A founder on a healthcare startup subreddit put it bluntly: "We budgeted $80K for our EHR integration. Eighteen months later, we'd spent $220K and still weren't live in a single hospital." The post got hundreds of upvotes. The comments were a graveyard of similar stories — compliance costs nobody warned them about, vendor fees that appeared out of nowhere, security audits that took longer than building the product itself.
This is the reality of healthcare app integration in 2026. Not the sanitized version you'll find in vendor pitch decks, but the actual financial gauntlet that separates healthcare startups that survive from those that run out of runway before their first hospital go-live.
If you are earlier in the journey, start with our complete development guide for building a healthtech app before budgeting integrations.
The numbers are staggering. The FHIR compliance market hit $2.3 billion in 2025 and is projected to reach $8.6 billion by 2036 — growing at 12.7% CAGR. Implementation and integration services account for 45% of that spend. The broader healthcare API market reached $5.4 billion in 2024 and is projected to hit $11.9 billion by 2033. These aren't abstract market projections. They represent the real dollars flowing out of startup bank accounts into the complex machinery of healthcare interoperability.
This guide breaks down exactly where that money goes — phase by phase, line item by line item — so you can plan your budget with precision instead of hope.
The Hidden Cost Iceberg: What Nobody Tells You Before You Start
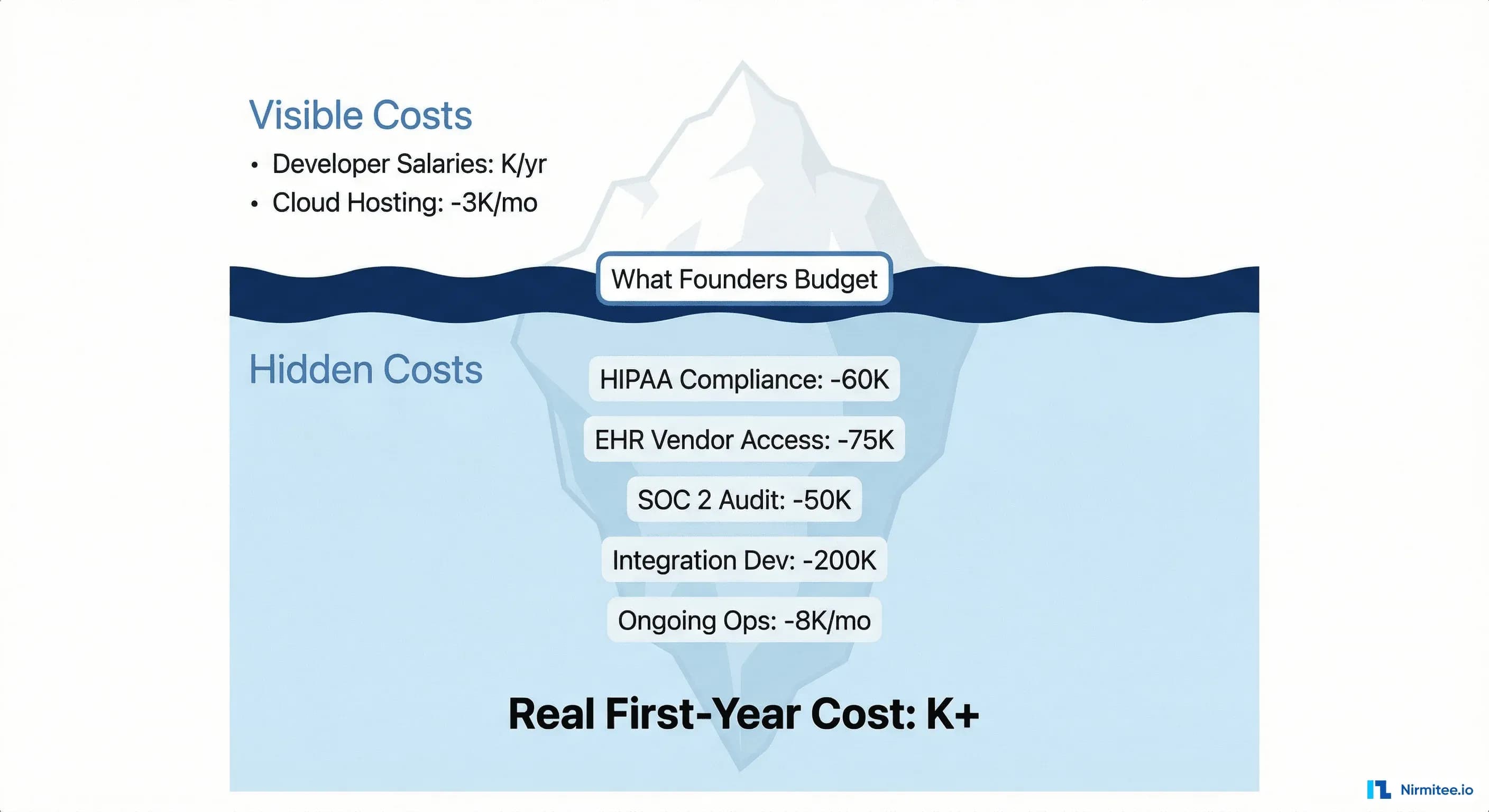
When a healthcare startup founder builds their first integration budget, they typically account for three things: developer salaries, cloud infrastructure, and maybe a HIPAA consultant. That covers roughly 30% of the actual cost.
The iceberg metaphor is overused in business writing, but it's genuinely accurate here. The visible costs — the engineering team writing FHIR API calls — sit above the waterline. Below it lurks a mass of expenses that sink budgets:
- Compliance infrastructure — HIPAA doesn't just mean encrypting data at rest. It means business associate agreements with every vendor, a documented incident response plan, workforce training, and ongoing risk assessments. Startups typically spend $15,000-$60,000 before writing a single line of integration code.
- EHR vendor access fees — Epic doesn't hand out sandbox access for free. Neither does Oracle Health (Cerner). The marketplace listing fees are just the beginning; validation, testing, and per-site go-live support add up fast.
- Security certifications — Hospital procurement teams increasingly require SOC 2 Type II or HITRUST certification. These aren't optional checkboxes. They're gate requirements that can cost $30,000-$100,000 and take 3-12 months.
- Integration testing cycles — Every hospital runs a slightly different EHR configuration. What works in Epic's sandbox may fail in a specific hospital's production environment due to custom workflows, different FHIR resource profiles, or non-standard HL7 v2 message segments.
- Ongoing operational costs — HIPAA-compliant cloud infrastructure alone runs $2,000-$15,000/month, depending on data volume. Add monitoring, on-call support, annual penetration testing, and BAA renewals.
One Series A healthcare startup budgeted $80,000 for their AI-powered patient engagement app but spent $310,000 — nearly 4x their estimate. The gap wasn't bad engineering. It was invisible compliance and vendor costs that no one modeled in the financial plan.
The rest of this guide gives you the model.
Cost Breakdown by Phase: From Zero to Production
Healthcare integration isn't a single expense. It's a sequence of five phases, each with its own cost profile, timeline, and failure modes. Here's what each phase actually costs, based on aggregated data from startup founders, vendor pricing, and industry benchmarks.
Phase 1: Compliance Foundation — $15,000-$60,000
Before you integrate with anything, you need the legal and technical infrastructure that healthcare requires. HIPAA compliance isn't a feature you add later — retrofitting it after launch costs 2-3x more than building it in from day one.
| Line Item | Low Estimate | High Estimate | Timeline |
|---|---|---|---|
| HIPAA risk assessment | $5,000 | $15,000 | 2-4 weeks |
| Privacy & security policies | $3,000 | $10,000 | 2-3 weeks |
| BAA negotiation & legal review | $2,000 | $8,000 | 1-4 weeks |
| HIPAA-compliant infrastructure setup | $3,000 | $12,000 | 1-2 weeks |
| Workforce training program | $1,000 | $5,000 | 1 week |
| Initial penetration test | $5,000 | $15,000 | 2-3 weeks |
| Phase 1 Total | $15,000 | $60,000 | 4-10 weeks |
The biggest mistake founders make: treating HIPAA as a one-time cost. Annual risk assessments, policy updates, and workforce re-training are ongoing requirements. Budget $5,000-$15,000 per year for maintenance.
For a deeper look at how compliance requirements shape your technical architecture, see our guide on healthcare API security, OAuth, SMART on FHIR, and HIPAA compliance.
