Why Code Stacking Is the Biggest Revenue Opportunity in Remote Care
Most healthcare practices leave significant revenue on the table by billing only a single remote care program per patient. In 2026, CMS allows providers to bill multiple remote care programs simultaneously for the same patient — a strategy known as code stacking. A patient enrolled in RPM alone generates approximately $150-160 per month. That same patient, when properly enrolled in RPM + CCM + RTM, can generate $360 or more per month — a 140% revenue increase with no additional patient acquisition cost.
According to CMS's 2026 Medicare Physician Fee Schedule, remote care management codes received a 10%+ reimbursement increase, making code stacking more financially attractive than ever. This guide breaks down every CPT code, stacking rule, eligibility requirement, and revenue calculation you need to implement a compliant, high-revenue remote care billing strategy.

Understanding the Four Remote Care Programs
Before stacking codes, you must understand each program's scope, CPT codes, and reimbursement rates. Each program serves a distinct clinical purpose — and CMS requires that billed time and services do not overlap between programs.
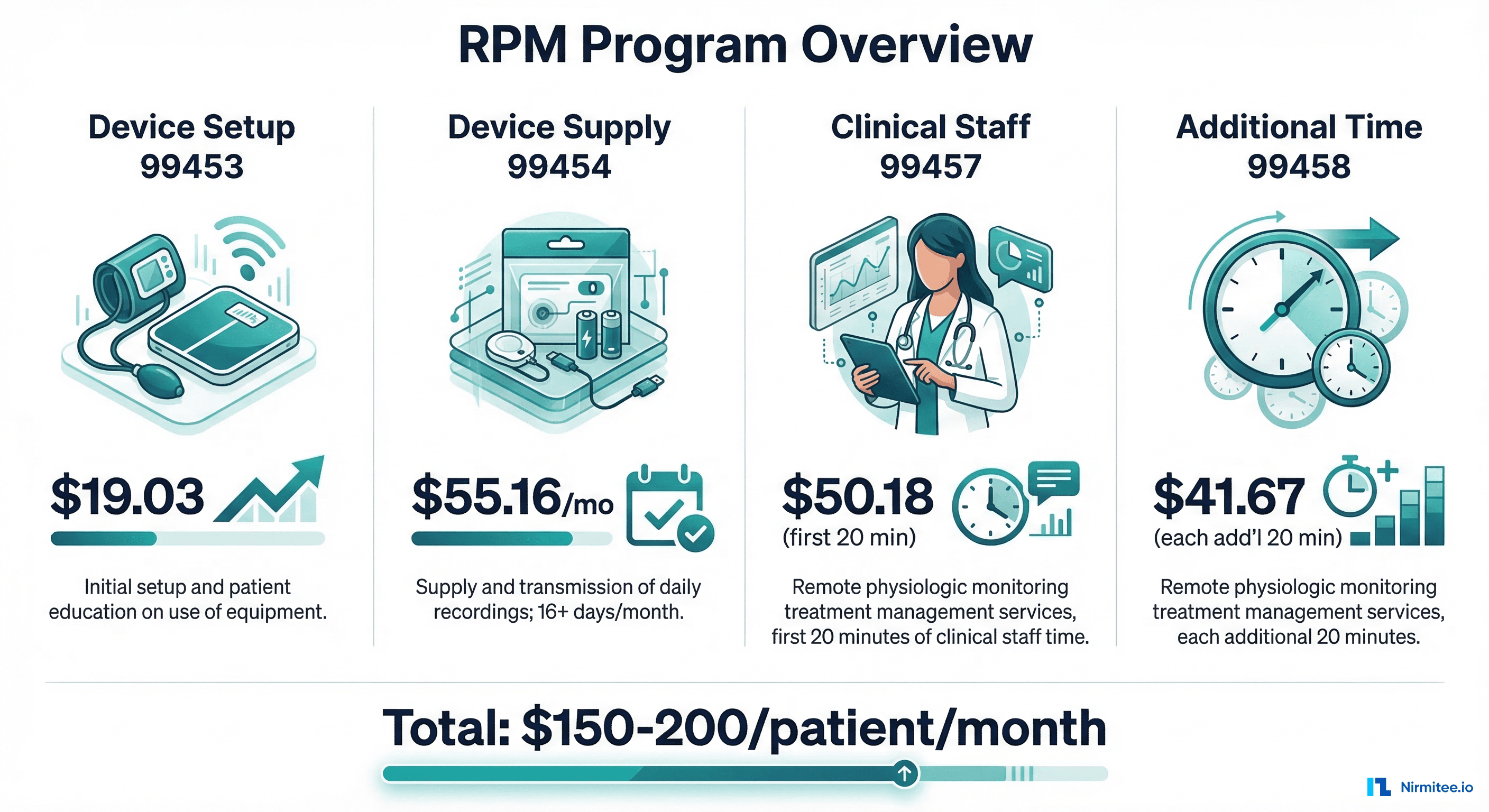
Remote Patient Monitoring (RPM): CPT 99453-99458 + New 2026 Codes
RPM covers the collection and clinical review of physiologic data transmitted from FDA-cleared medical devices. This includes blood pressure cuffs, glucose monitors, pulse oximeters, weight scales, and continuous glucose monitors (CGMs).
| CPT Code | Description | 2026 Rate | Frequency |
|---|---|---|---|
| 99453 | Initial device setup and patient education | $19.03 | Once per episode |
| 99454 | Device supply with daily recording/transmission (16+ days) | $55.16 | Monthly |
| 99457 | Clinical staff time — first 20 minutes | $51.90 | Monthly |
| 99458 | Clinical staff time — each additional 20 minutes | $41.52 | Monthly (up to 2x) |
| 99445 | NEW: Device supply/transmission for 2-15 days | ~$30 | Monthly |
| 99470 | NEW: Clinical review 10-19 minutes | ~$26 | Monthly |
Key 2026 change: The new CPT 99445 eliminates the previous 16-day minimum data transmission requirement. Practices can now bill RPM with as few as 2 days of patient data in a 30-day period, significantly expanding the eligible patient population. CPT 99470 fills the gap for encounters where clinical review takes 10-19 minutes — previously unbillable time.
Monthly RPM revenue per patient: $55.16 (99454) + $51.90 (99457) + $41.52 (99458) = $148.58-$190.10/month
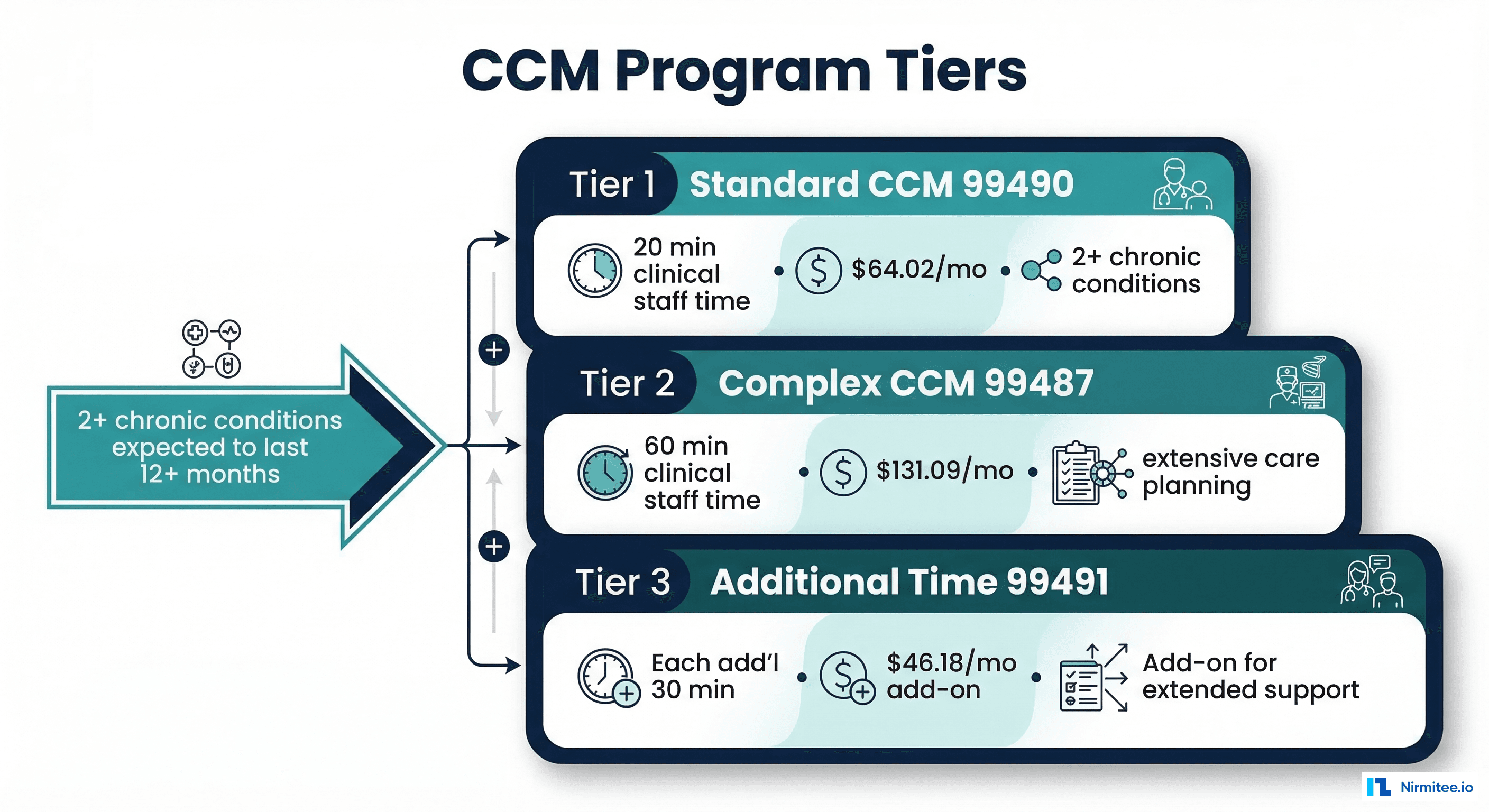
Chronic Care Management (CCM): CPT 99490, 99491, 99437, 99439
CCM covers non-face-to-face care coordination for patients with two or more chronic conditions expected to last at least 12 months. This includes care plan development, medication reconciliation, coordination with specialists, and patient/caregiver communication.
