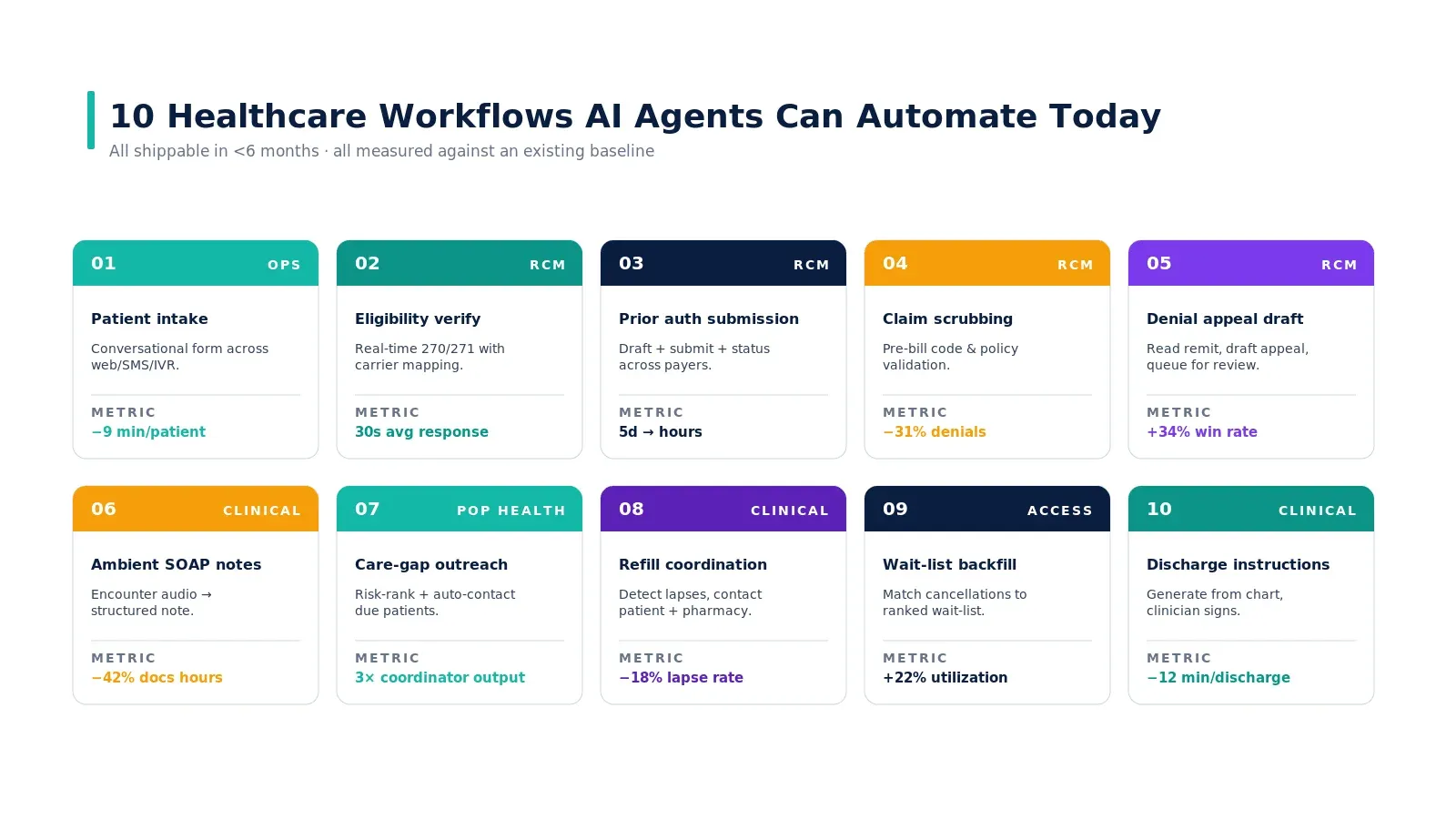
The number that has not moved in a decade
Most U.S. hospitals submit prior authorizations the same way they did in 2015. A nurse builds the request from the chart, types it into a payer portal, waits, and chases the response. Average cycle time is still 3 to 5 business days. The denial rate has barely budged. Layers of automation — RPA, OCR, web forms — have been applied. The number does not move because the bottleneck is not data entry.
This piece is for the revenue cycle leader who has watched two automation projects come and go. We will name the five structural causes that keep PA slow, show where the time actually goes inside the cycle, and identify what AI agents change about each cause. For the broader strategic context, see our guide to AI agents in healthcare.
Five structural causes
Cause 1 — Payer policies are unstructured PDFs
Coverage criteria are buried in 60-page payer policy PDFs that get updated quarterly. Your team cannot reasonably keep up. The result is decisions made on tribal knowledge — what the senior PA nurse remembers from the last update.
What agents change: the agent reads the policy at submission time, extracts the criteria as structured rules, and matches them against the patient's chart. Policy changes are absorbed automatically; tribal knowledge becomes documented evidence.