Phase 2: EHR Vendor Access — $25,000-$75,000
This is where healthcare integration diverges sharply from normal SaaS development. You can't just call an API. You need permission from the EHR vendor, validation of your application, and often a formal marketplace listing.
| EHR Vendor | Program | Entry Cost | Validation/Review | Typical Timeline |
|---|---|---|---|---|
| Epic | Showroom (formerly App Orchard) | $500/yr (Connection Hub) to $25,000+ (Workshop) | Security review, UX review, clinical safety | 3-8 months |
| Oracle Health (Cerner) | CODE Program | $10,000-$25,000 (sandbox + validation) | Functional, security, operations validation | 4-8 months |
| athenahealth | Marketplace Partner | $0 (no interface/setup fees) | Technical review, data quality checks | 2-4 months |
The listing fees are deceptively low. The real costs hide in what comes after:
- Sandbox development time: 2-4 months of engineering effort per EHR vendor, at $15,000-$25,000/month for a dedicated healthcare integration engineer
- Validation loops: Startups report $10,000-$20,000 in engineering time per vendor just for validation iterations — fixing issues flagged during security and UX reviews
- Per-site onboarding: Even after marketplace approval, each hospital deployment requires site-specific configuration. Budget $10,000-$25,000 per hospital for integration effort, clinical workflow mapping, and go-live support
One critical detail: Epic's transition from App Orchard to Showroom in 2024 introduced tiered pricing. The $500/year Connection Hub tier gets you listed, but deeper integration partnerships (Toolbox, Workshop) carry significantly higher fees and longer approval cycles. Plan accordingly.
Related Reading
For more insights, explore our guides on Epic Showroom App Approval Guide for HealthTech Startups and FHIR in Modern Healthcare.
You may also find value in EHR Software Development Guide and Building a Healthtech App.
If you're evaluating which EHR vendors to prioritize, our build vs. buy vs. partner analysis for EHR integration walks through the strategic trade-offs.
Phase 3: Integration Development — $80,000-$200,000
This is the phase founders understand best — and still underestimate. Building a production-grade FHIR client that handles the real-world messiness of clinical data is fundamentally different from consuming a well-documented REST API.
| Line Item | Low Estimate | High Estimate | Notes |
|---|---|---|---|
| FHIR R4 client implementation | $15,000 | $40,000 | Read-only adds ~$12K; read-write adds $25-40K |
| HL7 v2 message parsing (if needed) | $10,000 | $30,000 | Many hospitals still use v2 for ADT, orders, results |
| SMART on FHIR auth implementation | $8,000 | $20,000 | OAuth 2.0 + PKCE + token refresh + scope management |
| Data mapping & transformation | $12,000 | $35,000 | US Core profiles, terminology mapping (SNOMED, LOINC, RxNorm) |
| Multi-EHR testing & QA | $10,000 | $25,000 | Each EHR has different FHIR quirks and edge cases |
| Clinical workflow integration | $15,000 | $30,000 | EHR-embedded UI vs. standalone launch |
| Error handling & retry logic | $5,000 | $10,000 | Healthcare APIs have unique failure modes |
| Healthcare integration engineer (6-9 months) | $90,000 | $135,000 | Based on $180K annual salary, fully loaded |
| Phase 3 Total | $80,000 | $200,000 | 6-14 months |
The engineer salary line item deserves attention. HL7 interface engineers command $104,000-$162,000 annually according to ZipRecruiter's 2026 data, with a median around $128,000. Senior FHIR architects with multi-EHR experience regularly exceed $180,000. These aren't generic backend developers — they need domain-specific knowledge of clinical data models, healthcare terminologies, and EHR vendor quirks.
For a practical approach to building integration architecture that scales across multiple EHR vendors, see our technical guide on building a multi-EHR FHIR facade for Epic, Cerner, and athena.
Phase 4: Security & Audit — $30,000-$80,000
Hospital procurement teams have hardened their security requirements dramatically since 2023. The Change Healthcare breach accelerated what was already a trend: formal security certification is now a gate requirement, not a nice-to-have.
According to FHIR compliance market research, 41% of procurement now requires formal conformance validation. Here's what that costs:
| Certification | Cost Range | Timeline | Who Requires It |
|---|---|---|---|
| SOC 2 Type I | $15,000-$40,000 | 1-3 months | Minimum bar for most health systems |
| SOC 2 Type II | $20,000-$60,000 | 3-6 months (observation period) | Required by major hospital chains, payers |
| HITRUST e1 | $20,000-$70,000 | 1-3 months | Entry-level for startups with limited PHI scope |
| HITRUST i1 | $60,000-$200,000 | 4-9 months | Mid-market, multiple health system customers |
| HITRUST r2 | $150,000-$1,000,000+ | 6-18 months | Enterprise, large health system RFPs |
| Penetration testing (annual) | $5,000-$25,000 | 2-4 weeks | Required for SOC 2, HITRUST, and most vendor security reviews |
The practical advice for seed-stage startups: start with SOC 2 Type II. It's the most widely accepted certification and gives you 6-9 months of runway before hospital procurement asks about HITRUST. Budget $30,000-$50,000 all-in for your first SOC 2 Type II engagement, including readiness assessment, tooling, and the audit itself. HIPAA-regulated buyers rarely accept Type I point-in-time assessments, so go straight to Type II.
Phase 5: Ongoing Operations — $3,000-$8,000/month
The costs that never stop. After your integration is live, you need infrastructure, monitoring, and support to keep it running. AWS costs are a common surprise — startups that start at $500/month for a basic staging environment routinely see bills balloon to $3,000-$5,000/month once they add HIPAA-eligible services, encrypted storage, CloudTrail logging, and dedicated VPC configurations.
| Line Item | Monthly Cost | Annual Cost |
|---|---|---|
| HIPAA-compliant cloud (AWS/Azure/GCP) | $2,000-$5,000 | $24,000-$60,000 |
| Monitoring & alerting (Datadog, PagerDuty) | $300-$800 | $3,600-$9,600 |
| Integration middleware license (if applicable) | $500-$2,000 | $6,000-$24,000 |
| Annual penetration testing | — | $5,000-$25,000 |
| BAA renewals & compliance maintenance | $200-$500 | $2,400-$6,000 |
| On-call support staffing | $500-$1,500 | $6,000-$18,000 |
| Phase 5 Total | $3,000-$8,000 | $36,000-$96,000 |
The operational cost that catches most startups off guard: EHR maintenance. Ongoing EHR integration maintenance typically costs 15-20% of the initial setup investment each year. If your Phase 3 development cost was $150,000, expect $22,500-$30,000 annually just to keep it working as EHR vendors push updates, deprecate API endpoints, and change authentication flows.
The Integration Middleware Decision: Redox vs. Mirth Connect vs. Rhapsody vs. Direct FHIR
One of the highest-leverage decisions you'll make is whether to use integration middleware and which one. This choice affects your cost structure for years. Here's the honest comparison.
| Factor | Redox (iPaaS) | Mirth Connect | Rhapsody | Direct FHIR (Custom) |
|---|---|---|---|---|
| Year 1 cost | $80,000-$150,000 | $30,000-$60,000 | $60,000-$120,000 | $80,000-$200,000 |
| Pricing model | Platform fee + per-transaction | Open-source (commercial since v4.6) + DevOps staff | Per-communication-point license + 22% annual support | Engineering salary + cloud costs |
| Median annual spend | $49,500 (Vendr data) | $20,000-$50,000 (staff + infra) | $40,000-$80,000 | $20,000-$40,000 (maintenance) |
| 3-year TCO | $180,000-$310,000 | $90,000-$210,000 | $140,000-$280,000 | $120,000-$280,000 |
| Time to first integration | 2-4 weeks | 4-8 weeks | 4-6 weeks | 8-16 weeks |
| DevOps burden | Low (managed) | High (self-managed) | Medium (vendor-supported) | High (custom) |
| Multi-EHR support | Strong (250+ health systems) | Manual per-connection | Strong with pre-built adapters | Manual per-EHR |
| FHIR R4 native | Yes | Requires configuration | Yes | You build it |
| Best for | Startups needing speed, <10 integrations | Teams with strong DevOps, cost-sensitive | Mid-market with 10+ hospital connections | Teams with deep FHIR expertise, long-term play |
The key trade-off: Redox gets you to market 4-12 weeks faster but creates vendor dependency and per-transaction costs that scale linearly. Direct FHIR has the highest upfront cost but the lowest marginal cost per additional connection. Mirth Connect was the default "free" option for years, but its shift to commercial licensing since version 4.6 has narrowed the cost gap with Rhapsody.
Important note on Mirth: "open-source" doesn't mean free. You need a dedicated integration engineer ($128K-$162K/year) to build and maintain Mirth channels, plus infrastructure costs. The total cost of Mirth ownership often exceeds what people expect from an open-source tool.
For a detailed technical comparison of integration engines, see our in-depth analysis of Mirth Connect vs. Rhapsody vs. Iguana in 2026.
Why Beautiful UIs Get Rejected by Clinicians
This section isn't about a technology cost — it's about an opportunity cost that routinely burns $50,000+ of development budget.
Healthcare startups often build gorgeous standalone web applications, demo them to hospital administrators who love the design, and then watch the project die when it reaches the clinical workflow committee. The reason: clinicians won't use an app that requires them to leave their EHR.
The workflow alignment problem has three cost implications:
- EHR-embedded UI development: +$30,000-$60,000. Building a SMART on FHIR app that launches within an EHR's iframe, respects the EHR's visual context, and operates within clinical workflows requires fundamentally different design patterns than a standalone web app. You're not designing for beauty — you're designing for a 12-second interaction between patient encounters.
- Clinical workflow mapping: +$15,000-$25,000. You need to shadow clinicians, map their existing workflows, and identify the exact insertion points where your app adds value without adding friction. This is consulting work, not engineering work.
- Redesign after rejection: +$20,000-$50,000. If you build standalone first and then learn the hard way that clinicians won't alt-tab, the cost to refactor into an EHR-embedded app is often higher than building it correctly from the start.
The lesson: budget for clinical workflow integration from day one. Talk to end users — nurses, physicians, medical assistants — before you write a pixel of UI code. The most expensive feature is the one nobody uses.
How to Cut Costs by 60% with a FHIR-First Architecture
Here's the good news. A FHIR-first architecture can reduce your total integration cost by 40-60% compared to the traditional approach of building custom point-to-point integrations for each EHR vendor.
The FHIR-first approach means three things:
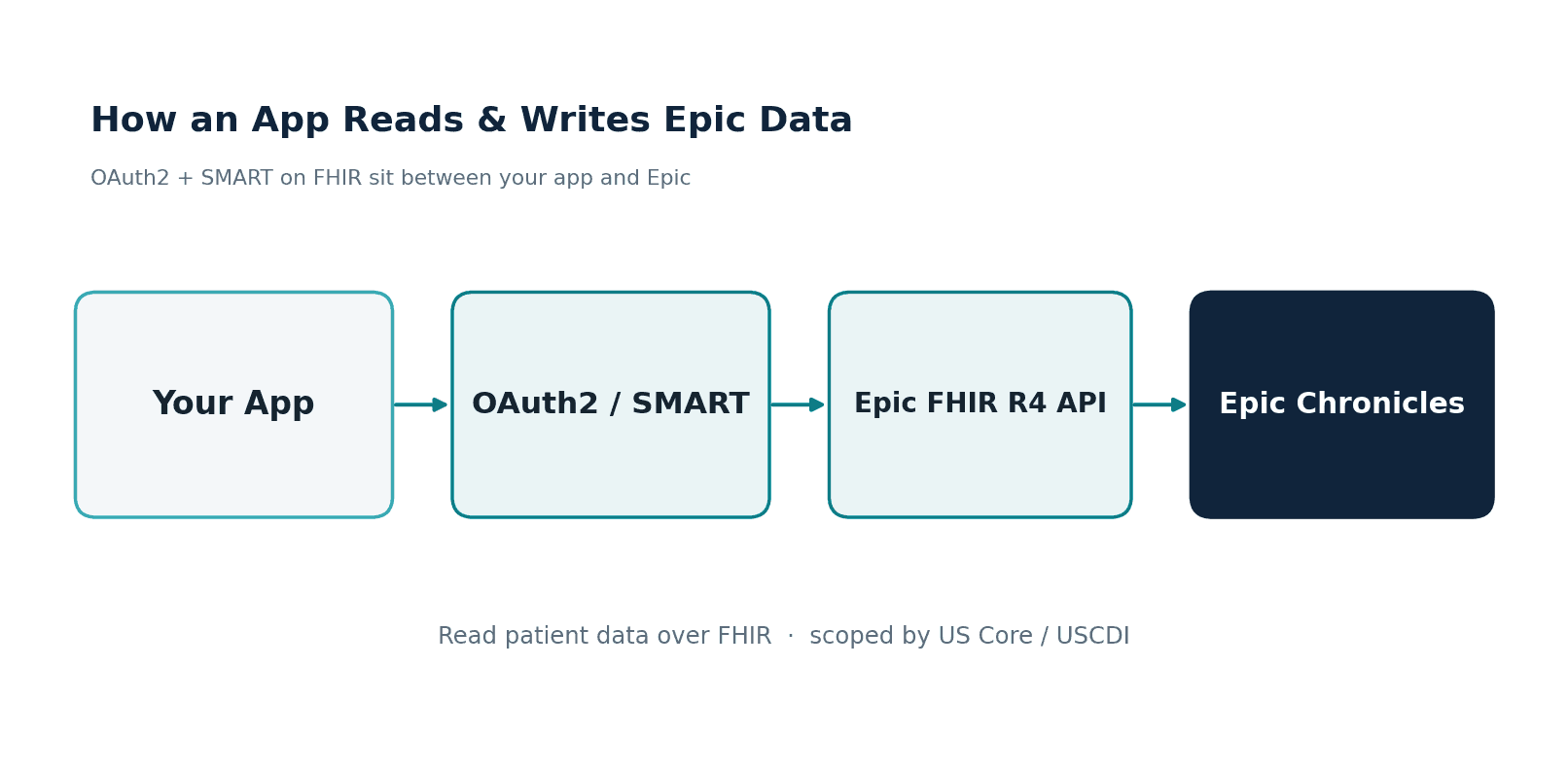
1. Build on SMART on FHIR from Day One
SMART on FHIR (Substitutable Medical Applications, Reusable Technologies) is the standard app launch framework supported by Epic, Oracle Health, athenahealth, and every major EHR vendor. Building a SMART app means:
- One authentication flow — OAuth 2.0 with PKCE, standardized across all EHR vendors. You implement it once.
- One app registration process — Each vendor has its own marketplace, but the underlying protocol is the same.
- EHR-embedded launch — Your app launches within the EHR's workflow, solving the clinician adoption problem from the start.
Cost savings: $30,000-$50,000 by avoiding custom auth implementations per vendor.
2. Use a FHIR-Native Data Model
Instead of building your own internal data model and then writing translation layers to/from each EHR, store your core clinical data in FHIR R4 resources from the beginning. Use US Core profiles as your baseline. This means:
- No data mapping layer per EHR — the data is already in FHIR format
- Terminology services (SNOMED CT, LOINC, RxNorm) are built into the FHIR ecosystem
- ONC certification testing becomes dramatically simpler
Cost savings: $20,000-$40,000 in data mapping and transformation work.
3. Design for Multi-EHR from Day One
The most expensive integration mistake is building for Epic first, then discovering that your architecture makes Cerner and athena integrations equally expensive. A FHIR facade pattern — a thin abstraction layer that normalizes the differences between EHR vendors' FHIR implementations — lets you add new EHR connections at 20-30% of the cost of the first one.
Cost savings: $40,000-$80,000 per additional EHR vendor.
Total cost reduction with FHIR-first: a startup that would spend $300,000+ on traditional point-to-point integrations across three EHR vendors can achieve the same coverage for $120,000-$180,000 with a FHIR-first architecture. That's a 40-60% reduction that compounds with every additional hospital connection.
The 12-Month Integration Budget Template
Theory is useful. A spreadsheet is better. Here are two budget templates — one for a seed-stage startup with limited capital, and one for a Series A company with a mandate to integrate with multiple EHR vendors.
Seed-Stage Budget ($150K-$250K, 12 months)
Assumption: Single EHR vendor (Epic), one FHIR-based integration, team of 2-3 engineers, SOC 2 Type II certification, HIPAA-compliant cloud infrastructure.
| Month | Activity | Cost | Running Total |
|---|---|---|---|
| 1-2 | HIPAA risk assessment, policies, BAAs | $15,000 | $15,000 |
| 2-3 | HIPAA-compliant infra setup (AWS/GCP) | $8,000 | $23,000 |
| 2-4 | Epic Showroom registration + sandbox access | $5,000 | $28,000 |
| 3-8 | FHIR client dev + SMART on FHIR auth (1 engineer, 6 months) | $90,000 | $118,000 |
| 5-8 | SOC 2 Type II readiness + audit engagement | $35,000 | $153,000 |
| 7-9 | Epic validation + testing iterations | $15,000 | $168,000 |
| 9-10 | Penetration test | $10,000 | $178,000 |
| 10-12 | First hospital go-live (site-specific config + support) | $15,000 | $193,000 |
| 1-12 | Cloud infrastructure ($2,500/mo avg) | $30,000 | $223,000 |
| 1-12 | Monitoring, tooling, misc | $7,000 | $230,000 |
| 12-Month Total | $193,000-$250,000 |
What this gets you: One EHR integration (Epic), FHIR R4 read/write, SMART on FHIR launch, SOC 2 Type II certified, live in one hospital.
Series A Budget ($350K-$550K, 12 months)
Assumption: Multi-EHR (Epic + Oracle Health + athena), FHIR facade architecture, team of 4-5 engineers, SOC 2 Type II + HITRUST e1, integration middleware (Redox or Mirth), 3-5 hospital go-lives.
| Month | Activity | Cost | Running Total |
|---|---|---|---|
| 1-2 | HIPAA compliance program (assessment + policies + training) | $25,000 | $25,000 |
| 1-3 | HIPAA-compliant infra + CI/CD pipeline | $15,000 | $40,000 |
| 2-4 | EHR vendor registrations (Epic + Oracle + athena) | $30,000 | $70,000 |
| 2-8 | FHIR facade + multi-EHR integration (2 engineers, 7 months) | $180,000 | $250,000 |
| 3-6 | Integration middleware setup (Redox or Mirth) | $40,000 | $290,000 |
| 5-9 | SOC 2 Type II + HITRUST e1 | $65,000 | $355,000 |
| 7-10 | Multi-vendor validation + testing | $35,000 | $390,000 |
| 8-10 | Penetration test + vulnerability remediation | $15,000 | $405,000 |
| 9-12 | Hospital go-lives (3-5 sites @ $15K avg) | $55,000 | $460,000 |
| 1-12 | Cloud infrastructure ($4,000/mo avg) | $48,000 | $508,000 |
| 1-12 | Monitoring, middleware license, tooling | $22,000 | $530,000 |
| 12-Month Total | $380,000-$550,000 |
What this gets you: Three EHR integrations, FHIR facade architecture, SOC 2 Type II + HITRUST e1 certified, live in 3-5 hospitals, scalable to 20+ connections.
For guidance on scaling beyond these initial deployments — the per-site costs, the operational challenges, and the common pitfalls — see our guide on scaling EMR integrations after MVP and hospital onboarding.
Planning Your Integration Budget
Healthcare app integration is expensive, but it's not unpredictable — not if you plan for the real costs instead of the ones you hope for. The founders who survive this process share three traits: they budget for compliance from day one, they choose their EHR vendor strategy before writing code, and they build on standards (FHIR R4, SMART on FHIR, US Core) rather than proprietary shortcuts.
The numbers in this guide aren't worst-case scenarios. They're the actual costs that successful healthcare startups pay. The difference between the startup that spends $220K and fails and the one that spends $220K and succeeds isn't the total budget — it's whether that budget was allocated to the right things in the right order.
Three immediate next steps:
- Audit your current budget against the phase-by-phase breakdown above. Identify which costs you've accounted for and which you haven't.
- Choose your integration architecture — the middleware decision and FHIR-first vs. point-to-point choice will determine your cost trajectory for years. Our CTO framework for evaluating healthcare interoperability vendors can help structure that decision.
- Start compliance early. HIPAA and SOC 2 are on the critical path to your first hospital sale. Every month you delay them is a month added to your sales cycle.