There is a paradox at the center of healthcare integration: the systems that move patient data between hospitals, labs, pharmacies, and payers are mission-critical infrastructure, yet the people who build and maintain those systems are among the hardest to find, hire, and retain in all of healthcare IT. The average time to fill a niche healthcare integration role is 60 to 90 days, according to healthcare staffing firm data, and that number assumes you know what you are looking for in the first place.
Mirth Connect is the most widely deployed open-source integration engine in healthcare, powering HL7 and FHIR data flows for thousands of hospitals and health systems worldwide. But "Mirth Connect engineer" does not appear on most computer science curricula. It is not a job title that recruiters understand intuitively. And the intersection of Java development skills, healthcare domain knowledge, and integration architecture expertise makes the talent pool extremely small.
This playbook is for IT directors, hiring managers, and team leads who need to build or grow a healthcare integration team. It covers everything from writing effective job descriptions to structured training programs, from interview questions that actually reveal capability to retention strategies that keep your best engineers from leaving. Whether you are building a team of 3 or scaling to 15, the principles here will help you find the right people, develop them effectively, and keep them engaged for the long term.
The Talent Shortage Reality
Healthcare integration engineering sits at the intersection of three specialized domains, and that intersection is where talent scarcity begins.
According to the Bureau of Labor Statistics, software developer employment is projected to grow 25% from 2022 to 2032, much faster than the average for all occupations. But healthcare integration is a subset of that growth with far fewer qualified practitioners. The number of engineers who understand both HL7 messaging standards and modern cloud deployment can be measured in thousands globally, not millions.
Integration engineer salaries reflect this scarcity. In the United States, experienced Mirth Connect engineers command $120,000 to $180,000 per year, with senior architects and team leads exceeding $200,000 in major metropolitan areas. Training a new engineer from adjacent skills to full productivity takes 3 to 6 months, a significant investment that makes retention as important as recruitment.
The talent pool is small for several reasons. Healthcare integration is not taught in universities. Most engineers discover it accidentally, coming from Java development, database administration, or clinical informatics backgrounds. The interoperability standards landscape is complex, spanning HL7 v2, HL7 FHIR, CDA, X12, and proprietary formats, and mastering even one standard takes months of hands-on work.
What Makes a Great Integration Engineer
The best integration engineers are not the best coders. They are the best problem solvers who happen to code. Healthcare integration is fundamentally a translation problem: taking data from System A, which speaks one language, and delivering it to System B, which speaks another, while preserving clinical meaning, handling edge cases, and maintaining regulatory compliance.
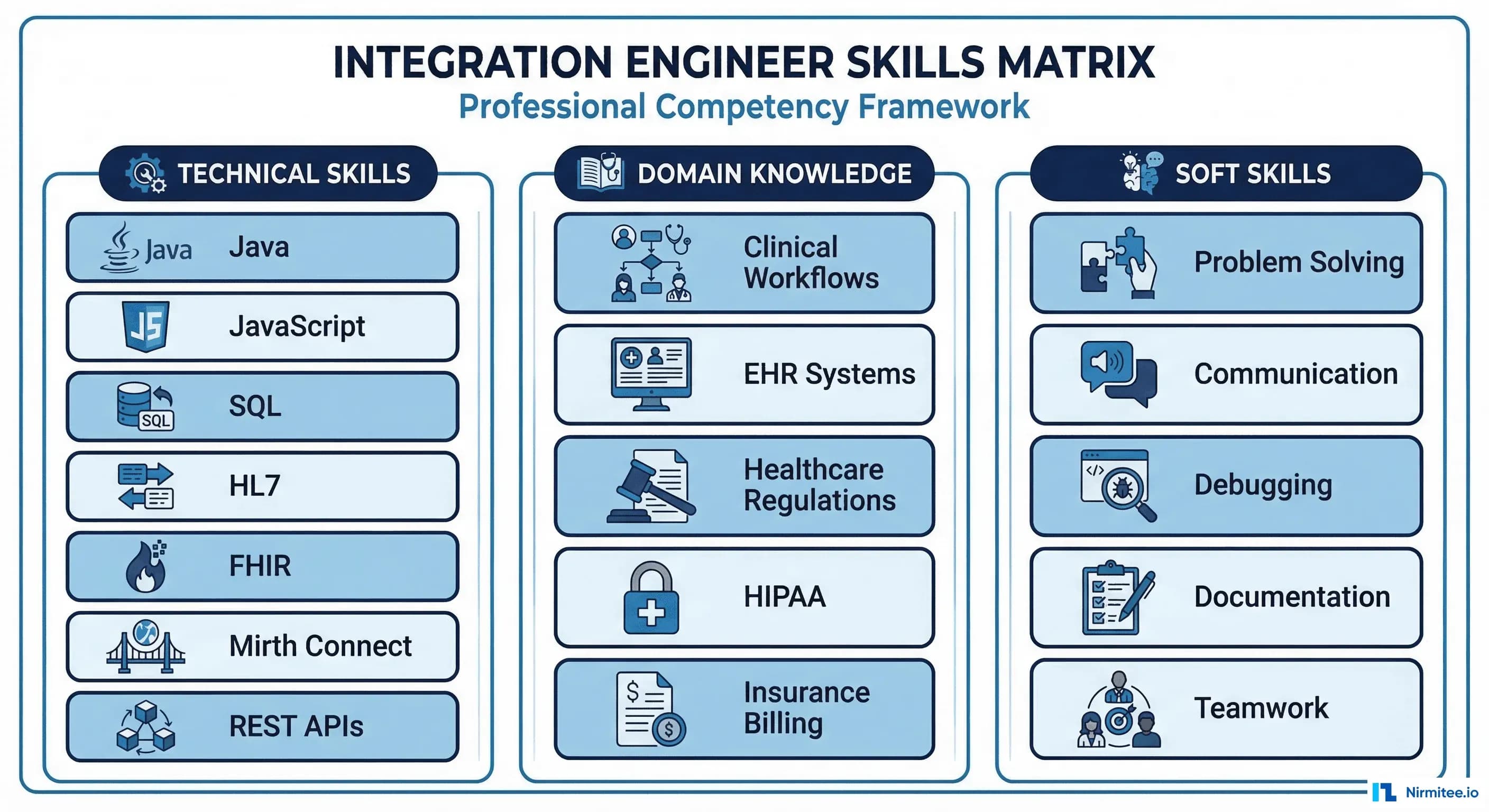
Technical Skills
- Java and JavaScript proficiency: Mirth Connect uses JavaScript (Rhino engine) for channel transformers and Java for custom extensions. Engineers need fluency in both.
- HL7 v2 message structure: Understanding segments, fields, components, and repetition separators. Being able to read an ADT^A01 message and identify every clinical data element.
- SQL and database skills: Many integration channels read from or write to databases. Proficiency in PostgreSQL and SQL Server is common.
- API and web services: REST APIs, SOAP, FHIR endpoints, OAuth 2.0 authentication. Modern integrations increasingly use FHIR APIs alongside traditional HL7.
- Networking fundamentals: TCP/IP, MLLP protocol, TLS configuration, firewall rules, VPN connectivity.
Domain Knowledge
- Clinical workflows: Understanding how patient registration, lab ordering, result delivery, and discharge processes work in a hospital.
- EHR system familiarity: How Epic, Cerner (Oracle Health), Meditech, and other EHR systems expose and consume data.
- Regulatory awareness: HIPAA requirements for data in transit and at rest, Meaningful Use / Promoting Interoperability requirements, state-level reporting mandates.
Soft Skills That Matter Most
- Debugging mindset: Integration work is 60% debugging. The ability to trace a message through multiple systems, identify where transformation logic went wrong, and fix it under pressure is the single most valuable skill.
- Communication: Engineers must translate between clinical users who say "the lab results are wrong" and technical teams who need "the OBX-5 value mapping for LOINC code 2160-0 is returning the wrong unit."
- Documentation discipline: Every interface has specifications, mapping documents, and operational runbooks. Engineers who document well reduce the team's bus factor.
What to Look for in Candidates
The hiring funnel for integration engineers is steep. From 200 applicants, you will typically screen 50, technically assess 20, interview 10, and extend offers to 2-3. Understanding what to prioritize at each stage saves enormous time.
Must-Have Qualifications
- 3+ years of software development experience (Java, JavaScript, or Python)
- Experience with at least one integration engine, ESB, or ETL tool
- Basic understanding of healthcare data (HL7, FHIR, or clinical databases)
- SQL proficiency for database-driven integrations
Strong Differentiators
- Direct Mirth Connect experience (channel development, deployment, troubleshooting)
- HL7 v2 message parsing and transformation experience
- Experience supporting production healthcare interfaces
- NextGen Mirth Connect certification
- Familiarity with channel design patterns and architecture best practices
Job Description Template
An effective integration engineer job description should include these elements while avoiding common pitfalls:
Include: Specific technologies used (Mirth Connect, HL7 v2, FHIR), types of integrations (EHR, lab, pharmacy, payer), team size and reporting structure, on-call expectations, growth opportunities, salary range.
Avoid: Requiring 10+ years of Mirth experience (the tool has only been widely used for 12 years), listing every possible technology as "required," vague descriptions like "other duties as assigned," omitting salary range (candidates skip these listings).
Interview Questions That Actually Work
Standard coding interviews do not reveal integration engineering capability. Here are five scenario-based questions that do:
Question 1: The Broken ADT Feed
"A hospital reports that patient demographic updates from their EHR are not reaching the billing system. The ADT channel in Mirth shows messages as 'Sent,' but the billing system has stale data. Walk me through your troubleshooting process."
What you are looking for: A systematic debugging approach. Does the candidate check the message content (not just the status)? Do they verify the destination is actually receiving? Do they check for filtering logic that might be dropping A08 update messages while passing A01 admits?
Question 2: The Mapping Challenge
"You receive an HL7 ORM message from a lab system that uses local codes for test orders. The destination system requires LOINC codes. How would you implement this translation in Mirth Connect?"
What you are looking for: Knowledge of code translation tables, database lookup approaches, Code Template Libraries for reusable mapping functions, and error handling for unmapped codes.