Cause 2 — Each portal is a different shape
Anthem's portal is not Cigna's portal. Cigna's portal is not Aetna's portal. Aetna's portal is not the regional Blues plan's portal. Your scripted bots break monthly. Your team gets hired partly for their ability to navigate fourteen different web forms.
What agents change: the agent adapts to the portal layout the way a human does. When a payer changes a dropdown, the agent flags the change once and adjusts; the workflow does not need a developer ticket.
Cause 3 — Clinical evidence lives in narrative notes
The ICD code is structured. The H&P that justifies it is narrative. The lab values that support it are structured but spread across encounters. The submission has to pull all three, in the right order, with the right citations.
What agents change: the agent extracts the supporting evidence and cites it inline. The PA letter is grounded in the chart, with quoted excerpts and resource references. Auditability is built in.
Cause 4 — Status updates require human polling
The portal does not push status updates. Your team checks every 24 hours. A request stalled with the payer waiting for additional info sits unanswered for two days because nobody saw the status change.
What agents change: the agent polls status continuously, routes responses to the right team member, and surfaces escalations only when human action is required. The 48-hour stall disappears.
Cause 5 — Appeals get triaged by gut
Of every 100 denials, your team picks 30 to appeal. Win rate sits at ~30%. Which means your team is leaving money on the table — and is also wasting time on appeals they cannot win.
What agents change: the agent ranks appeals by win-likelihood and dollar value, and drafts the appeal letter from chart evidence. The team works the top of the queue and skips the rest. Appeal win rate climbs because effort is concentrated.
Where the 5 days actually go
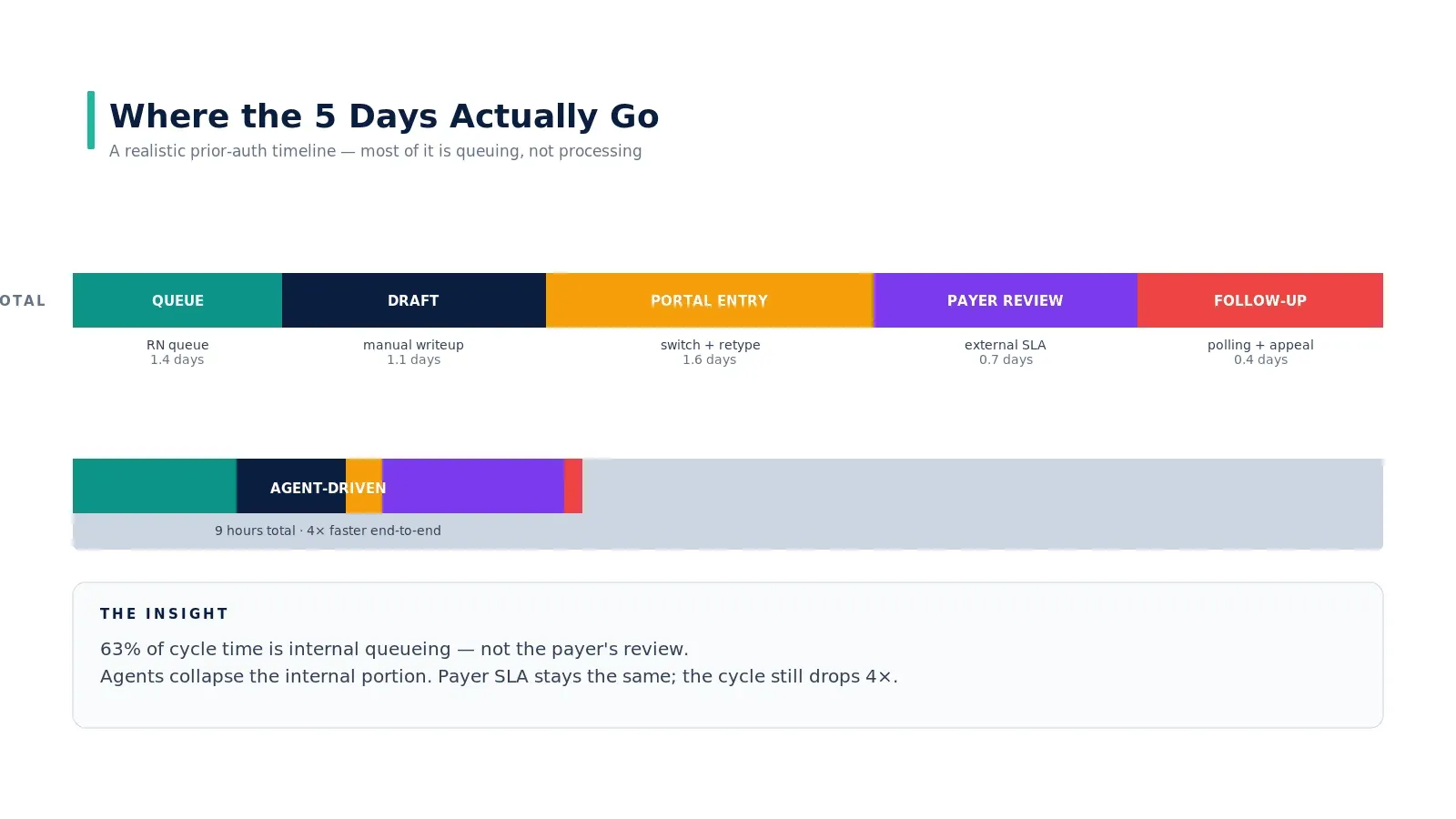
If you decompose a 5-day cycle, here is the distribution most hospitals see:
- 1.4 days in the RN review queue waiting for triage
- 1.1 days drafting the writeup manually
- 1.6 days in portal entry — context-switching across systems and retyping data
- 0.7 days at the payer being reviewed (the part you cannot control)
- 0.4 days following up — polling, appealing, escalating
63% of the cycle is internal queueing. The payer's actual review is less than a day. Agents collapse the internal portion to single-digit hours; the payer SLA stays the same; the cycle still drops 4–8x. This is the math that makes PA the highest-ROI agent deployment for most U.S. hospitals.