| CPT Code | Description | 2026 Rate | Time Requirement |
|---|---|---|---|
| 99490 | Standard CCM — clinical staff time | $66.30 | 20 minutes/month |
| 99439 | Each additional 20 min of clinical staff time | $48.12 | Additional 20 min (up to 2x) |
| 99491 | CCM by physician/QHP personally | $93.40 | 30 minutes/month |
| 99437 | Each additional 30 min by physician/QHP | $68.25 | Additional 30 min |
| 99487 | Complex CCM — clinical staff time | $131.09 | 60 minutes/month |
| 99489 | Each additional 30 min complex CCM | $68.25 | Additional 30 min |
Eligibility: Patient must have 2+ chronic conditions (e.g., diabetes + hypertension, COPD + CHF), must consent to CCM services, and must have a comprehensive care plan. Complex CCM (99487) requires substantially more clinical staff time and moderate-to-high complexity medical decision-making.
Monthly CCM revenue per patient: $66.30 (99490) + $48.12 (99439) = $66.30-$114.42/month (standard) or $131.09-$199.34/month (complex)
Remote Therapeutic Monitoring (RTM): CPT 98975-98981
RTM covers non-physiologic data monitoring — specifically medication adherence, therapeutic response, and musculoskeletal/respiratory treatment outcomes. Unlike RPM's physiologic data (vitals), RTM tracks therapeutic data like pain levels, medication side effects, inhaler usage, and range-of-motion measurements.
| CPT Code | Description | 2026 Rate | Frequency |
|---|---|---|---|
| 98975 | Initial setup and patient education | $17.56 | Once per episode |
| 98976 | Device supply — respiratory system | $51.42 | Monthly |
| 98977 | Device supply — musculoskeletal system | $51.42 | Monthly |
| 98980 | Treatment management — first 20 minutes | $54.24 | Monthly |
| 98981 | Treatment management — each additional 20 min | $41.67 | Monthly |
RTM vs RPM distinction: RPM monitors physiologic data (blood pressure, glucose, SpO2). RTM monitors therapeutic data (medication adherence, symptom surveys, treatment response). A patient using a blood pressure cuff is RPM; a patient logging daily pain scores after knee replacement is RTM. Both can be billed for the same patient because they track fundamentally different data types.
Monthly RTM revenue per patient: $51.42 (98976/98977) + $54.24 (98980) = $105.66/month

Advanced Primary Care Management (APCM): G0556-G0558 (New 2026)
APCM is a new bundled payment model for 2026 that combines CCM, Principal Care Management (PCM), Transitional Care Management (TCM), and certain virtual communication services into a single monthly payment. APCM uses HCPCS G-codes rather than CPT codes.
| HCPCS Code | Description | 2026 Rate | Eligibility |
|---|---|---|---|
| G0556 | APCM — low complexity | ~$80/month | 1 chronic condition |
| G0557 | APCM — moderate complexity | ~$100/month | 2+ chronic conditions |
| G0558 | APCM — high complexity | ~$120/month | 2+ chronic conditions + high complexity |
| G0568-G0570 | APCM Behavioral Health add-ons | ~$30-50/month | Co-occurring BH condition |
Critical stacking rule: APCM and CCM are mutually exclusive — you cannot bill both for the same patient in the same month. APCM bundles CCM services into its payment. However, APCM + RPM is allowed, and APCM + RTM is allowed. Evaluate whether APCM or CCM yields higher revenue per patient based on complexity.
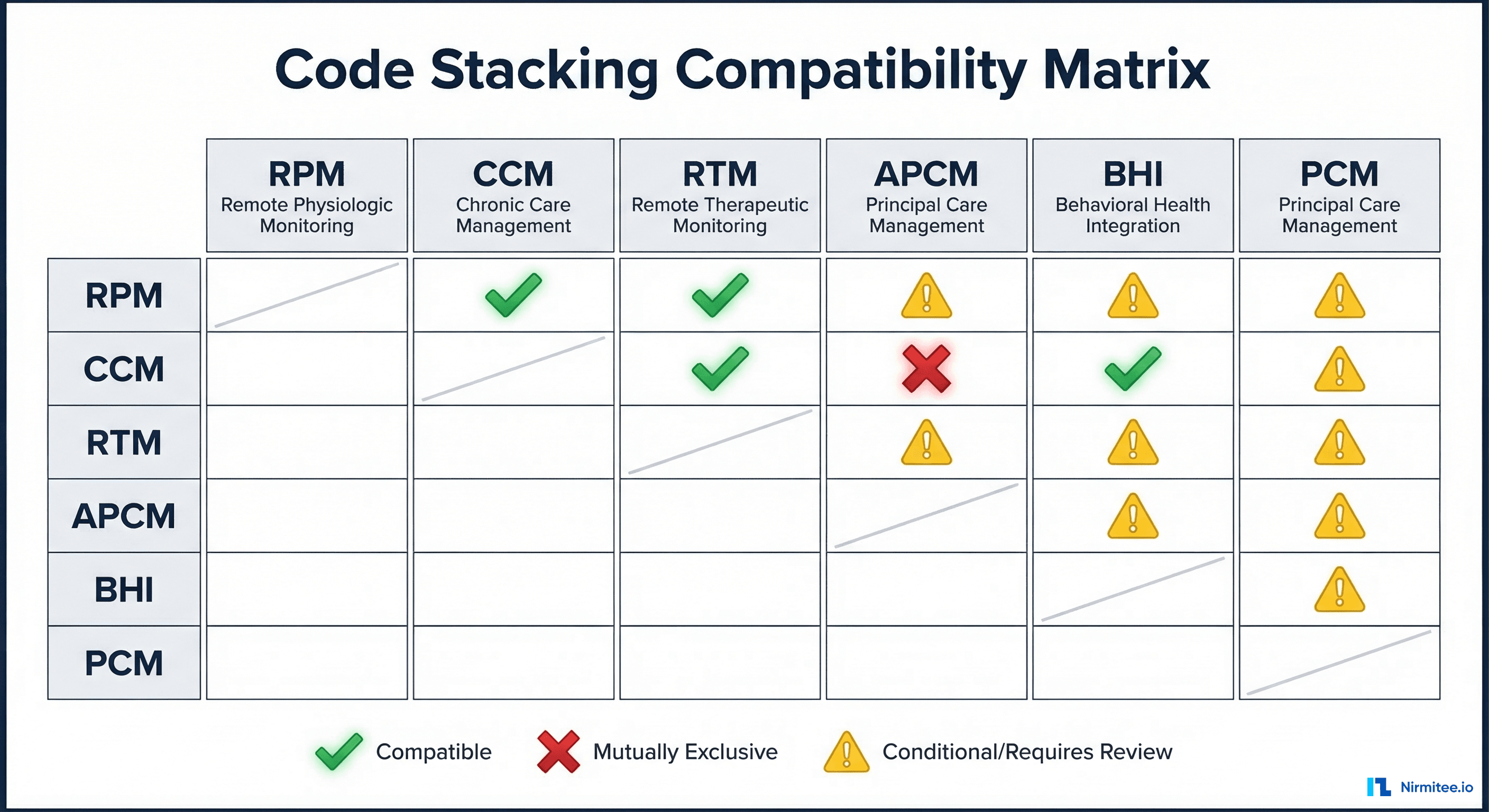
The Complete Code Stacking Compatibility Matrix
Not all programs can be billed together. The following matrix shows which combinations are CMS-compliant for same-patient, same-month billing:
| Combination | Allowed? | Rationale |
|---|---|---|
| RPM + CCM | Yes | Different services: device monitoring vs care coordination |
| RPM + RTM | Yes | Different data types: physiologic vs therapeutic |
| CCM + RTM | Yes | Different services: care coordination vs therapeutic monitoring |
| RPM + CCM + RTM | Yes | Maximum stack — all three serve distinct purposes |
| CCM + APCM | No | APCM bundles CCM — mutually exclusive |
| RPM + APCM | Yes | RPM is device-based; APCM is care management |
| CCM + PCM | No | Cannot bill both in same month for same patient |
| RPM + BHI | Yes | Different clinical domains: physiologic vs behavioral |
| CCM + BHI | Yes | BHI addresses behavioral health; CCM addresses chronic conditions |
| RPM + CCM + RTM + BHI | Yes | Full stack for qualifying patients (~$450+/month) |
Compliance rule: Time spent on one program cannot be counted toward another. If a nurse spends 20 minutes reviewing RPM data (99457), that same 20 minutes cannot be billed as CCM time (99490). Document time separately for each program with distinct clinical notes.
Revenue Per Patient — Code Stacking Calculator
The financial impact of code stacking compounds across your patient panel. Here is a detailed revenue breakdown for common stacking scenarios:

| Scenario | Monthly/Patient | 100 Patients/Year | 250 Patients/Year | 500 Patients/Year |
|---|---|---|---|---|
| RPM Only | $148 | $177,600 | $444,000 | $888,000 |
| RPM + CCM (Standard) | $214 | $256,800 | $642,000 | $1,284,000 |
| RPM + CCM (Complex) | $280 | $336,000 | $840,000 | $1,680,000 |
| RPM + CCM + RTM | $360 | $432,000 | $1,080,000 | $2,160,000 |
| RPM + CCM + RTM + BHI | $450+ | $540,000+ | $1,350,000+ | $2,700,000+ |
Revenue impact: Moving from single-program RPM to full RPM+CCM+RTM stacking represents a 143% increase in per-patient revenue. For a practice with 250 patients, that is an additional $636,000 in annual revenue from the same patient population. These are Medicare rates — commercial payer rates are typically 20-40% higher.
Patient Eligibility — Who Qualifies for Multiple Programs?
Not every patient qualifies for every program. Here is a decision framework for determining which programs each patient is eligible for:
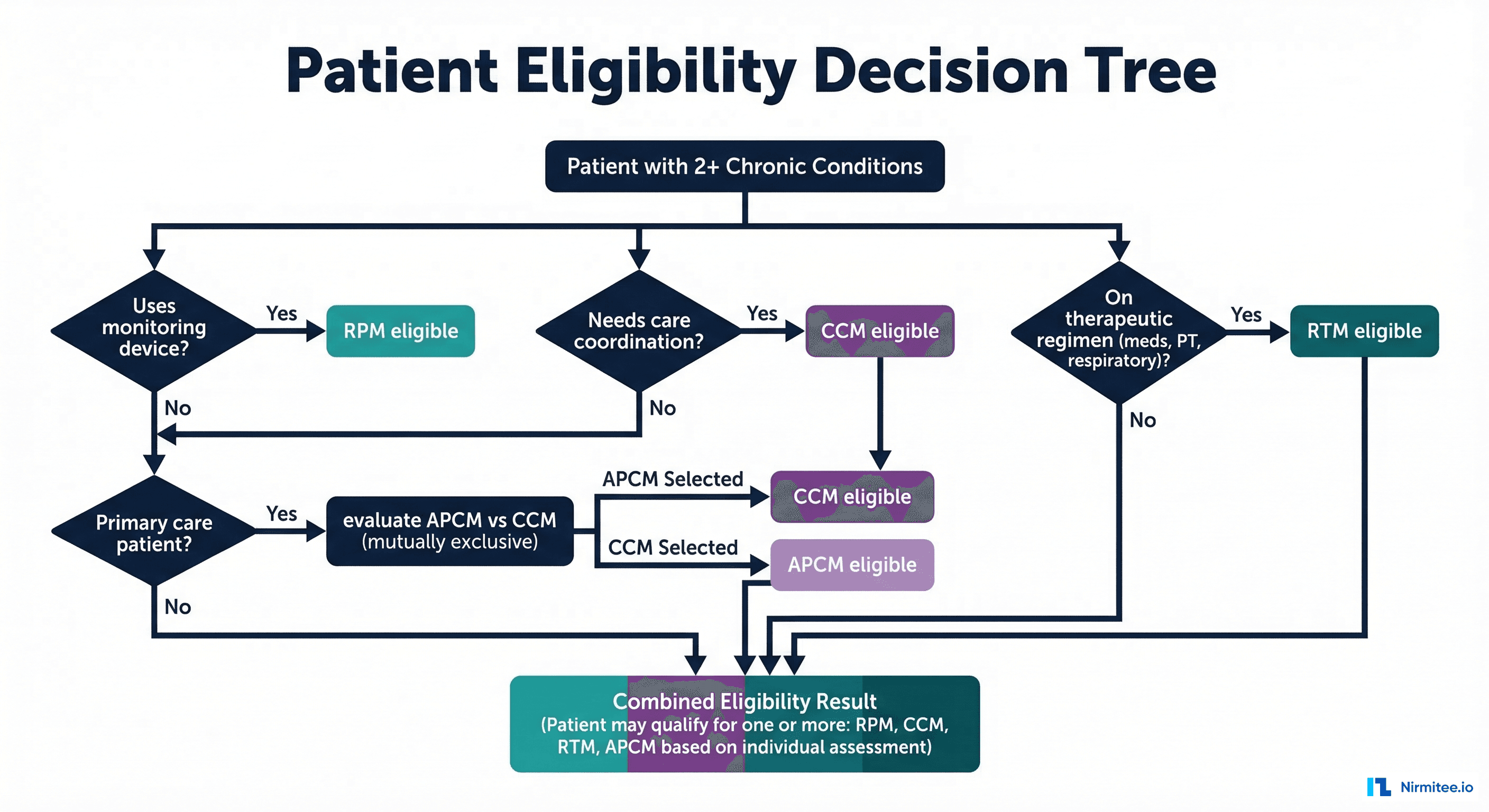
RPM Eligibility Criteria
- Patient has a chronic condition requiring physiologic monitoring (hypertension, diabetes, CHF, COPD)
- Physician orders RPM services
- Patient uses an FDA-cleared monitoring device
- Data transmitted at least 2 days per 30-day period (2026 rule via CPT 99445) or 16+ days for full reimbursement (99454)
- Patient consents to RPM services
CCM Eligibility Criteria
- Patient has 2 or more chronic conditions expected to last at least 12 months
- Conditions place patient at significant risk of death, acute exacerbation, or functional decline
- Comprehensive care plan established and maintained
- Patient consent obtained (verbal or written)
- 24/7 access to care management services
RTM Eligibility Criteria
- Patient is on a therapeutic regimen: medications, physical therapy, respiratory therapy, or musculoskeletal treatment
- Patient uses a monitoring device or app to report therapeutic data (pain scores, medication adherence, inhaler usage, range of motion)
- Data transmitted at least 16 days per 30-day period
- Monitoring is for a therapeutic purpose (not physiologic — that is RPM)
Sample Qualifying Patient Profile
Consider a 68-year-old Medicare beneficiary with Type 2 diabetes (E11.9), hypertension (I10), COPD (J44.1), and chronic knee pain (M17.11) post-arthroplasty. This patient qualifies for:
- RPM: Blood pressure cuff + CGM for physiologic monitoring of hypertension and diabetes
- CCM: 2+ chronic conditions requiring ongoing care coordination between endocrinologist, pulmonologist, and PCP
- RTM: Medication adherence tracking (insulin, antihypertensives) + post-surgical range-of-motion monitoring for knee
Combined monthly revenue: $148 (RPM) + $114 (CCM) + $106 (RTM) = $368/month or $4,416/year from one patient.
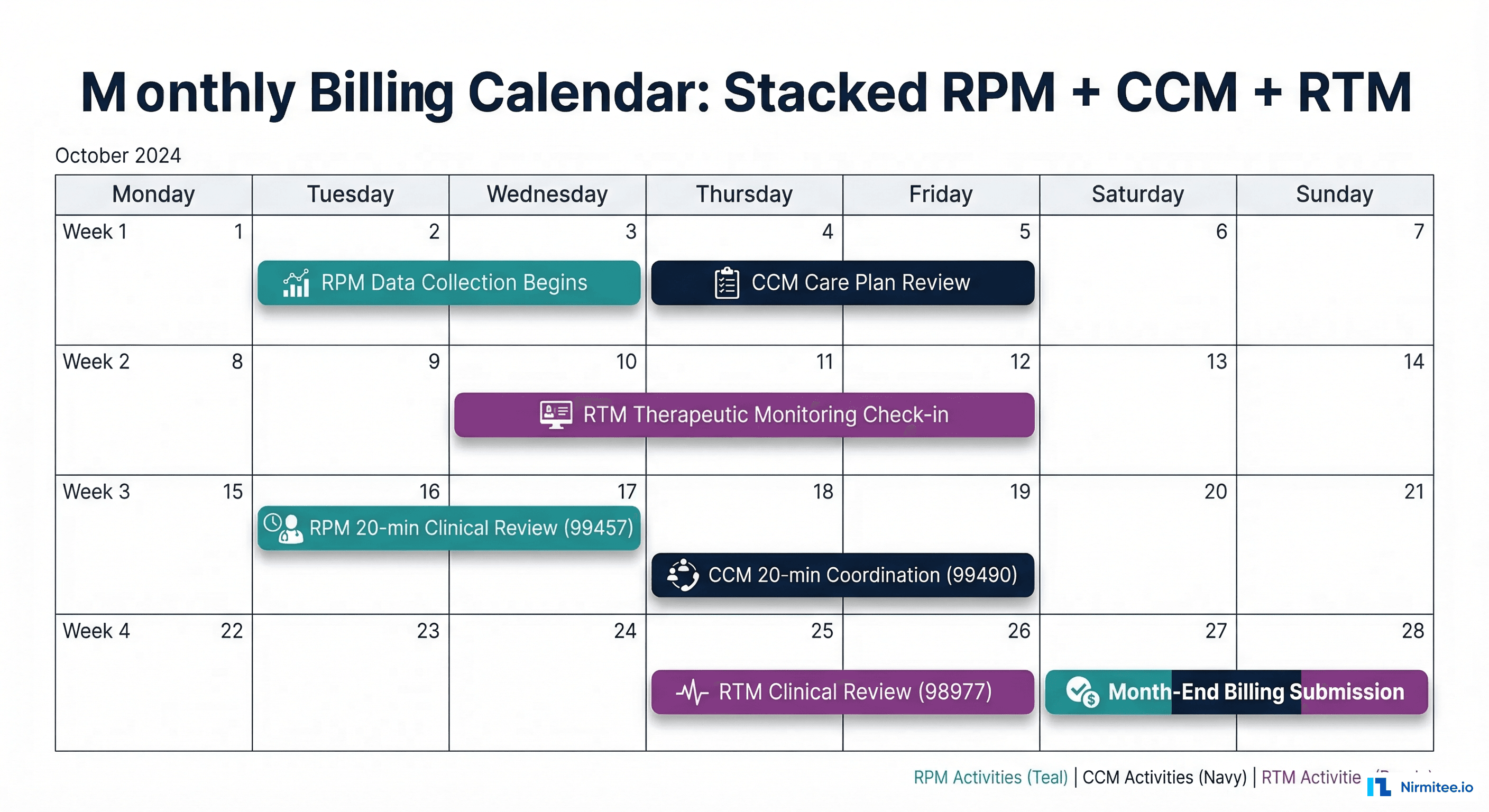
Monthly Billing Calendar — Coordinating Stacked Programs
Successful code stacking requires careful documentation and time tracking throughout the month. Consider this: sample billing calendar for a patient enrolled in RPM + CCM + RTM:
MONTH: [Any 30-Day Period]
═══════════════════════════════════════════════════════════════
WEEK 1 (Days 1-7)
RPM: Patient transmits BP + glucose readings daily (auto)
CCM: Review care plan, update medication list (10 min)
RTM: Patient completes medication adherence survey (auto)
WEEK 2 (Days 8-14)
RPM: Continue daily vitals transmission
CCM: Coordinate with endocrinologist re: HbA1c results (5 min)
RTM: Review therapeutic response data, adjust protocol (10 min)
WEEK 3 (Days 15-21)
RPM: 20-min clinical review of physiologic data trends (99457)
CCM: Patient phone call, medication reconciliation (5 min)
RTM: Continue therapeutic data collection
WEEK 4 (Days 22-30)
RPM: Additional 20-min review if needed (99458)
CCM: Document care coordination activities, total 20+ min (99490)
RTM: 20-min treatment management review (98980)
BILLING: Submit claims — 99454+99457+99458, 99490, 98976+98980
═══════════════════════════════════════════════════════════════
Documentation Requirements for Compliant Stacking
The single biggest risk in code stacking is an audit finding that time was double-counted across programs. Follow these documentation requirements to maintain compliance:
Time Tracking Separation
DOCUMENTATION TEMPLATE — STACKED SERVICES
══════════════════════════════════════════
Patient: [Name] DOS: [Date] MRN: [Number]
RPM Documentation (99457 — 20 minutes)
Start: 10:00 AM End: 10:20 AM
Activity: Reviewed 22 days of BP data (avg 142/88 trending down),
glucose readings (fasting avg 134, post-prandial avg 178),
weight stable at 198 lbs.
Clinical Decision: BP medication titration effective, continue current dose.
Data Source: Omron BP cuff, Dexcom G7 CGM
CCM Documentation (99490 — 20 minutes)
Start: 10:25 AM End: 10:45 AM
Activity: Updated care plan, coordinated with Dr. Smith (cardiology)
re: upcoming stress test. Called pharmacy to resolve insulin
prior authorization. Patient education on dietary sodium.
Care Plan Updated: Yes — added cardiology follow-up 4/15
RTM Documentation (98980 — 20 minutes)
Start: 2:00 PM End: 2:20 PM
Activity: Reviewed medication adherence data (92% compliant this month),
patient-reported pain scores (avg 4/10, down from 6/10),
inhaler usage logs (2x daily as prescribed).
Therapeutic Assessment: Medication regimen effective, no changes needed.
Data Source: MedMinder app, patient symptom survey
══════════════════════════════════════════
Key Compliance Rules
- Separate time entries: Each program must have distinct start/end times — no overlapping time windows
- Distinct activities: RPM = device data review; CCM = care coordination; RTM = therapeutic response assessment
- Separate clinical notes: Document each service in its own note section or template
- Patient consent: Obtain consent for each program separately — a single blanket consent is insufficient
- Initiating visit: RPM requires a face-to-face or telehealth initiating visit; CCM requires an AWV, IPPE, or E/M visit; RTM requires a qualifying visit
APCM vs CCM — Which Generates More Revenue?
The introduction of APCM (G0556-G0558) in 2026 creates a strategic decision for practices already billing CCM. Since APCM and CCM are mutually exclusive, you must choose one per patient per month. Below is comparison framework:
| Factor | CCM (99490/99487) | APCM (G0556-G0558) |
|---|---|---|
| Monthly Revenue | $66-$199 (varies by complexity) | $80-$120 (fixed tiers) |
| Time Tracking | Must track exact minutes | Bundled — no minute tracking |
| Stacks with RPM? | Yes | Yes |
| Stacks with RTM? | Yes | Yes |
| Administrative Burden | Higher — time documentation | Lower — flat monthly payment |
| Best For | Complex patients (99487 = $131+) | Standard-complexity patients |
Recommendation: Use CCM (99487) for high-complexity patients where documented time exceeds 60 minutes — the $131+ reimbursement beats APCM's $120 cap. Use APCM for moderate-complexity patients where the administrative simplicity and guaranteed monthly payment outweigh CCM's variable reimbursement. Many practices will use a hybrid approach: APCM for the majority of patients, CCM for the highest-complexity cases.
Implementation Roadmap — Launching a Code Stacking Program
Implementing code stacking requires changes to clinical workflows, EHR documentation, billing processes, and staff training. Follow this phased approach:
Phase 1: Patient Panel Analysis (Weeks 1-2)
- Run EHR query: all patients with 2+ chronic conditions on active medication regimens
- Cross-reference with current RPM enrollment — identify patients already on RPM who could add CCM/RTM
- Prioritize patients by revenue potential: RPM+CCM+RTM eligible patients first
- Target: identify 50-100 patients for initial stacking program
Phase 2: Workflow and Documentation Setup (Weeks 3-4)
- Create separate EHR documentation templates for RPM, CCM, and RTM
- Configure time-tracking tools with program-specific categories
- Develop consent forms for each program (cannot use a single consent)
- Train clinical staff on time separation requirements
Phase 3: Patient Enrollment and Billing (Weeks 5-8)
- Obtain consent for additional programs during patient touchpoints
- Configure billing system for multi-program claims submission
- Submit first stacked claims and monitor for denials
- Adjust documentation based on payer feedback
Phase 4: Scale and Optimize (Weeks 9-12+)
- Expand to full eligible patient panel
- Monitor per-patient revenue against targets
- Audit documentation quarterly for compliance
- Evaluate APCM vs CCM split based on first quarter data
Technology Requirements for Code Stacking
Effective code stacking requires technology that can manage multiple programs per patient simultaneously. Key platform requirements include:
- Multi-program enrollment tracking: Ability to tag patients with RPM, CCM, RTM, and APCM enrollment status
- Separate time tracking: Program-specific timers that prevent overlapping time entries across RPM, CCM, and RTM
- FHIR-based EHR integration: Push documentation to EHR using FHIR interoperability standards — CarePlan resources for CCM, Observation resources for RPM, and DocumentReference for clinical notes
- Automated eligibility screening: Flag patients who qualify for additional programs based on diagnosis codes, medication lists, and device usage. AI-driven clinical decision support can automate this screening at scale
- Multi-program billing engine: Generate separate claims for each program with proper documentation linkage
- Compliance dashboard: Real-time visibility into time tracking, consent status, and documentation completeness per program per patient
Building a platform that handles multi-program remote care requires deep expertise in healthcare technology stack selection and EHR integration architecture.
Common Billing Mistakes That Trigger Audits
- Double-counting time: Using the same 20-minute block for both RPM (99457) and CCM (99490). Each program requires separate, non-overlapping time entries.
- Missing initiating visits: Billing RPM without a documented face-to-face or telehealth initiating visit within the billing period.
- Insufficient data days: Billing 99454 when patient transmitted data fewer than 16 days (use 99445 for 2-15 days instead).
- Stacking mutually exclusive codes: Billing CCM + APCM or CCM + PCM for the same patient in the same month.
- Missing consent documentation: Failing to obtain and document separate consent for each program.
- Upcoding complexity: Billing complex CCM (99487) when clinical documentation does not support moderate-to-high complexity medical decision-making.
- Inadequate care plans: CCM requires a comprehensive, documented, regularly-updated care plan — not just a problem list.
Frequently Asked Questions
Can I bill RPM and CCM for the same patient on the same day?
Yes. RPM and CCM can be billed for the same patient in the same calendar month, and activities can occur on the same day — as long as the time and services are documented separately. RPM covers device data review; CCM covers care coordination and care plan management. These are distinct clinical activities.
What is the maximum revenue per patient with code stacking?
The theoretical maximum using RPM + Complex CCM + RTM + BHI is approximately $450-500+ per month ($5,400-6,000/year). However, this requires the patient to genuinely qualify for all programs and the practice to deliver and document all required services. Most practices achieve $280-360/month for triple-stacked patients.
Do I need separate consent for each program?
Yes. CMS requires separate patient consent for RPM, CCM, and RTM services. A single blanket consent is not sufficient. Each consent must explain the specific services, cost-sharing responsibilities, and the patient's right to revoke consent at any time. Consent can be obtained verbally but must be documented in the medical record.
Can clinical staff (RNs, MAs) bill these codes, or must it be a physician?
RPM (99457/99458), standard CCM (99490/99439), and RTM (98980/98981) can be billed for clinical staff time under general physician supervision. Physician/QHP-specific codes (99491, 99437) require the billing practitioner's personal time. This makes code stacking highly scalable — a single physician can oversee multiple clinical staff members managing stacked programs for hundreds of patients.
How does APCM affect existing CCM programs?
APCM (G0556-G0558) is a new alternative to CCM introduced in 2026. It bundles CCM, PCM, TCM, and virtual communication services into a single monthly payment. APCM simplifies billing (no time tracking required) but caps reimbursement at approximately $120/month. Practices currently billing complex CCM ($131+/month) should continue using CCM for high-complexity patients. APCM is better suited for moderate-complexity patients where administrative simplicity is valued.
Is code stacking legal and compliant?
Yes. CMS explicitly allows billing multiple remote care programs for the same patient when each program's requirements are independently met. The key compliance requirements are: (1) separate time documentation, (2) distinct clinical activities, (3) individual patient consent per program, and (4) no double-counting of time or services. The CMS Chronic Care Management MLN Booklet and the Medicare Physician Fee Schedule provide authoritative guidance on concurrent billing.
Conclusion — Code Stacking Is a Revenue Imperative
In 2026, the combination of increased reimbursement rates, new CPT codes (99445, 99470), and the introduction of APCM makes remote care revenue optimization more accessible than ever. Practices that continue billing single-program RPM are leaving 50-140% of potential revenue uncaptured.
The implementation path is straightforward: analyze your patient panel for multi-program eligibility, set up separate documentation workflows, train clinical staff on time separation, and submit stacked claims. With 250 patients, the difference between RPM-only and full code stacking is over $600,000 in annual revenue.
For practices ready to build or upgrade their custom RPM platform to support multi-program code stacking, the technical architecture must include FHIR-based data exchange, program-specific time tracking, automated eligibility screening, and multi-program billing capabilities. Nirmitee's RPM solutions are designed to handle exactly these requirements — enabling compliant, high-revenue remote care at scale.