If you are sizing a healthcare integration budget for 2026, the question that keeps surfacing in vendor calls and CFO reviews is deceptively simple: how much does a single Mirth Connect interface actually cost to build? The honest answer is "it depends" — but "it depends" is not a number you can put in a board deck. This guide replaces guesswork with a defensible pricing matrix.
We have built, audited, and re-platformed hundreds of Mirth Connect interfaces across hospital systems, digital health startups, labs, and payers. The numbers in this post come from real project ledgers, not pulled from thin air. Whether you are a five-clinic group trying to decide between two RFP responses, or a 300-bed hospital scoping a full EHR integration program, you will leave with a budget you can actually defend.
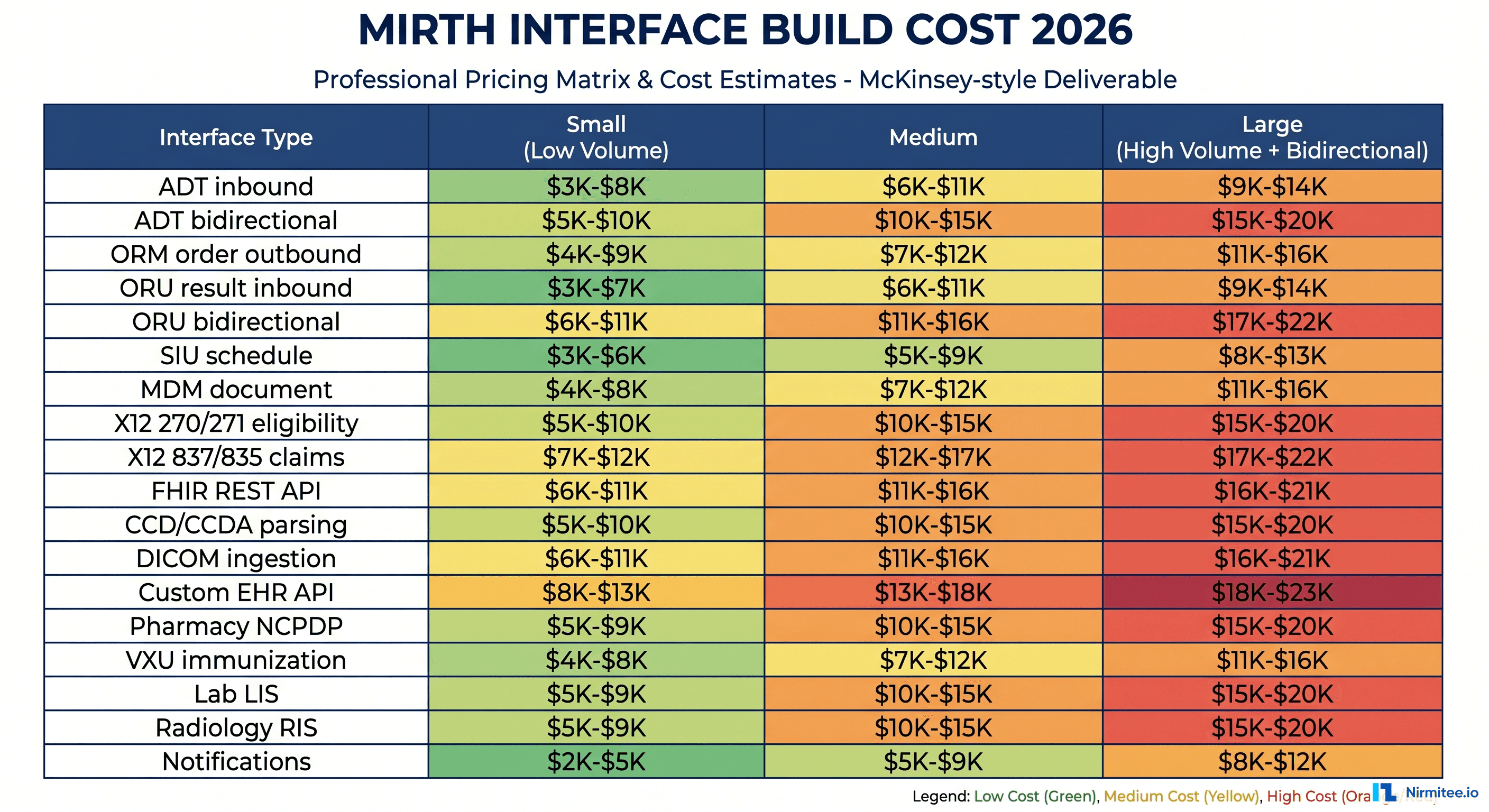
The 2026 Mirth Interface Pricing Matrix at a Glance
Before we get into the cost drivers, here is the headline pricing matrix. These are build costs — not annual maintenance, not licensing, not infrastructure. Just the engineering work to design, develop, test, and deploy a single interface into production using Mirth Connect as the integration engine.
