Why this list, in this order
"Where do we start with AI agents?" is the most common question from hospital decision-makers we work with. The answer is almost never the most exciting use case in the demo — it is the use case with the cleanest baseline metric, the lowest clinical risk, and the largest pool of comparable hospitals already deploying it. This list is ordered by that pragmatic logic, drawn from public deployments and our own production work. For the strategic context, see our pillar guide on AI agents in healthcare and the strategic adoption framework for hospitals.
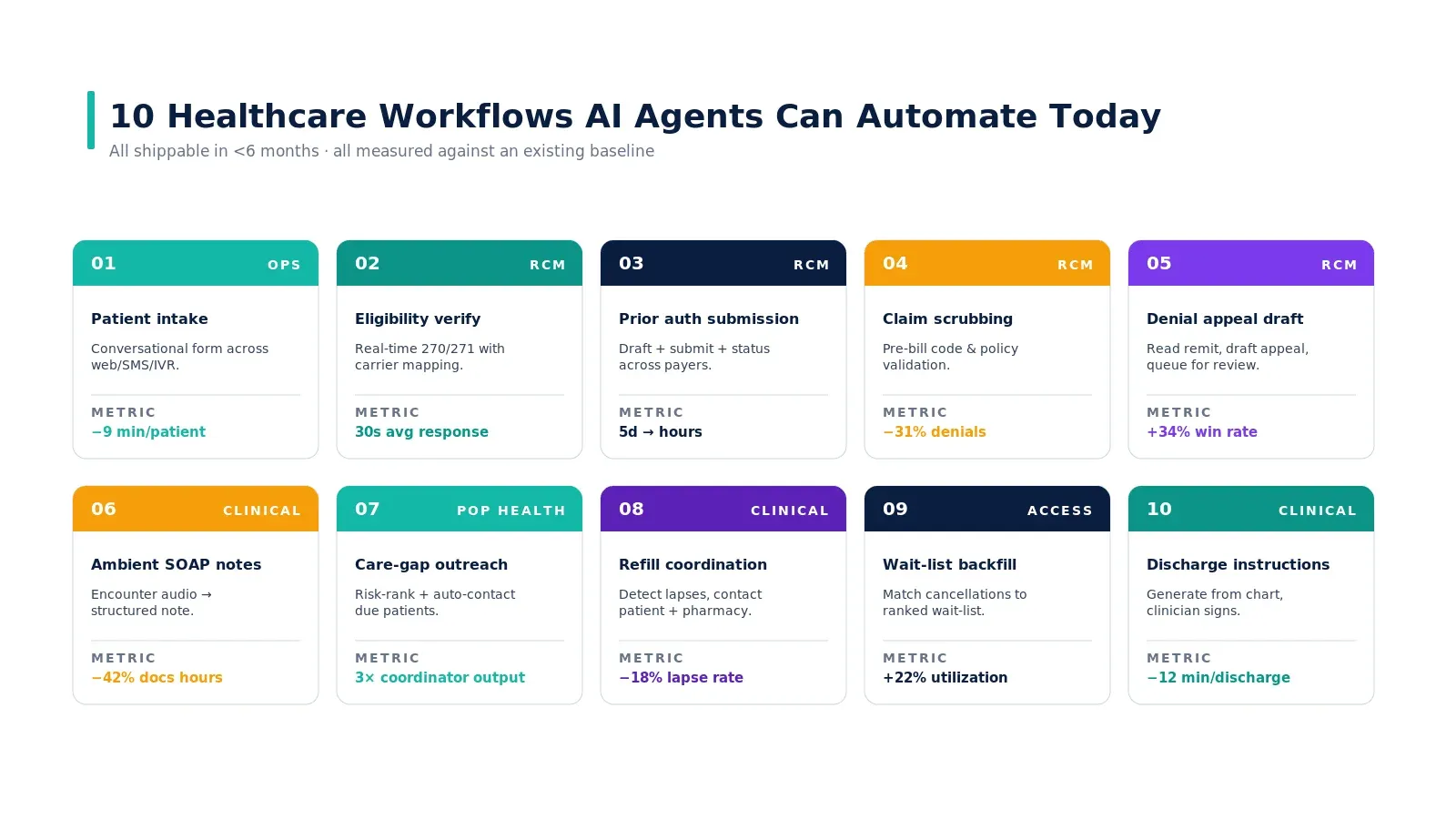
1. Patient intake
A conversational agent captures demographics, visit reason, insurance, and consent across web, SMS, or voice — then validates the data and writes structured FHIR resources directly into the EHR. Front-desk time per patient drops from 12 minutes to 3 minutes of staff review on top of self-service capture. Eligibility is checked in real time at the moment of capture, not three days later.
Why first: the data model is bounded, FHIR R4 has explicit coverage, and the failure surface is administrative rather than clinical. Build path: how to build an AI agent for patient intake automation.
2. Prior authorization
End-to-end PA submission and tracking. The agent reads the chart, maps to payer-specific criteria, drafts a justification letter, submits via the portal or API, monitors status, and drafts an appeal if denied. Cycle time compresses from 5 days to hours; the human stays in the loop for medical-judgment escalations only.
Why second: large dollar impact, repeated workflow, predictable failure modes. Backed by a working case study on eliminating the prior authorization bottleneck and why prior authorization is broken.
3. Eligibility verification
Real-time 270/271 transactions with carrier mapping, payer-specific quirks handled, and coverage gaps surfaced before the patient arrives. Average response time drops to under 30 seconds. Coverage exceptions get queued for staff review with the relevant context attached, not as bare denial codes.
Why critical: it is the cleanest possible first agent. Deep dive: eligibility verification AI agent in 30 seconds.
4. Claim coding assist
Code suggestions from clinical notes, payer-policy validation before submission, and pattern recognition across thousands of claims to surface systemic denial trends. First-pass denial rate typically drops 25–40% in the first six months. The coder reviews the agent's draft instead of building the code set from scratch.
Risk profile: low to medium. Coders should keep final approval authority — the agent is a draft, not a decision.
5. Ambient documentation
The agent listens to the encounter, structures it into the right note format for the specialty, cross-references the patient's existing record for context, and presents a completed draft for physician review. After-hours documentation drops 40%. Note quality improves because the agent captures the full encounter, not just what the physician remembers to type at 9pm.
Risk profile: medium. The clinician retains final sign-off on every note. There is good evidence on burnout reduction — see our case study on agentic AI for clinician burnout.
6. Care navigation and triage
Symptom intake, validated triage protocols (the same the nurse triage line uses), recommendation of appropriate care setting, and direct booking with clinical context pre-populated. Red-flag symptoms (chest pain, suicidal ideation) trigger immediate human escalation. Patient access NPS climbs because routing matches acuity, not whoever picked up the phone.
Risk profile: medium. The agent should never close the loop without escalation in protocols that warrant it.
7. Population outreach
The agent runs continuously against the attributed population. It identifies patients past due on screenings, ED frequenters with the same complaint, lapsed medication refills, and care-gap closures. Outreach is generated and queued for routine cases (appointment reminders, refill check-ins) and pushed to a coordinator only when a conversation is needed. A team of 10 coordinators ends up actively managing what previously required 30.
Risk profile: medium. SDOH and bias monitoring are non-optional here — the wrong stratification logic can entrench inequities at scale.
8. Clinical early warning
Continuous monitoring of vitals, labs, medication administration, and nursing notes for patterns that precede sepsis, respiratory failure, cardiac decompensation, or post-surgical complications. The agent escalates with the specific data pattern that triggered the flag and the recommended response protocol — not a generic alert that gets dismissed.
Risk profile: high. Build only after the governance layer is mature and the QA/safety lane is established. This is not a Phase 1 use case.
How to sequence them

Time-to-value at a glance

The pattern is durable: administrative agents pay back in 3–6 months, clinical decision-support agents in 6–12, true clinical action agents in 12+ if at all on a direct ROI basis (most are outcome-driven). For the dollar-level math, see where AI agents deliver ROI in healthcare.
Real-world examples grounding this list
The use cases above are not theoretical. Mass General Brigham has published outcomes on ambient documentation across 18,000 clinicians. Kaiser Permanente publishes annually on its early-warning system credited with 500 lives saved per year. Mayo Clinic has documented agentic deployments across patient access and revenue cycle. Geisinger has published on conversational digital intake. The ranking and time-to-value bands in this article are calibrated against those published outcomes plus the patterns we have observed across multiple Nirmitee deployments.
Key takeaways
- Start administrative, not clinical. Eligibility, prior auth, intake, and coding are the high-ROI, low-risk first plays.
- Sequence to compound, not to impress. Eligibility → PA → coding stacks because the data flows compound.
- Match risk profile to organizational maturity. Sepsis early warning is not a Phase 1 use case; build governance muscle on administrative wins first.
- Time-to-value is non-linear. Administrative agents return value in months; clinical agents in quarters.
- Same FTE, different work — not headcount cuts. The pattern that works is staff reviewing agent drafts, not staff being replaced.
Call to Action
Want to deploy an AI Agent inside your hospital or healthcare product? Get in touch with our team — we will scope the workflow, governance, and 90-day rollout plan against your own baseline metrics.
Learn more about AI Agents in Healthcare → read the full pillar guide.
Related reading: