coverage": {
"reference": "Coverage/coverage-anthem-ma-0042"
}
}
],
"diagnosis": [
{
"sequence": 1,
"diagnosisCodeableConcept": {
"coding": [
{
"system": "http://hl7.org/fhir/sid/icd-10-cm",
"code": "I50.9",
"display": "Heart failure, unspecified"
}
]
}
}
],
"item": [
{
"sequence": 1,
"productOrService": {
"coding": [
{
"system": "http://www.ama-assn.org/go/cpt",
"code": "75561",
"display": "Cardiac MRI with contrast"
}
]
},
"servicedDate": "2026-04-10",
"quantity": {
"value": 1
}
}
],
"supportingInfo": [
{
"sequence": 1,
"category": {
"coding": [
{
"system": "http://terminology.hl7.org/CodeSystem/claiminformationcategory",
"code": "info"
}
]
},
"valueReference": {
"reference": "Observation/ef-measurement-25-percent"
}
},
{
"sequence": 2,
"category": {
"coding": [
{
"system": "http://terminology.hl7.org/CodeSystem/claiminformationcategory",
"code": "info"
}
]
},
"valueReference": {
"reference": "DiagnosticReport/stress-test-jan-2026"
}
}
]
}Layer 4: Task-Based Workflow Tracking
The FHIR Task resource tracks the PA through its lifecycle — from initial submission through payer review, pend resolution, and final determination. The agent monitors task status and autonomously responds to pender requests, information needs, or escalation triggers.
Da Vinci Implementation Guides
The agent's FHIR integration should conform to the Da Vinci Prior Authorization Support (PAS) and Documentation Templates and Rules (DTR) implementation guides. PAS defines the FHIR-based PA submission and response workflow. DTR defines how payer-specific questionnaires are dynamically rendered and auto-populated from EHR data — a task ideally suited for an AI agent that can reason about which clinical data satisfies which questionnaire fields.
Real-World Results: Who's Shipping and What They're Seeing
Agentic PA is not theoretical. Multiple organizations are in production, and their performance data validates the architecture.
Optum: 96% First-Pass Approval Rate
Optum's AI-powered PA platform, launched in late 2025, reports:
- 45% reduction in manual touches per PA request
- 56% reduction in review turnaround time
- 96% first-pass approval rate for submissions processed through the AI system
The 96% first-pass rate is the critical metric. Every PA that requires rework — resubmission, additional documentation, peer-to-peer — costs 3-5x the original submission in staff time and elapsed days. A high first-pass rate is not just efficient; it is the primary driver of patient access speed.
Availity AuthAI: 90-Second Recommendations
Availity's AuthAI platform (marketed under the Intelligentum brand) processes PA requests and returns a recommendation — approve, deny, or escalate — in under 90 seconds on average. The system integrates with the payer's medical policy engine and clinical evidence databases, performing the same multi-step review that previously required a nurse reviewer spending 15-30 minutes per case.
Cohere Health: Intelligent Prior Authorization at Scale
Cohere Health's platform combines clinical intelligence with PA automation, reporting that over 50% of PA requests are auto-determined without human review. Their system ingests clinical guidelines (InterQual, MCG, proprietary payer policies) and performs automated medical necessity determination — the most complex and clinician-dependent step in the PA workflow.
Amazon Connect Health: Big Tech Enters the Arena
In March 2026, Amazon launched Connect Health, an agentic AI platform explicitly targeting healthcare administrative workflows including prior authorization, scheduling, and patient communication. Amazon's entry signals that PA automation has crossed the threshold from niche healthIT to infrastructure-layer opportunity. Connect Health leverages Amazon's existing contact center AI (Amazon Connect) combined with healthcare-specific LLM fine-tuning.
Industry-Wide Momentum
The Deloitte 2026 Health Care Executive Outlook survey found that 93% of health plan executives expect AI to add measurable value through automated prior authorization within the next 18 months. Gartner's 2026 Market Guide for Intelligent Prior Authorization further validates the category, identifying it as one of the fastest-growing segments in health IT investment. Meanwhile, IDC's healthcare research positions agentic AI as the technology best suited to address the structural PA crisis that incremental automation has failed to solve.
The data also shows that 52.5% of US healthcare providers are now adopting composable IT architectures specifically designed to support electronic PA workflows — a precondition for agentic AI deployment.