| Interface Type | Direction | Small / Low Volume | Medium | Large / High Volume |
|---|---|---|---|---|
| ADT (Admit, Discharge, Transfer) | Inbound, one-way | $3K-$5K | $5K-$7K | $7K-$8K |
| ADT bidirectional | Two-way | $8K-$10K | $10K-$13K | $13K-$15K |
| ORM (Order Message) | Outbound | $5K-$6K | $6K-$8K | $8K-$10K |
| ORU (Result, Inbound) | Inbound | $5K-$6K | $6K-$8K | $8K-$10K |
| ORU bidirectional with corrections | Two-way | $12K-$15K | $15K-$20K | $20K-$25K |
| SIU (Scheduling) | Inbound/Outbound | $6K-$8K | $8K-$10K | $10K-$12K |
| MDM (Medical Document Management) | Inbound/Outbound | $8K-$10K | $10K-$12K | $12K-$15K |
| VXU (Immunization) | Outbound to registry | $5K-$7K | $7K-$10K | $10K-$14K |
| X12 270/271 (Eligibility) | Bidirectional | $10K-$13K | $13K-$17K | $17K-$20K |
| X12 837/835 (Claims/Remit) | Bidirectional | $15K-$20K | $20K-$25K | $25K-$30K |
| FHIR REST API endpoint | Bidirectional | $8K-$12K | $12K-$16K | $16K-$20K |
| CCD / C-CDA document parsing | Inbound | $10K-$15K | $15K-$20K | $20K-$25K |
| DICOM ingestion | Inbound | $12K-$15K | $15K-$20K | $20K-$25K |
| NCPDP (Pharmacy) | Bidirectional | $10K-$14K | $14K-$18K | $18K-$22K |
| Lab LIS interface (HL7 v2) | Bidirectional | $8K-$10K | $10K-$14K | $14K-$18K |
| Radiology RIS interface | Bidirectional | $10K-$13K | $13K-$17K | $17K-$22K |
| Custom EHR API (Epic, Cerner, Athena) | Bidirectional | $15K-$25K | $25K-$38K | $38K-$50K |
| Real-time notifications/event bus | Outbound | $6K-$9K | $9K-$13K | $13K-$18K |
How to read this table: "Small" means low message volume (under 1,000 messages/day), a single source and destination, no complex business rules, and standard mappings. "Large" means high volume (over 50,000 messages/day), multiple endpoints, custom code mappings, full error handling, and bidirectional flow with reconciliation logic. Most real-world interfaces land in the Medium column. A useful rule of thumb: doubling the message volume rarely doubles the cost, but adding bidirectionality usually does.
These ranges assume you are working with a vendor who already has Mirth experience. If you are paying a team to learn Mirth on your project — common with generalist software shops — add 30 to 50 percent for ramp-up.
What Actually Drives Mirth Interface Cost
The dollar ranges above swing for predictable reasons. If you understand the six drivers below, you can self-estimate any interface in 30 seconds.
1. Bidirectionality (+50% to +100%)
A one-way ADT feed from your Epic source into a downstream system is roughly half the cost of a bidirectional ADT exchange. Bidirectional flow forces you to handle acknowledgments (ACK/NACK), reconciliation when messages cross in flight, idempotency on the receiving end, and conflict resolution when both sides update the same record. Every one of those concerns is a code path, a test case, and a failure mode you have to design around.
2. EHR Vendor Complexity (Epic Premium: +30%)
Not all EHRs are priced equal. Epic interfaces typically cost 30 percent more than equivalent ones into Meditech, Athena, or eClinicalWorks. The reasons are real: Bridges and Chronicles configuration, the need for Epic-side analyst sign-off, Interconnect/Hyperspace specifics, and limited sandbox access without a paid relationship. Cerner (now Oracle Health) sits between Epic and the rest — somewhat less expensive than Epic, but still requires CCL knowledge and tight change-control coordination.
3. Message Volume (+20% to +40%)
Volume changes the engineering, not just the runtime. A 1,000-messages-per-day interface can live on a single Mirth channel with synchronous processing. A 100,000-messages-per-day interface needs queue tuning, JVM heap sizing, database connection pools, batched commits, dead-letter handling, and a real high-availability setup. The build itself is more careful, and that care costs money.
4. Code Mapping Complexity (+25%)
LOINC, SNOMED CT, RxNorm, ICD-10, local mnemonics — the more code systems an interface has to translate between, the more lookup tables, transformation rules, and edge-case handling you need. A simple ORU that passes through codes is cheap. An ORU that has to map proprietary lab codes to LOINC, then re-map LOINC to the destination's local dictionary, is materially more expensive. Curating and validating those mappings is often more work than the integration itself.
5. Edge Cases and Corrections (+30%)
Real healthcare data is messy. Patients are merged, results are amended, orders are cancelled mid-flight, demographics change retroactively, and discharges sometimes happen before admissions are posted. An interface that handles only the "happy path" is half-built. The other half — corrections (HL7 RPT_NEW versus RPT_CORR), cancellations, merges, deletes, retroactive updates — is where projects that look on-budget become "we need another sprint."
6. Compliance and Audit Requirements (+15%)
If your interface touches PHI under HIPAA — which it always does — you need audit logging that survives a real auditor's scrutiny, TLS configuration that meets your security team's standards, message-level encryption at rest, role-based access for the Mirth admin UI, and documentation that maps controls to your policies. None of that is hard. All of it takes time.
The Interface Complexity Scoring Rubric
If you want to estimate an interface in under five minutes, score it against five categories on a 1-to-5 scale, sum the result, and look up the cost band. We use this rubric for every Mirth proposal we write, and it correlates well with the final invoice.
| Category | Score 1 (Simple) | Score 3 (Moderate) | Score 5 (Complex) |
|---|---|---|---|
| Message Volume | <1,000/day | 10,000-50,000/day | >100,000/day |
| Bidirectionality | One-way | Two-way, simple ACK | Two-way w/ reconciliation |
| Code Translation | Pass-through | 1-2 code systems | 3+ systems, custom maps |
| Source/Dest EHR | Modern API, good docs | Standard HL7 v2 | Epic / Cerner / legacy |
| Compliance | Internal-only | HIPAA standard | HIPAA + audit + 42 CFR Part 2 |
Total score → cost band:
- 5-10: Simple — $3K to $8K
- 11-15: Moderate — $8K to $18K
- 16-20: Complex — $18K to $35K
- 21-25: Enterprise — $35K to $75K (custom EHR, X12 claims, DICOM at scale)
This is a starting point, not a contract. The rubric undercounts risks like immature vendor APIs, unstable source systems, and organizational change-management friction. Always carry a 15 to 25 percent contingency.
Three Worked Examples (Real Project Budgets)
Aggregating individual interfaces into a program budget exposes scaling effects you cannot see at the line-item level. Here are three scenarios drawn from actual engagements, with names and numbers anonymized.
Scenario 1 — The 5-Interface Clinic Group ($25K to $50K, 3 months)
A four-location primary care group migrating from a legacy practice management system to a modern EHR. They need: two ADT feeds (one inbound from registration, one outbound to the patient portal), one ORU lab result inbound, one SIU scheduling sync with a third-party booking app, and one billing handoff to their RCM vendor.
None of the interfaces is individually complex. Volumes are well under 5,000 messages/day total. The cost driver is project overhead — kickoff, requirements gathering, testing coordination across three external vendors, and go-live support. We typically budget a single senior integration engineer at 50 percent allocation for three months, plus 10 percent for a tech lead. Total landed cost: $25K on the low end, $50K if Epic or a tricky payer is in the mix.
Scenario 2 — The 25-Interface Community Hospital ($150K to $300K, 6 months)
A 180-bed regional hospital implementing a new HL7 backbone to replace a tired legacy engine. Twenty-five interfaces: eight ADT, six ORU, four SIU, three X12 (270/271 plus 837), and four custom integrations to specialty systems (cardiology, radiology, anesthesia, pharmacy).
Here the team scales: two senior engineers, one mid-level engineer, one QA, and a part-time technical project manager. Six months from kickoff to last interface in production. The X12 claims interface alone is a $25K to $30K line item; the custom radiology RIS integration adds another $20K. Total: $150K to $300K depending on EHR vendor mix and how much of the legacy mapping documentation survived the transition.
Scenario 3 — The 75-Interface Regional Health System ($400K to $800K, 12 months)
A multi-hospital system standardizing on a single integration platform across three facilities, two ambulatory networks, and a shared lab. Seventy-five interfaces including 20 ADT (each facility, each downstream), 18 ORU, 10 SIU, 8 X12, 12 FHIR endpoints feeding population health and analytics, and 7 DICOM/imaging integrations.
This is a 12-month, 12-person program. Three senior engineers, four mid-level, two QA, a dedicated project manager, an integration architect, and a part-time security lead. Healthcare interoperability at this scale is also a governance exercise — naming conventions, code mapping ownership, runbook standards, on-call rotations. The interface build itself is roughly 60 percent of the budget; the other 40 percent is platform engineering, monitoring, and operational readiness.
Total Cost of Ownership — Why Build Cost Is Less Than Half the Story
The biggest mistake we see in Mirth budgeting is treating an interface as a one-time capital expense. It is not. A production interface is a piece of software that lives in your environment for years. It accrues maintenance, monitoring, updates, and incident response cost every single month.
Our rule of thumb for three-year TCO:
| Cost Component | % of Year 1 Build Cost (Annual) | Notes |
|---|---|---|
| Maintenance and bug fixes | 15-20% | Schema drift, vendor API changes, edge cases discovered in prod |
| Monitoring and observability | 5-10% | Tooling + on-call coverage. See monitoring guide |
| Mirth version upgrades | 5-8% | Major version changes every 12-18 months |
| Compliance and security audits | 3-5% | Annual HIPAA review, penetration test remediation |
| Incident response | 3-7% | Higher for high-volume or claims interfaces |
Add these up: a Mirth interface that costs $10K to build will typically cost another $3K to $5K every year to keep running. Over three years, that is a 90 to 150 percent multiplier on the build cost.
For a 25-interface hospital program with a $200K build budget, you should plan for $60K to $100K/year in ongoing operations — a $380K to $500K three-year TCO. Skipping the ops budget is the single most common reason mid-sized integration programs run into trouble in years two and three.
The shift in Mirth's commercial licensing model also matters here. If you have not already, read our take on the Mirth Connect commercial transition and the alternatives landscape. License cost was historically zero; for some configurations in 2026 it is not.
Build vs Buy — When Mirth Engineering Should Be Outsourced
Should you hire engineers to build interfaces in-house, outsource the program to a Mirth specialist, or run a hybrid? Cost is one input — capability and timeline matter more. Use the decision tree above, or work through these questions:
Build in-house if:
- You have already built more than five production Mirth interfaces successfully
- You have at least one staff engineer with deep HL7 v2 experience (not just Java)
- Your timeline is over six months and you have headcount approved
- You will maintain the interfaces in-house long term (3+ years)
- You are willing to invest in ongoing training as standards evolve (FHIR R5, USCDI v4, etc.)
Consider a hybrid model if:
- You have one or two in-house integration engineers but the workload is bursty
- Your first wave of interfaces is needed in under 90 days, but steady state is manageable
- You want to retain platform ownership but offload specialized work (X12, DICOM, FHIR)
- You need 24x7 monitoring coverage that your team cannot staff alone
Fully outsource if:
- You have never built a Mirth interface before
- Your timeline is under 90 days and the program is more than three interfaces
- You do not plan to keep integration engineers on permanent payroll
- You are migrating between integration platforms (BizTalk, Rhapsody, Iguana → Mirth) and need expertise across both sides — see our comparison guide
Outsourced Mirth engineering in 2026 is priced at $125 to $200/hour for North American teams and $50 to $90/hour for offshore-blended teams with healthcare specialization. Per-interface fixed-bid pricing from specialist shops (including us) is typically 15 to 25 percent more efficient than time-and-materials billing on the same scope.