Question 3: The Scale Problem
"Your Mirth instance processes 5,000 messages per hour during peak. The hospital is merging with another facility, and message volume will double. What would you evaluate and potentially change?"
What you are looking for: Understanding of Mirth performance tuning, database optimization, channel threading, queue management, and potentially high-availability architecture.
Question 4: The Security Incident
"You discover that your Mirth Connect admin interface is accessible from the internet with default credentials. What do you do immediately, and what is your remediation plan?"
What you are looking for: Incident response instincts. Immediate lockdown actions, credential rotation, audit log review, network security assessment, and a hardening plan.
Question 5: The Design Decision
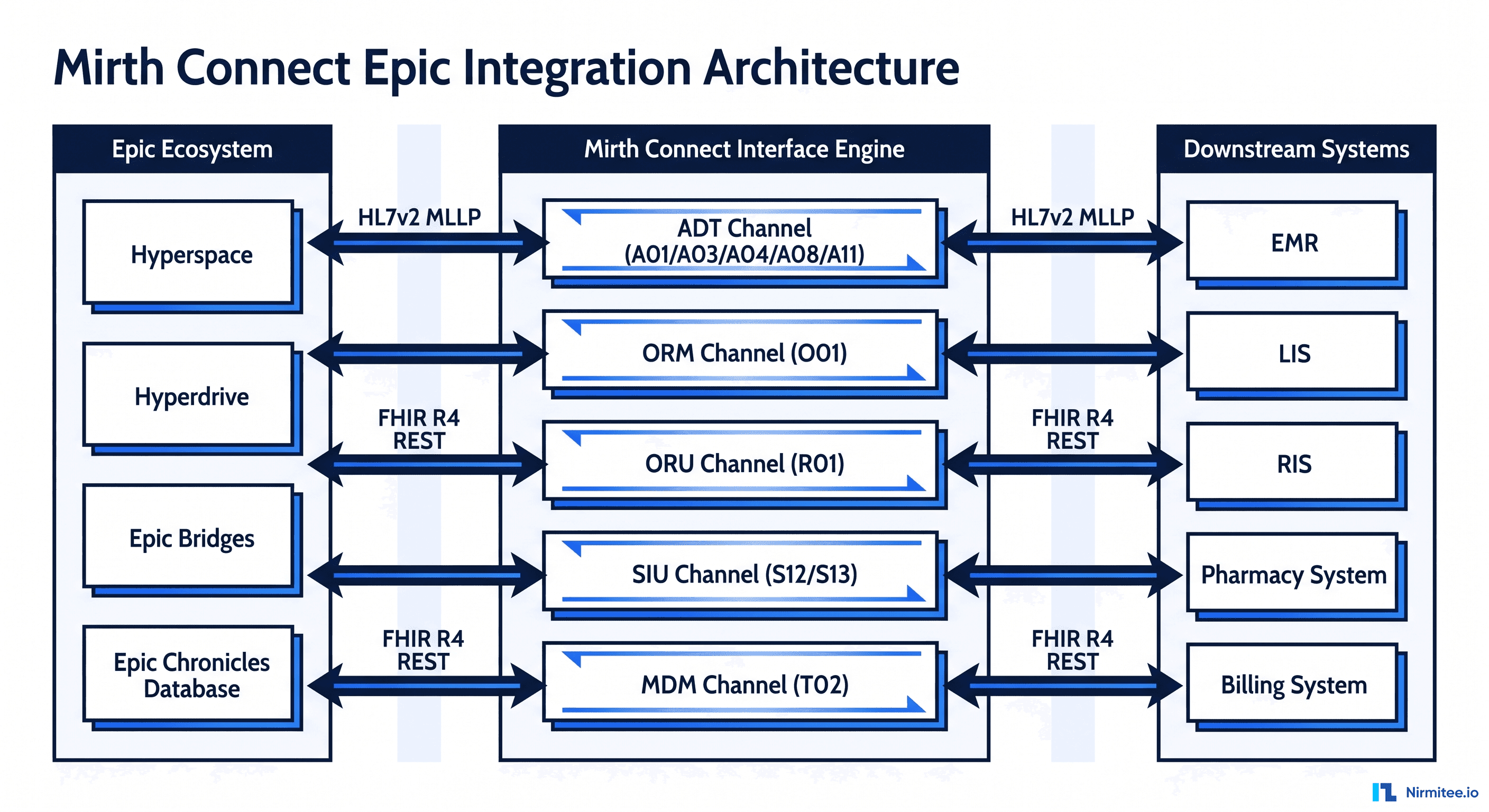
"You need to integrate a new FHIR-based patient portal with a legacy EHR that only speaks HL7 v2. Describe your high-level architecture for this integration."
What you are looking for: Understanding of bridging HL7 v2 and FHIR, API design thinking, data model mapping, and pragmatic architecture decisions.
The 6-Month Training Path for New Hires
Even experienced developers need structured onboarding for healthcare integration. This training path assumes a hire with strong Java/JavaScript skills but limited healthcare or Mirth experience.
Month 1-2: HL7 Standards and Mirth Connect Basics
- Week 1-2: HL7 v2 fundamentals. Message structure, common message types (ADT, ORM, ORU, SIU), segment definitions, data types. Read the HL7 v2 specification for ADT and ORM message types.
- Week 3-4: Mirth Connect fundamentals. Install locally, create the first channel, understand source/destination connectors, filters, and transformers. Complete NextGen's online training materials.
- Week 5-6: Build a simple ADT routing channel. Receive HL7 messages via MLLP, filter by message type, and route to appropriate destinations. Deploy to the dev environment.
- Week 7-8: Introduction to FHIR. RESTful APIs, FHIR resources (Patient, Encounter, Observation), JSON/XML formats. Build a simple FHIR endpoint in Mirth.
- Milestone: New hire can independently build and deploy a basic HL7 routing channel with transformer logic.
Month 3-4: Channel Development and Testing
- Week 9-10: Advanced transformer techniques. Code Template Libraries, database lookups, complex field mappings, and error handling patterns.
- Week 11-12: Work on a real production interface under mentorship. Pair with a senior engineer on an active project. Handle the mapping and transformation logic while the senior handles architecture decisions.
- Week 13-14: Testing practices. Unit testing transformer functions, integration testing with Docker, and building test message libraries. Reference the CI/CD testing guide for framework setup.
- Week 15-16: Monitoring and alerting. Understanding production monitoring, setting up alerts for channel errors, reading Mirth logs, and basic troubleshooting.
- Milestone: New hire can develop and test a moderately complex interface with guidance on architecture but independent of implementation.
Months 5-6: Production Support and Advanced Patterns
- Week 17-18: On-call shadowing. Join the on-call rotation as a secondary, shadowing the primary on-call engineer for incident response.
- Week 19-20: Advanced architecture patterns. Fan-out routing, message queuing, dead letter channels, Kafka integration for high-volume scenarios.
- Week 21-22: Performance tuning and optimization. Thread management, database optimization, batch processing, and handling message backlogs.
- Week 23-24: Independent project. Assign a new interface build from requirements gathering through production deployment. Senior engineer reviews architecture and code, but the new hire drives the project.
- Milestone: New hire is ready for independent on-call rotation and can architect and deliver new interfaces with minimal oversight.
Building from Adjacent Skills
Given the small pool of experienced Mirth engineers, many organizations build their teams by training professionals from adjacent domains. Here are the most successful transition paths:
Java Developers to Mirth Engineers
What they bring: Strong programming fundamentals, familiarity with the JVM ecosystem that Mirth runs on, experience with debugging and testing practices.
What they need: Healthcare domain knowledge, HL7 message structure, understanding of clinical workflows, MLLP protocol specifics.
Timeline to productivity: 3-4 months with structured training.
HL7 Analysts to Mirth Engineers
What they bring: Deep understanding of HL7 message structures, clinical workflows, interface specifications, and vendor communication.
What they need: Programming skills (JavaScript for Mirth transformers, SQL for database channels), Mirth Connect administration, deployment practices.
Timeline to productivity: 4-6 months, longer due to the coding skill gap.
Database Administrators to Mirth Engineers
What they bring: SQL expertise, data modeling skills, performance tuning experience, understanding of data integrity.
What they need: HL7 standards, JavaScript/Java programming, message-based integration concepts (versus batch/database integration).
Timeline to productivity: 4-5 months.
NextGen Certification and Training Options
NextGen Healthcare, the commercial steward of Mirth Connect, offers formal certification and training programs:
- Mirth Connect Fundamentals: Self-paced online course covering installation, channel creation, and basic configuration. Ideal for new hires in their first month.
- Mirth Connect Advanced: Covers complex transformations, performance tuning, and high-availability deployment. Best for engineers in months 3-4 of training.
- Mirth Connect Certification: Validates proficiency with Mirth Connect. While not universally required, it provides structured learning and a credential for career development.
Beyond NextGen's official offerings, valuable training resources include the Mirth Connect community forums, the open-source GitHub repository, and the growing ecosystem of healthcare integration content from practitioners sharing real-world patterns and solutions.
Team Structure by Organization Size
Small Team: 3 People (Community Hospital, Small Health System)
- Integration Lead / Senior Engineer: Architecture decisions, complex channel development, vendor communication, on-call primary.
- Integration Engineer: Channel development and maintenance, testing, documentation, on-call secondary.
- Junior Engineer / Analyst: Message mapping, testing, monitoring, documentation, learning channel development.
Key risk: Bus factor of 1 for architecture decisions. Mitigate with thorough documentation and cross-training.
Medium Team: 8 People (Regional Health System)
- Integration Manager: Team leadership, project prioritization, stakeholder management, budget.
- Senior Engineers (2): Architecture, complex interfaces, mentoring, on-call escalation.
- Mid-Level Engineers (3): Interface development and maintenance, production support, on-call rotation.
- QA / Test Engineer (1): Test automation, regression testing, test data management.
- Operations / DevOps (1): Mirth server management, monitoring, deployments, infrastructure.
Enterprise Team: 15 People (Large Health System, Multi-Hospital)
- Director of Integration: Strategy, budget, vendor relationships, cross-departmental leadership.
- Team Leads (2): One for inbound integrations, one for outbound. Technical leadership and mentoring.
- Integration Architects (2): Enterprise architecture, standards governance, technology evaluation.
- Senior Engineers (3): Complex interface development, technical mentoring, escalation support.
- Mid-Level Engineers (3): Interface development, maintenance, and on-call rotation.
- QA Engineers (2): Test automation, performance testing, compliance validation.
- DevOps Engineer (1): CI/CD pipelines, infrastructure automation, monitoring.
- Project Manager (1): Interface project coordination, vendor communication, timeline management.
Retention Strategies That Work
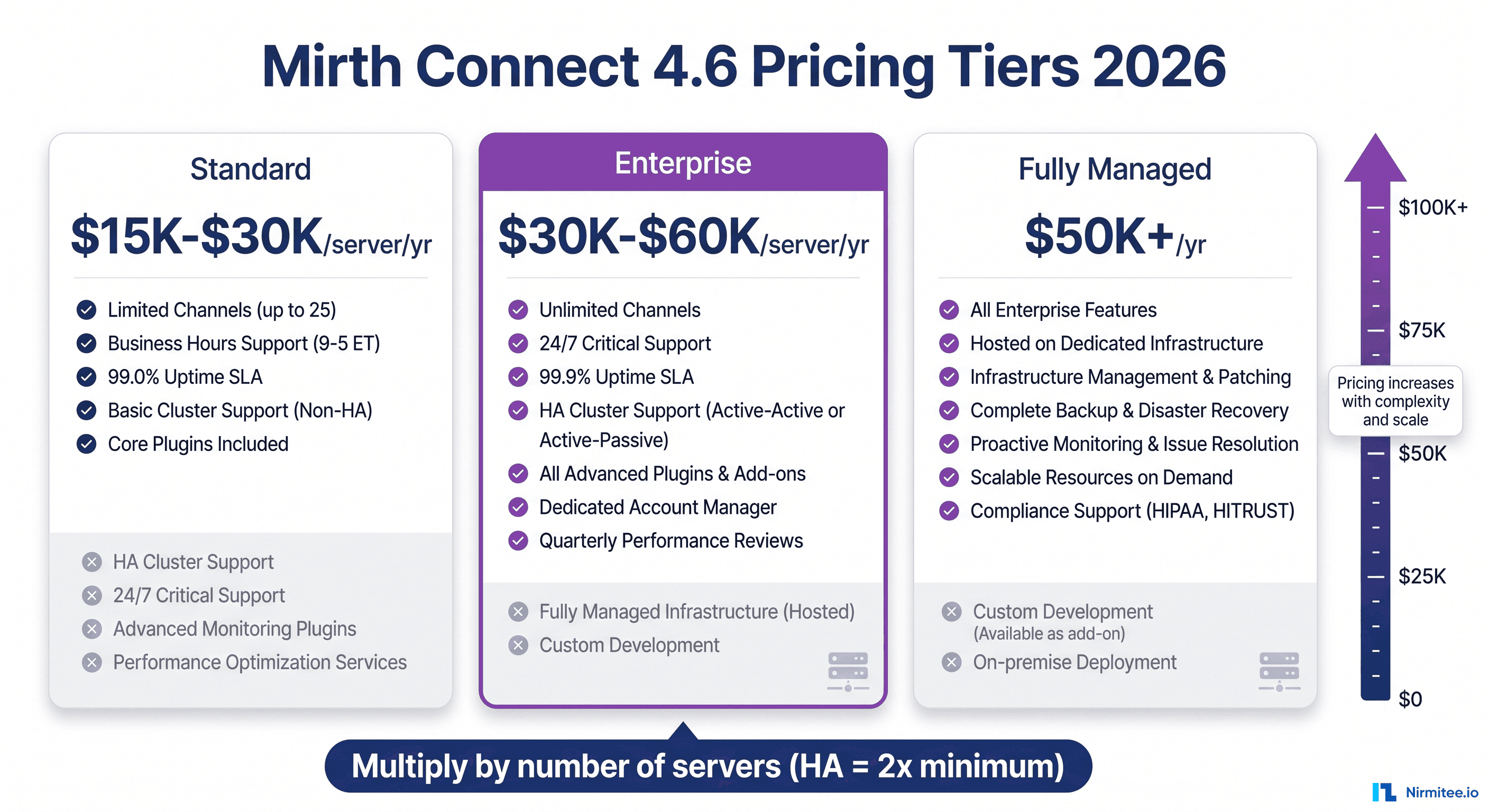
Hiring an integration engineer costs $15,000-$30,000 in recruiting fees and 3-6 months of reduced productivity during training. Retention is always cheaper than replacement. Here is what keeps integration engineers engaged:
Interesting Work
Engineers leave when work becomes repetitive. Rotate team members across different types of integrations. Let the senior engineer who has been maintaining ADT feeds for two years lead the new FHIR API project. Expose engineers to architecture decisions, not just implementation tasks.
Growth Paths
The career ladder for integration engineers should be clearly defined:
- Junior Integration Engineer (0-2 years): $70,000-$95,000. Learning standards, building channels under supervision.
- Integration Engineer (2-4 years): $95,000-$130,000. Independent channel development, production support.
- Senior Integration Engineer (4-7 years): $130,000-$170,000. Architecture decisions, mentoring, complex integrations.
- Lead / Staff Engineer (7-10 years): $160,000-$200,000. Technical leadership, cross-team standards, strategic direction.
- Integration Architect (8-12 years): $170,000-$220,000. Enterprise architecture, technology strategy, vendor evaluation.
- Director of Integration (10-15 years): $180,000-$250,000. Team leadership, budget, organizational strategy.
- VP of Engineering / Integration (15+ years): $220,000-$300,000+. Executive leadership, organizational transformation.
Competitive Compensation
Integration engineers know their skills are scarce. If your compensation falls below market by more than 10%, your best people will get recruited. Conduct annual salary benchmarking against healthcare IT salary surveys. Include retention bonuses for critical team members. Consider equity or profit-sharing where possible.
Avoiding On-Call Burnout
On-call duty is the number one cause of burnout in integration teams. Mitigate it with: rotation schedules that give at least 3 weeks off between on-call weeks, compensatory time off after heavy on-call periods, clear escalation paths so on-call engineers are not handling every issue alone, and investment in robust monitoring that reduces false alarms.
Professional Development Budget
Allocate $3,000-$5,000 per engineer annually for conferences, training, and certification. Relevant events include HIMSS, HL7 FHIR DevDays, and healthcare integration meetups. NextGen certification courses should be employer-funded as a baseline.
When to Outsource vs. Build In-House
Not every organization needs a full in-house integration team. Here is a framework for the decision:
Build in-house when:
- You have 20+ active interfaces requiring ongoing maintenance
- Integration is a core competency (you are a health system, HIE, or health IT vendor)
- You need 24/7 on-call support with fast response times
- Your interfaces involve complex, organization-specific business logic
- Regulatory requirements demand direct control over PHI-handling systems
Outsource when:
- You have fewer than 10 interfaces with low change frequency
- Integration is a supporting function, not a core competency
- You need to stand up interfaces quickly, but lack internal expertise
- Your budget supports project-based work but not full-time headcount
Hybrid approach: Many organizations maintain a small in-house team (2-3 engineers) for ongoing maintenance and monitoring while engaging specialized firms for new interface builds, migrations (like commercial transition migrations), and surge capacity during large projects like EHR implementations.
The Bottom Line
Building a healthcare integration team is a long game. The talent pool is small, training takes months, and the cost of turnover is high. But the organizations that invest in their integration teams, with structured hiring, systematic training, clear career paths, and competitive retention, build a strategic advantage that compounds over time.
Your integration infrastructure is only as reliable as the people who build and maintain it. Every EHR integration, every lab interface, every pharmacy connection depends on engineers who understand both the technology and the clinical workflows it supports. Invest in finding those people, developing their skills, and giving them reasons to stay. The alternative, a revolving door of engineers who leave before they understand your environment, is far more expensive than getting retention right from the start.