Implementation Roadmap: From Pilot to Production
Deploying an agentic PA system is not a weekend hackathon. It requires careful orchestration across clinical, technical, compliance, and operational teams. Here is a four-phase approach based on our experience building FHIR-native AI agent infrastructure for health systems.
Phase 1: Foundation (Weeks 1-6)
- FHIR connectivity audit: Map your EHR's FHIR R4 API surface. Identify which resources are available (Patient, Coverage, Condition, ServiceRequest, Observation), their completeness, and any custom extensions. If you are on Epic, Cerner, or MEDITECH Expanse, the USCDI-mandated APIs provide a solid baseline.
- Payer rule ingestion: Collect medical policies, InterQual/MCG criteria subscriptions, and payer-specific PA requirements for your top 10 procedures by volume. Structure these as machine-readable rule sets.
- HIPAA and compliance framework: Establish the HIPAA-compliant AI agent architecture — including data handling agreements, audit logging, PHI de-identification boundaries, and human escalation triggers. This is not optional pre-work; it is the foundation that determines whether your agent can operate in production.
- Baseline metrics: Measure current PA volume, turnaround times, denial rates, first-pass approval rates, and staff hours per PA. You cannot demonstrate ROI without a baseline.
Phase 2: Pilot (Weeks 7-14)
- Select 2-3 high-volume, low-complexity PA categories: Start with procedures that have clear, binary authorization criteria — advanced imaging (MRI, CT), physical therapy visits, DME. Avoid starting with complex categories like specialty drugs or transplant services.
- Deploy in "co-pilot" mode: The agent assembles the PA package and recommends a submission, but a human reviews and approves before submission. This builds trust, surfaces edge cases, and generates training data.
- Measure and iterate: Track first-pass approval rate, time-to-submission, documentation completeness score, and human override rate. Aim for <10% human override rate before advancing to autonomous mode.
Phase 3: Scale (Weeks 15-26)
- Enable autonomous submission for categories where pilot data shows >95% first-pass approval and <5% override rate.
- Expand to 10-15 PA categories, progressively including higher-complexity procedures.
- Integrate denial management: Train the agent to parse denial reasons, identify correctable documentation gaps, and auto-generate appeal packages with additional clinical evidence.
- Connect to payer PARDD APIs as they become available under the CMS mandate, replacing portal-based and fax-based submission channels.
Phase 4: Optimize (Ongoing)
- Payer-specific model tuning: Each payer has distinct approval patterns. The agent's reasoning layer should maintain payer-specific probability models that improve with every outcome.
- Predictive PA: Shift from reactive ("order placed, PA needed") to predictive ("based on this patient's clinical trajectory, a cardiac MRI will likely be ordered in 2-3 weeks — begin pre-authorization assembly now").
- Cross-system intelligence: Aggregate anonymized PA outcome data across provider clients to build industry-wide payer behavior models.
What Agentic PA Means for Different Stakeholders
For Health System CXOs and CFOs
PA automation is a direct margin improvement. A 500-physician medical group processing 2,000 PAs per week at a blended cost of $45/PA spends $4.68 million annually on PA administration alone. At an 85% automation rate — consistent with what Optum and Availity are demonstrating — that drops to under $1.2 million. The ROI case closes in 6-9 months for most implementations.
Beyond cost, agentic PA reduces time-to-treatment, which directly impacts quality metrics tied to value-based contracts and HEDIS measures. Faster PA approval means faster procedure scheduling, which means better outcomes scores.
For Payer CTOs and Medical Directors
The CMS reporting mandate creates an existential transparency problem. Plans with high denial rates and slow turnaround times will face competitive disadvantage, regulatory scrutiny, and member attrition. AI-powered PA review — particularly systems that can apply medical policy with documented reasoning chains — provides both operational efficiency and defensible clinical decision support.
The Deloitte survey's 93% figure reflects this urgency: payer executives are not asking whether AI will transform PA, but how quickly they can deploy it.
For Health IT Engineering Leaders
Agentic PA is a forcing function for FHIR maturity. You cannot build an effective PA agent on top of HL7v2 ADT feeds and PDF clinical notes. The agent needs structured FHIR resources, SMART on FHIR authentication, and a CDS Hooks integration layer for real-time triggers. If your organization's FHIR infrastructure is immature, the PA agent project will expose every gap — which makes it a high-value catalyst for broader interoperability investment.
For Patients
Patients experience PA as unexplained delays, repeated phone calls, and anxiety about whether their insurance will cover a medically necessary procedure. Agentic PA reduces the gap between "doctor orders it" and "insurance approves it" from days or weeks to minutes. For time-sensitive conditions — stroke rehabilitation, cancer treatment initiation, behavioral health interventions — this is the difference between recovery and decline.
Frequently Asked Questions
What is agentic AI for prior authorization?
Agentic AI for prior authorization refers to autonomous AI systems that can independently execute multi-step PA workflows: gathering clinical documentation from the EHR, reasoning against payer medical policies, assembling and submitting authorization requests, monitoring for responses, and resolving pends — all with minimal human intervention. Unlike basic automation or RPA, agentic AI systems perform clinical reasoning, adapt to payer-specific requirements, and learn from approval and denial outcomes over time.
How does the 2026 CMS prior authorization rule affect health plans?
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F), effective March 31, 2026, requires health plans in Medicare Advantage, Medicaid, CHIP, and federal exchange programs to publicly report PA approval rates, denial rates, turnaround times, and appeal outcomes. Standard PA decisions must now be completed within 7 calendar days (down from 14), and every denial must include a specific reason. Plans must also implement FHIR-based PARDD APIs for electronic PA submission and requirements checking.
What ROI can health systems expect from AI-powered prior authorization?
Based on published data from Optum, Availity, and Cohere Health, organizations implementing AI-powered PA systems report 45-56% reductions in review time, 75-85% reduction in manual touches, and first-pass approval rates exceeding 95%. For a mid-size health system processing 2,000 PAs per week, this translates to approximately $3-4 million in annual savings from reduced staff time, fewer rework cycles, and faster reimbursement. The CAQH Index estimates $20 billion in industry-wide savings from full PA automation.
Is AI prior authorization HIPAA compliant?
AI PA systems can be built to be fully HIPAA compliant, but compliance is an architectural decision, not an inherent property of the technology. Key requirements include: BAA agreements with AI vendors, end-to-end encryption for PHI in transit and at rest, comprehensive audit logging of all agent actions and clinical data access, minimum necessary data principles in agent design, and human oversight mechanisms for high-risk decisions. The HIPAA-compliant AI agent architecture must be established before any clinical data flows through the system.
What FHIR resources are used in prior authorization workflows?
The primary FHIR R4 resources for PA workflows include: CoverageEligibilityRequest and CoverageEligibilityResponse (checking PA requirements), Claim with use: "preauthorization" (submitting the PA), ClaimResponse (receiving the payer's decision), Task (tracking workflow status), and supporting clinical resources like Condition, Observation, DiagnosticReport, and DocumentReference. The Da Vinci PAS and DTR implementation guides define the standard profiles for these resources in PA contexts.
How long does it take to implement an agentic PA system?
A typical implementation follows a four-phase approach spanning 6-9 months to full production. Phase 1 (Foundation, 6 weeks) covers FHIR connectivity, payer rule ingestion, and compliance setup. Phase 2 (Pilot, 8 weeks) deploys the agent in co-pilot mode for 2-3 high-volume PA categories. Phase 3 (Scale, 12 weeks) enables autonomous submission and expands to 10-15 categories. Phase 4 (Optimize) is ongoing, covering payer-specific tuning and predictive PA capabilities. Organizations with mature FHIR infrastructure can compress Phases 1-2 significantly.
The Window Is Open — But Closing
Prior authorization has been healthcare's most complained-about administrative process for a decade. What changed in 2026 is that complaints became mandates: CMS now requires the transparency, speed, and digital infrastructure that makes agentic AI not just viable, but necessary.
The organizations deploying PA agents today — Optum, Availity, Cohere Health, and a growing number of health systems running their own FHIR-native implementations — are building a structural advantage. Their first-pass approval rates will be higher. Their staff costs will be lower. Their patients will get to treatment faster. And their CMS-mandated public metrics will prove it.
The organizations that wait will face compressed timelines, scarce implementation talent, and competitors who have already trained their agents on millions of PA outcomes.
At Nirmitee, we build the FHIR interoperability layer and AI agent infrastructure that health systems and payers need to make agentic PA a reality — from SMART on FHIR connectivity and Da Vinci IG implementation to autonomous agent orchestration with bounded autonomy guardrails. If your organization is evaluating PA automation or building its 2026-2027 interoperability roadmap, we should talk.
Related reading
For more insights, explore our guides on AI agents in healthcare: an overview and FHIR in Modern Healthcare.
You may also find value in EHR Software Development Guide and Building a Healthtech App.