The Hidden Costs Most RFPs Forget
Even careful buyers overlook line items that materially change the program cost. If your RFP does not surface these, ask the vendor to itemize them separately:
- Integration test environments. Mirth Connect needs at least three environments (dev, UAT, prod). Mirroring vendor sandboxes (Epic, Cerner) sometimes incurs subscription fees.
- VPN and network connectivity. Site-to-site VPN setup with each partner organization runs $2K to $5K per partner and frequently lands on the integration team's plate.
- Code mapping data and licenses. Some code systems (SNOMED CT international edition) require paid licenses for commercial use.
- Test data generation. Synthetic but realistic HL7 messages, claims, and CCD documents are surprisingly hard to source. Budget $5K to $15K for a serious test corpus.
- Documentation and runbooks. A 50-page operational runbook per critical interface is non-negotiable for hospital-grade systems. Bake 10 percent of build cost into documentation explicitly.
- Change management with source systems. Every Epic upgrade can break ADT field mappings. Every CMS X12 companion guide update can break claims. Plan for two to four "vendor update" cycles per interface per year.
- Performance tuning at production scale. If you are not tuning JVM heap, channel queue settings, and database pools, your interfaces will degrade once real traffic hits. See our deep dive on performance tuning at 10,000 messages/hour.
Pricing Calculator — Estimate Your Program in Five Minutes
If you want a fast number to put in front of your CFO, walk this five-step calculator:
- List every interface (source system → message type → destination). Aim for completeness, not perfection.
- Score each interface 5 to 25 using the complexity rubric above. Use Medium-column pricing when in doubt.
- Sum the per-interface build costs. That is your raw build number.
- Add 30 percent for program overhead — kickoff, architecture, integration testing, deployment, project management.
- Add 15 to 25 percent contingency for discovery-stage scope additions.
That total is your year-1 capital cost. For three-year TCO, add 90 to 150 percent of that figure for ongoing operations. You will be within 10 to 15 percent of what a specialist vendor would quote you — close enough to defend the budget internally before you go to RFP.
Common Mistakes That Inflate Mirth Budgets by 50%+
Patterns we see again and again in audits of stalled or over-budget Mirth programs:
- Treating Mirth as a no-code tool. The drag-and-drop UI suggests Mirth interfaces require minimal engineering. They do not. The cheap-looking interfaces in the matrix above still assume a senior engineer is writing JavaScript transformers, debugging acks, and reasoning about idempotency.
- Skipping the architecture phase. Channel naming conventions, error queues, retry strategies, monitoring hooks, and shared libraries — all should be designed up front, before the first interface ships. Retro-fitting these is twice the cost.
- Underestimating testing. Mirth testing typically consumes 30 to 40 percent of project hours when done correctly. Programs that allocate 10 percent are the ones that miss the go-live date.
- Confusing "Mirth-certified" with "Mirth-experienced." Certification is a knowledge check. Real experience comes from production incidents. Ask any vendor to walk you through a major outage they resolved — that conversation reveals more than a resume.
- Building without monitoring. Read our piece on production-grade Mirth monitoring. Interfaces without monitoring are interfaces that fail silently — and silent failures are the most expensive failures in healthcare.
Get a Same-Day Mirth Interface Cost Estimate
Send us your interface list — source system, message type, destination, rough volume — and we will return a defensible cost estimate within one business day. No sales call required. We will also share a sample statement of work and the pricing calculator spreadsheet so your team can iterate internally.
If you would rather book a 30-minute working session to whiteboard your program, our integration architects do that too. Talk to our team with a one-line description of your environment and we will get back the same day.
Where to Go Deeper
This pricing guide is the budgeting companion to our broader Mirth content library:
- Building a robust HL7 interface engine with Mirth Connect — engineering-level architecture deep dive
- Top 10 Mirth Connect integration failures — what goes wrong, and what it costs to fix
- Mirth Connect security hardening, Log4j, and HIPAA compliance — controls and audit prep
- Healthcare integration architecture with Mirth and Kafka — when to pair Mirth with a streaming layer
- BridgeLink and the open-source Mirth fork landscape — license-driven alternatives
Need expert help scoping or building Mirth integrations? Explore our Healthcare Interoperability Solutions for end-to-end integration engineering, or our Healthcare Software Product Development services for full-stack clinical platform builds. Talk to our team to get a same-day estimate on your interface program.