Why more automation has not helped

The pattern in the diagram above is the structural answer to "why have we not fixed this already." Each automation layer optimizes data entry. Most PA work is not data entry — it is reading, mapping, drafting, deciding. Static automation cannot close that gap. We unpack the same dynamic at workflow level in why healthcare workflows break and at the technology level in why RPA failed in healthcare and what agentic AI does differently.
What an agent-native PA workflow looks like
- Trigger: a procedure is scheduled. The agent runs immediately, not after the order is placed.
- Eligibility check: 270/271 transaction confirms coverage for the specific procedure or medication.
- Policy retrieval: the agent pulls the relevant payer policy and extracts the criteria for this case.
- Evidence assembly: the agent retrieves chart evidence — diagnosis codes, recent labs, prior treatments, imaging — and matches it to the criteria.
- Justification draft: the agent drafts the medical-necessity letter with inline citations to the chart.
- Human review: a PA nurse approves or revises the draft. This is the step that does not disappear.
- Submission: the agent submits via portal or API and starts polling.
- Response handling: approval → close. Additional info request → agent drafts a response and queues for nurse review. Denial → agent ranks for appeal viability and drafts the appeal if pursued.
The deliverable to the PA nurse is no longer a blank form. It is a draft, an evidence pack, and a recommendation. The nurse spends time on judgment, not on retyping. For the case study showing what this changes at scale, see AI agents eliminating the prior authorization bottleneck.
What does not change — and why that matters
Two things stay the same:
- The payer's SLA. The agent cannot make the payer review faster. Internal cycle compression accounts for the entire improvement until payers themselves automate response.
- The need for clinical judgment on edge cases. Agents handle the 80% of cases that are policy-mappable. The 20% that require physician judgment still go to a physician — but with a draft, not a blank form.
Where to start
If your PA cycle time is 3+ days and your denial rate is above 20%, this is the highest-ROI agent deployment available to you. Sequence it after eligibility verification — the data flows compound. The pattern lands in production in 4–6 months for a single-payer pilot, 9–12 months for full coverage across your top 10 payers.
Companion reading: a strategic adoption framework for hospitals for the operating model, how AI agents reduced claim processing time for the revenue cycle case study, and eligibility verification AI agent in 30 seconds for the upstream piece.
Real-world example
AMA's published 2024 prior authorization physician survey is the single best public reference point on the scale of the problem — 88% of physicians describe PA burden as high or extremely high; 24% report a PA delay led to a serious adverse event for a patient in the prior 12 months. The composite improvement we describe (5 days → 9 hours, denial rate halved) is consistent with results published by Geisinger, Banner Health, and Mayo Clinic on agent-driven PA workflows. The pattern that holds across these deployments: collapse the internal queueing time, leave the payer SLA untouched, and the cycle still drops 4–8x.
Key takeaways
- The bottleneck is judgment, not data entry. RPA, OCR, forms — none move the needle because none read charts and draft letters.
- 63% of cycle time is internal queueing. The payer's actual review is under a day. Fix the internal portion; the cycle drops.
- Agents read payer policy, draft justification, submit, poll, escalate — end to end. The PA nurse approves; she does not retype.
- Appeals get won by concentration, not effort. Rank denials by win-likelihood and dollar value; work the top of the queue.
- Sequence eligibility first. Cleaner coverage data upstream makes the PA agent's job dramatically easier.
Call to Action
Want to deploy an AI Agent inside your hospital or healthcare product? Get in touch with our team — we will scope the workflow, governance, and 90-day rollout plan against your own baseline metrics.
Learn more about AI Agents in Healthcare → read the full pillar guide.
Related reading: